
Abstract
Objective:
This paper reports patterns of health service utilisation in the second Australian national survey of psychosis corresponding with changes in available services of this period.
Method:
Semi-structured interviews were carried out of an age-stratified random sample of adults who screened positive for psychosis. Multivariate logistic regressions were used to identify predictors of service use for a sample of 1825 individuals.
Results:
Use of psychiatric inpatient services was associated with higher symptom levels, suicidal ideation, poor social functioning and younger age. High users of emergency mental health services similarly reported higher symptom levels, poor functioning and younger age, and also reported being married or in a de facto relationship. Recipients of general practitioner services had greater anxiety symptoms and suicidal thoughts, fewer negative symptoms, single marital status and English as their first language. Rehabilitation service use was associated with greater anxiety symptoms, unemployment, younger age of illness onset, living alone and having no dependent children living at home. Last, outpatient/community services were more frequently used by younger people with good premorbid adjustment, hallucinations and a less severe course of illness.
Conclusions:
Service utilisation patterns vary with the clinical and socio-demographic features of those who use them – inpatient and emergency service users being similar in such features and differing from users of other services. Comparison with the first national survey of psychosis revealed a significant decline in acute inpatient service use and a substantial increase in the use of outpatient/community and rehabilitation services over the past 10 years.
Introduction
Mental disorders are among the leading causes of morbidity (Andrews et al., 2001; Dewa et al., 2004; Insel, 2008; Vos et al., 2012; World Health Organization, 2008) and of these the psychoses are the most costly per capita (Andrews et al., 2004; Carr et al., 2003). In Australia, the cost of psychotic disorders has been estimated at 1.2% of total health expenditure. While inpatient service use accounts for a large share of mental health care expenditure (Carr et al., 2003; Lang et al., 1997), services have come to focus more on community-based care and rehabilitation concomitant with the decline in hospital bed numbers (Pezzimenti et al., 2006; Tansella et al., 2006). Detailed analysis of service utilisation patterns and their correlates in psychosis is a necessary prerequisite for assisting resource allocation decisions and improving the efficiency of services. Moreover, it has been recommended that the scope of mental health service research be widened to encompass a multilevel perspective, including patient characteristics, symptom severity, perceived needs, and the socio-economic and cultural environment (Becker and Kilian, 2006).
In 1995, Andersen developed a behavioural model for identifying factors associated with the utilisation of mental health services (Andersen, 1995). This classifies predictors of service use into three categories: predisposing, enabling, and needs-related. Predisposing factors are individual characteristics that exist prior to the illness (e.g. socio-demographic profile); enabling factors refer to various features that influence care delivery and attitudes toward care (e.g. income, social support); and needs-related factors include physical and mental health profiles (e.g. symptom severity and cognitive impairment).
Research on potential determinants of service use in various settings has already demonstrated that needs-related factors are most closely associated with mental health service use (Leaf et al., 1985); in particular, the more robust predictors seem to be level of functioning, symptom patterns and comorbidity (Lay et al., 2006; Oiesvold et al., 2000).
Predisposing factors account for another important proportion of variance in mental health service use, especially age, sex, marital status, education and race/ethnicity. For example, individuals with more education use mental health services more often (Leaf et al., 1985; Vasiliadis et al., 2007). Older individuals are less likely to use emergency services (Kessler et al., 2001; Wang et al., 2005). Females are the most frequent users of services for mental health, especially general practitioners (GPs) (Carr et al., 2003; Narrow et al., 2000; Putkonen et al., 2011; Uebelacker et al., 2006), and there are significant differences in health care utilisation by marital status with single, divorced or widowed persons using services more frequently (Moreno-Küstner et al., 2011). Race and ethnicity are also reported to contribute to mental health service use (Bhui et al., 2003; Mohan et al., 2006).
Studies focusing on enabling factors suggest that various social risk factors (e.g. low income, lack of social support) increase the chances of repeated mental health service use. In particular, social isolation, homelessness and unemployment are highly correlated with admission rates (Dhossche and Ghani, 1998). Individuals of higher socio-economic status tend to use all services more assiduously, particularly mental health care (Alegria et al., 2000; Hendryx and Ahern, 2001; Wang et al., 2000).
An important limitation of previous research is that it has tended to focus on a particular subset of determinants (e.g. enabling versus needs-related) or used a limited set of dependent variables (e.g. inpatient versus outpatient or community services) within the same study. A more comprehensive approach that can account for the likelihood of using different types of services while controlling for the effects of a large set of potential determinants is rare. Comparatively few studies have looked simultaneously at the relative impact of predisposing, enabling and needs-related factors within the same design and across different types of services. The present study sought to address those shortcomings in identifying determinants of health service utilisation in the second Australian national survey of psychosis (Morgan et al., 2011, 2012). Although primarily a descriptive study, in accordance with previous research, we predicted that needs-related factors would show the strongest associations with mental health service use.
Methods
A detailed account of the design and method for the second Australian national survey of psychosis has been provided elsewhere (Morgan et al., 2012). The survey was a population-based, representative sample of people with psychosis in contact with mental health treatment services. All mental health service users in the catchment sites were screened for psychosis, with participants randomly selected for interview from those who were screen-positive. The study identified three mutually exclusive groups: (1) people in contact with specialised public sector mental health services of all kinds during the census month; (2) people not in contact with these services in the census month but in contact with non-government organisations (NGOs) funded to support people with mental illness in that month; and (3) people not in contact with public specialised mental health services or NGOs in the census month but in contact with public specialised mental health services in the 11 months prior to census.
Approval was obtained from relevant institutional human research ethics committees and the participants gave informed consent before being interviewed.
Measures
The survey employed a semi-structured interview covering, inter alia, psychopathology, substance use, service utilisation, level of functioning, education, employment, accommodation, and socio-demographic variables. The instrument is described in detail, together with a description of sampling frame, selection criteria and methodology, by Morgan et al. (2012). Diagnostic assessment was made using the Diagnostic Interview for Psychosis-Diagnostic Module (DIP-DM) (Castle et al., 2006). A computer algorithm provides diagnostic classification in accordance with the International Classification of Diseases (ICD)-10, the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) and other criteria on the basis of the DIP-DM scores, thus reducing subjective bias in the interpretation of symptoms and signs. DIP-DM has excellent inter-rater diagnostic agreement (averaged pairwise agreement of 0.94 for ICD-10 diagnoses).
Outcome measures included: inpatient admissions for mental and physical health problems; outpatient community clinic attendances for mental and physical health problems, including mental health crisis-related home visits; psychiatric and non-psychiatric emergency service contacts; use of mental health rehabilitation services; and consultations with GPs. The selected predictor variables spanned four different domains: socio-demographic data, premorbid factors, characteristics of the disorder, and comorbidities and symptomatology.
Socio-demographic data included sex and age (age strata 18–34 years and 35–64 years); secondary school qualification (year 12) completion or above; marital status (married/de facto or single/separated/divorced); having any dependent children under 18 years of age living with the participant; being in any paid employment in the past 12 months; having someone to rely on; having someone to confide in; living alone; and social networks (number of friends).
Premorbid factors included poor premorbid work adjustment, poor premorbid social adjustment and premorbid personality disorder.
Characteristics of the disorder included age of illness onset and mode of onset (five categories); illness duration; and course of disorder (single or multiple episodes with partial or good recovery versus continuous chronic illness with or without deterioration).
Diagnosis, comorbidities and symptoms included: ICD-10 diagnosis of psychotic disorder; lifetime diagnosis of alcohol, cannabis and other substance abuse/dependence; past 12-month hallucinations, delusions, mania, anxiety/phobia, depressive symptoms, self-harm behaviours, suicidal ideation and subjective thought disorder. Negative or deficit symptoms were measured using a scale that summed scores on six items: diminished emotional range, diminished sense of purpose, loss of motivation, restricted affect, poverty of speech and impairment in socialising. Overall social functioning was assessed using the Personal and Social Performance (PSP) measure (Morosini et al., 2000). Finally, a measure assessing whether participants spoke a language other than English at home was included.
Data analyses
Statistical analyses were conducted using SPSS Version 20. Mantel–Haenszel chi-squared tests of significance were used to test the bivariate association between sex and each of the service utilisation components. Multivariate logistic regressions were performed to identify significant predictors of the likelihood of service use during the past year. Odds ratios (OR) and their estimated (95%) confidence intervals were reported to evaluate the magnitude of the effects. Given the large number of correlates/determinants in each set of regressions, Bonferroni adjusted probabilities were used to control the effect of each predictor for the number of outcome variables.
Results
Overview
There were 1087 males (59.6%), 57.6% of all participants were in the 35–64-year-old age group, 90.8% spoke English at home, and 24.5% of women and 12.1% of men were in a married or de facto relationship. (For a more detailed description of the sample see Morgan et al., 2012.)
Table 1 describes characteristics of the modal group in the central column, those recruited through public specialised mental health services (PSMHS) in the census month, compared to participants recruited through non-government organisations (NGOs) on the one hand, and those who were in contact with PSMHS only in the 11 months prior to census on the other (all are mutually exclusive categories). Those who were recruited through NGOs were more likely to be older (69.3%), engaged in formal studies (27.8%) and least likely to have dependent children at home (8.8%). Compared to those recruited through PSMHS in the census month, NGO participants were more likely to be in supported accommodation (18.5%) or report homelessness during the last 12 months (18%), and were less likely to have a diagnosis of schizophrenia or schizoaffective disorder (46.3%). NGO participants also reported lower use of mental health inpatient services, voluntary (19.5%) and involuntary (7.8%). They had very high participation in rehabilitation programs (74.1%).
Key characteristics.
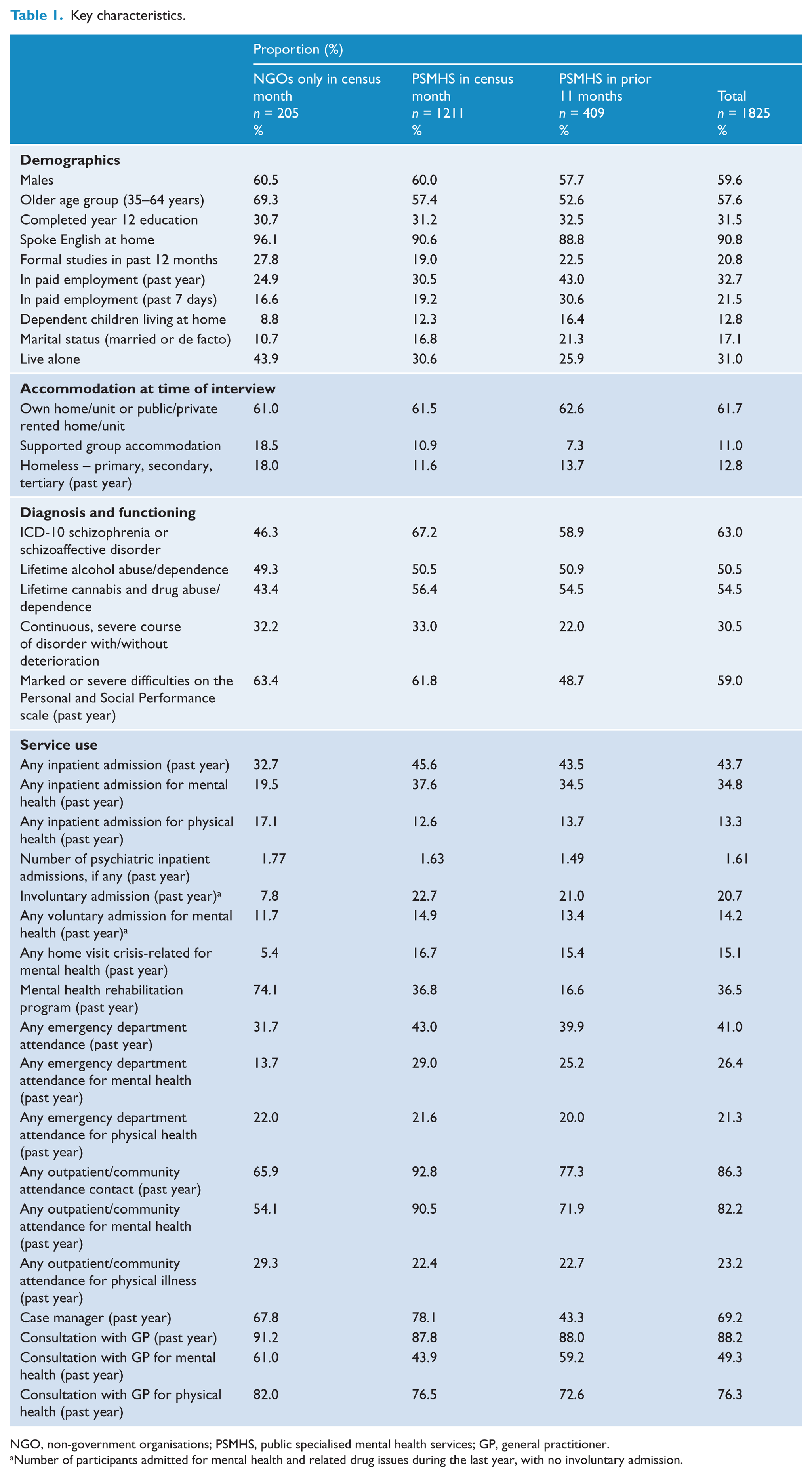
NGO, non-government organisations; PSMHS, public specialised mental health services; GP, general practitioner.
Number of participants admitted for mental health and related drug issues during the last year, with no involuntary admission.
Participants in PSMHS contact during the census month were more likely to have schizophrenia or schizoaffective disorder (67.2%), and to report high use of outpatient and community mental health services (92.8%). However, their use of GPs for mental health, at 43.9%, was lower than that of the other two groups. Those in contact with PSMHS in the 11 months prior to the census month exhibited higher rates of employment (43.0%), especially compared to those who were recruited through NGOs (24.9%); they were also more likely to be married or in a de facto relationship (21.3%) and to report having dependent children at home (16.4%) compared to their counterparts. They also showed less use of supported accommodation (7.3%) and were less likely to report a chronic continuous course of disorder (22%). Overall, these participants showed evidence of a higher level of functioning and reported less case management.
A series of multivariate logistic regression analyses was conducted to identify predictors of 12-month use of mental health and physical health services.
Table 2 shows the set of eight logistic regression models performed to predict use of the various types of mental health services. In each logistic regression the binary outcome was non-use (designated 0) versus use (designated 1) during the previous 12 months.
Significant determinants of mental health services utilisation (total sample 1825).
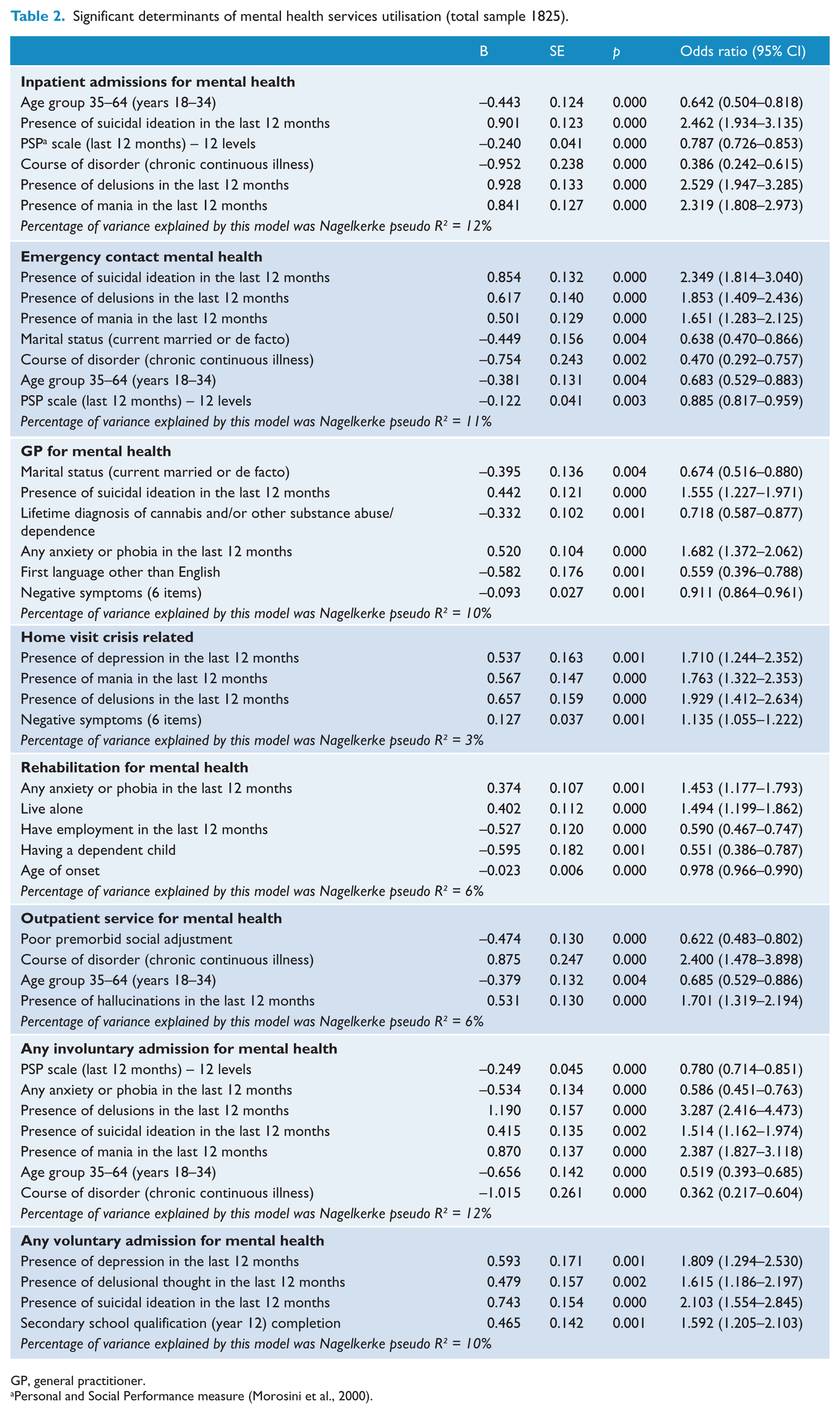
GP, general practitioner.
Personal and Social Performance measure (Morosini et al., 2000).
Determinants of mental health service utilisation
The likelihood of any psychiatric admission was associated with: younger age (18–34 years); symptoms of mania, delusions and suicidal ideation; a less chronic and disabling course of illness; and poorer social functioning. Among these predictors, the presence of delusions had the strongest association with inpatient admission, followed by suicidal ideation. For the other predictors, ORs ranged from 0.39 (non-chronic continuous course) to 2.32 (mania). Emergency contacts for mental health followed a similar pattern, being associated with: younger age; poorer functioning; less chronic and disabling course of illness; and symptoms of suicidal ideation, delusions and mania. Suicidal ideation was the strongest predictor of emergency service use.
GP contacts were associated with absence of substance abuse, fewer negative symptoms, being single, and not having English as the language spoken at home. GP contacts were also associated with suicidal ideation and anxiety/phobic symptoms. Crisis home visits were significantly associated with delusions, mania, depression and more negative symptoms. Use of rehabilitation services was associated with quite a different profile comprising unemployment, anxiety/phobic symptoms, having no dependent children, living alone and early age of onset. Living alone had the strongest association with use of rehabilitation services, followed by symptoms of anxiety/phobia. Outpatient/community clinic service use was associated with a chronic continuous course of illness, hallucinations and younger age. Participants who reported any use of outpatient/community services were also less likely to have a poor premorbid social adjustment. Finally, involuntary admissions presented the same pattern as for any psychiatric admissions (acute symptomatology, less chronic and disabling course of illness and poorer social functioning), while voluntary admissions were mainly related to the presence of symptoms of depression, delusions and suicidal ideation, with the latter again being the strongest predictor.
The variance explained by the models represented in Table 2 using the Nagelkerke pseudo R2 ranged from 3% to 12%. Pseudo R2 values suggest that our models are explaining a small proportion of the variation in health service use.
Determinants of physical health service utilisation
Table 3 shows the results of four sets of logistic regressions reporting the significant correlates of physical health service use. The likelihood of admission for physical health reasons was associated with older age, suicidal ideation and anxiety/phobic symptoms. Use of emergency services showed a similar pattern of correlates (anxiety/phobia and suicidal ideation), but with the addition of younger age of onset and a higher likelihood of having someone to rely on (mainly family members). GP contact for physical health reasons was mainly related to male sex, older age and better overall social functioning, but also to symptoms of anxiety/phobia. Reduced odds of using GP services were associated with having no lifetime history of substance abuse. Finally, the most important correlate of outpatient/community clinic use for physical health problems was anxiety/phobic symptoms. Participants who had used outpatient/community clinics were also more likely to be older and to be female.
Significant determinants of physical health services utilisation (total sample 1825).
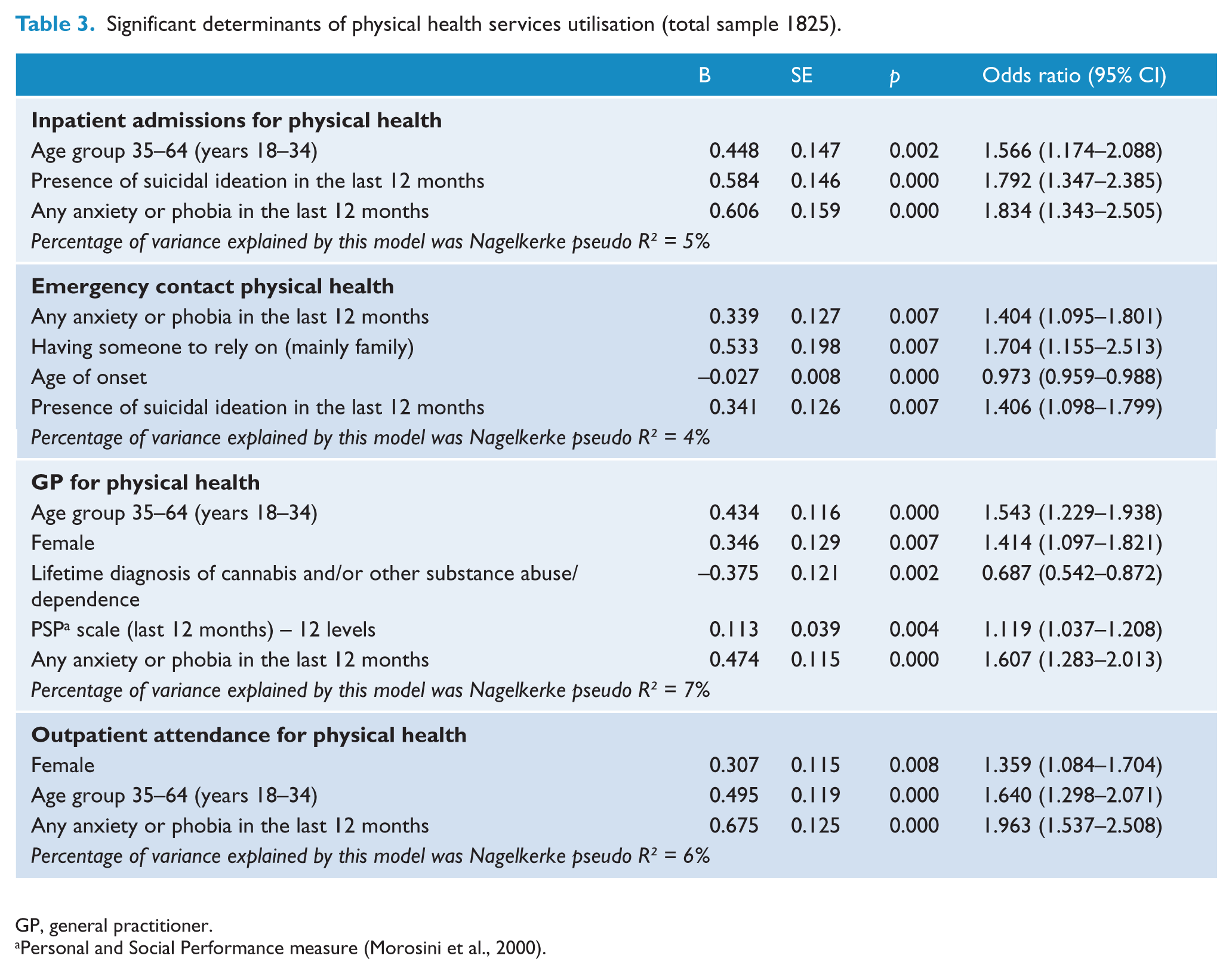
GP, general practitioner.
Personal and Social Performance measure (Morosini et al., 2000).
The variance explained by the models represented in Table 3 using the Nagelkerke pseudo R2 ranged from 4% to 7%.
Discussion
This study of service utilisation using data from the 2010 Australian national survey of psychosis shows some patterns of interest. Although the proportion of variance explained by the variables measured in the survey is small, some important predictors of service use were extracted and potential user profiles might be delineated as follows. (1) Frequent service users are younger and tend not to be in a sustained intimate relationship. Increased likelihood of service use occurs in those with few family contacts, little social support and high psychosocial needs for care. Loneliness and social isolation have been reported as the leading challenges faced by people with psychotic disorders (Morgan et al., 2011), and this is evidently contributing to greater service utilisation. (2) Comorbid anxiety/phobic symptoms predict the use of several types of services, particularly physical health and non-acute mental health services, and such symptoms were reported by almost 60% of the sample (Morgan et al., 2011). This strongly suggests a need for anxiety and stress management services that may not yet be widely available. It is interesting that comorbid substance abuse was not a strong predictor of service use, in spite of an increase in the prevalence of these problems in the context of psychosis (Morgan et al., 2012). The very high rates of comorbid drug and alcohol abuse in this population may have contributed to a ceiling effect and failure to appear as a significant service use predictor. (3) One of the most important contributors to the likelihood of mental health service use was symptom severity; in particular, high levels of mania, hallucinations, delusions and suicidal thoughts were strongly related to service use. These are all needs-related factors (after Anderson), suggesting that services are functioning in accordance with expectations and are meeting critical needs.
Pattern of service use by source of recruitment
Compared to those recruited from PSMHS during the census month, participants recruited through the NGOs were higher users of mental health rehabilitation programs and lower users of mental health inpatient, community or emergency/crisis services. This pattern suggests in the NGO clientele a relatively stable clinical picture, comparatively late in the course of the illness, with less engagement in PSMHS, but requiring accommodation assistance and support. It suggests that NGO services are acting in a way that is complementary to PSMHS, targeting a population needing maintenance care rather than the acute care that is generally provided by PSMHS.
Participants who were in recent contact (previous 11 months) with PSMHS were more likely to be younger, employed, married, higher functioning and showing an episodic course of illness compared to those who were in contact with PSMHS during the census month. With regard to their service utilisation pattern, they showed a slightly lower rate of admissions for mental health problems, and if they were admitted their length of stay was shorter. This group presented very low rates of rehabilitation program utilisation, low rates of case management and low rates of outpatient/community attendances for mental health. This appears to be a better functioning group with a more benign pattern of illness, and one that probably requires, and certainly consumes, fewer mental health services.
Correlates of service use
Within the framework of Andersen’s behavioural model of access to health care, a number of variables were associated with the likelihood of service use. Mental health inpatient admissions, emergency service use and crisis home visits – all acute services – were overwhelmingly driven by needs-related factors, whereas GP, rehabilitation and community/outpatient services were driven by a mixture of predisposing, enabling and needs-related factors.
Higher levels of illness severity (needs-related factors, following Andersen’s model) were associated with a greater likelihood of use of acute services. Recurring correlates with the use of these services included suicidal ideation, mania and delusions. These symptoms were evident in relation to inpatient service use (involuntary and voluntary), home crisis visits and emergency department attendance. The greater likelihood of hospitalisation was associated with younger age and an episodic (less chronic continuous) course of illness. Clearly these services are being accessed appropriately by patients in crisis, who are at risk of harm, and who have severe psychotic or mood symptoms and require immediate care and protection, which is the typical purpose of acute services.
In contrast, use of non-acute services (i.e. outpatient/community services, GP consultations and rehabilitation services) was associated with different factors. For instance, GPs were more likely to be used by people who were divorced, who suffered anxiety/phobic symptoms, who did not have substance abuse problems and were English speakers. Outpatient/community services were more frequently used by younger people with good premorbid adjustment, hallucinations and a less chronic disabling course of illness. Rehabilitation service users were more likely to live alone, less likely to have had children, were unemployed and had an earlier age of illness onset. Acute service use for physical health problems (i.e. inpatient admission and emergency services) was associated with suicidal ideation and anxiety/phobic symptoms. An unknown proportion of these would likely have been related to suicide attempts or self-harming behaviours. Use of GPs and outpatient services for physical health reasons were both associated with being female, older age and the presence of anxiety/phobia. In addition, GP attendees were less likely to have had a lifetime history of substance abuse and showed a higher level of functioning. Finally, specific correlates of physical health service use included older age, female sex and presence of anxiety/phobic symptoms. The recurring association of anxiety/phobic symptoms with physical health service use implies a degree of worry and apprehension either secondary to physical ill health or contributing to health-care seeking.
Service utilisation patterns have changed in over a decade since the first national survey of psychosis (Jablensky et al., 1999). Service utilisation in 2010 (n = 1211 using PSMHS in the census month) has been compared with data from the first survey in 1997–1998 (n = 687 using PSMHS in the census month) (Morgan et al., 2011, 2012). Both studies used a similar design, comparable instruments and identical sampling methodology in relation to patients in contact with PSMHS during the census month. There has been a reduction in hospital admissions from 58.7% to 37.6% and a reduction in both voluntary and involuntary admissions. Emergency Department attendances declined slightly (47.6% to 43.0%). In contrast, outpatient and community service use increased substantially between 1997/98 and 2010, with 92.8% of people in contact with outpatient and community clinics in 2010 compared to 75.3% previously. The percentage of persons using community rehabilitation or day programs rose from 22.9% to 36.8% over the 12 years, and the role of NGOs in the provision of mental health care showed an increase from 18.9% to 26.5%. Use of GPs increased from 76.7% to 87.8%. Overall, the pattern since 1997/98 has been a reduction in hospital inpatient care and a shift towards more community-based care involving PSMHS, NGO and private (GP) sectors.
Patterns of mental health service use in the first psychosis survey have been published (Carr et al., 2003). Strikingly in line with results reported here, significant predictors of inpatient service use for mental health in 1997/98 were acute symptoms; namely, mania, delusions and suicidal thoughts. However, while in the first survey the use of inpatient services was associated with good social functioning, in the second survey inpatient admissions for psychiatric reasons were associated with poor social functioning. This may reflect a shift in hospital use towards admissions of more severely and acutely ill patients as more effective use of outpatient/community and rehabilitation services over the past 12 years has increased, obviating the need for hospital admissions in many cases, and the practice of hospital beds being used as surrogate accommodation facilities has declined.
Similarities between the two surveys have been found for emergency mental health service use, with predictors of such use in both studies including suicidal thoughts, younger age and being married or in a de facto relationship. Other comparisons between the two surveys show more differences than similarities in the predictors of service utilisation. Much has changed on the service delivery landscape as documented in the second national survey, and this is bound to change the patterns of service use correlates, with the evident exception of acute mental health services.
The small proportion of variance accounted for by the variables examined in this study is virtually identical to the findings reported for the first psychosis survey (Carr et al., 2003), in which range restriction (e.g. narrow diagnostic spectrum, sampling predominantly from public mental health services with relative under-representation of those treated solely in the private sector by psychiatrists and/or GPs) was proposed as a partial explanation for this effect, an interpretation that would also apply in the present survey. However, it is also likely that many other factors influence service use apart from individual patient characteristics, such as availability and accessibility of services, differential resource allocation and local variations in health policies and practices. Variables that might have been expected to be associated with service use, such as drug and alcohol abuse or dependence, failed to retain the statistical significance achieved in univariate analyses when entered into multivariate logistic regressions with Bonferroni correction.
This paper is part of a suite of publications arising from the second Australian national psychosis survey, and policy and service planning implications need to be derived from the totality of the published material, including the analysis of costs and cost changes (Neil et al., 2014a, 2014b).
Conclusions
Service utilisation patterns vary with patient clinical and socio-demographic features, inpatient and emergency service users being similar in such features with a preponderance of needs-related factors predicting their use. In this they differ from users of other services where there is a mixture of predisposing, enabling and needs-related factors. There were somewhat similar findings in relation to physical health services.
Factors associated with an increased likelihood of mental health service use within the second national survey of psychosis (suicidal ideation, mania, delusions, younger age, social isolation) are broadly consistent with the results of previous research (Carr et al., 2002, 2003; Fleury et al., 2010; Putkonen et al., 2011; Uebelacker et al., 2006; Vasiliadis et al., 2007). Comparison with the first survey suggests a shift in service use with a significant decline in acute inpatient admissions and a substantial increase in outpatient/community and rehabilitation service use over the past 10 years.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis (SHIP). The members of the SHIP Study Group are: V. Morgan (National Project Director), A. Jablensky (Chief Scientific Advisor), A. Waterreus (National Project Coordinator), R. Bush, V. Carr, D. Castle, M. Cohen, C. Galletly, C. Harvey, B. Hocking, A. Mackinnon, P. McGorry, J. McGrath, A. Neil, S. Saw, H. Stain. Ethics approvals for the study were obtained from relevant institutional human research ethics committees. The main study was funded by the Australian Government Department of Health and Ageing. This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Funding
This paper did not receive any specific funding. The original SHIP study was funded by the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.