
Abstract
Objective:
The relationship between psychosis and contact with the criminal justice system for Indigenous people living in rural and remote areas is not well understood. In this study, the authors examine patterns of incarceration among Indigenous people living with psychosis in Cape York and the Torres Strait over two decades.
Methods:
Data were collated from a clinical database of complete psychiatric records from 1992 to 2015, extracted for all Indigenous patients with a psychotic disorder from the Remote Area Mental Health Service, and linked to the Queensland Corrections Service database. Descriptive statistics were calculated to compare characteristics between those incarcerated and those not incarcerated during the study period and to quantify patterns of incarceration including types of offences, time spent in custody and frequency of incarceration. Multivariate Cox regression analysis was used to assess associations between reported variables and ‘first incarceration’.
Results:
Forty-five percent of Aboriginal patients (n = 116) were incarcerated compared with 31% of Torres Strait Islanders (n = 41) (p = 0.008), and the proportion of males incarcerated (51%, n = 141) was approximately twice that of females (24%, n = 35; p = 0.001). A cluster of first incarcerations were observed in close time proximity to diagnosis of psychosis. Individuals who had a history of both alcohol and cannabis use had approximately two times higher risk of being incarcerated following positive diagnosis compared to those without a history of substance use (hazard ratio = 1.85; 95% confidence interval: [1.08, 3.17]; p = 0.028). Males accounted for approximately 85% (n = 328) of sentences. The most common most serious offence was causing physical harm to others (assault – n = 122, 31%).
Conclusion:
Our study found that for Aboriginal and Torres Strait Islander people with a psychotic disorder in North Queensland, criminal justice responses with resultant incarceration occurs frequently. Access to appropriate mental health services and diversion options for Indigenous Australians with psychosis should be a key public health and justice priority.
Introduction
One of the landmark findings of Australia’s 1989 Royal Commission into Aboriginal Deaths in Custody was that Indigenous people were vastly over-represented in Australia’s prisons (Royal Commission into Aboriginal Deaths in Custody, 1991). Despite key recommendations to government to reduce this over-representation, 30 years on, Indigenous Australians, who make up less than 3% of the Australian population (Australian Bureau of Statistics, 2016) but comprise 28% of the prison population, are incarcerated at an age standardised rate of 2088 per 100,000 population compared to non-Indigenous Australians who are incarcerated at a rate of 173 per 100,000 population (Australian Bureau of Statistics, 2019). Reducing this over-representation, recognised to be significantly related to health gaps, particularly mental health, is a justice and health policy priority for Australia (Australian Human Rights Commission, 2015; Australian Medical Association, 2015; National Mental Health Commission, 2013).
It has been well established in Australia (Butler et al., 2006) and internationally (Sirdifield et al., 2009) that psychiatric morbidity is far greater among people in prison compared to the community. Research in three jurisdictions in Australia has indicated that the prevalence of mental disorder among Aboriginal and Torres Strait Islander people in prison is concerningly high (Butler et al., 2007; Heffernan et al., 2012b; Ogloff et al., 2013) particularly with regard to psychotic disorder. For example, Heffernan et al. (2012a) estimated the 12-month prevalence of psychotic disorder in Indigenous people in Queensland prisons to be 8% for males and 25% for females (Heffernan et al., 2012b). Studies in other Australian jurisdictions using screening instruments for psychosis have generated similar prevalence estimates (Butler et al., 2007; Tye and Mullen, 2006).
The treated prevalence of psychotic disorders in remote communities of Cape York and the Torres Strait over a 3-month period has been previously estimated at 1.68% (Hunter et al., 2012) – several times higher than in the general population of Australia. That same study reported alarming results regarding lifetime rates of incarceration in this sample – 43.9% of Aboriginal and 10.3% of Torres Strait Islander, patients with a history of psychosis and 42.5% men and 4.4% women. However, a limitation of this study was that it was based on self-report.
In a recent study, Gynther et al. (2019) reported on data collated from a clinical database of the Remote Area Mental Health Service (RAMHS) that contains complete psychiatric records of all Indigenous patients from remote communities of Cape York and the Torres Strait who were treated for psychotic disorders over a 23-year period, 1992 to 2015. The treated prevalence of psychotic disorders was shown to increase throughout the study period to 2.3% and 1.1% in 2015 for males and females, respectively. The highest treated prevalence in 2015 was in Aboriginal men (4.0%).
In this study, the authors linked RAMHS data with Queensland Corrective Services (QCS) records with the aim of examining patterns of incarceration among Indigenous people living with psychosis in Cape York and the Torres Strait over two decades. Specifically, we aimed to examine the prevalence, frequency and duration of incarceration over time; what types of offences resulted in incarceration; the temporal relationship between psychosis diagnosis and incarceration; and the association of other patient characteristics with incarceration.
Methods
Study location and sample
Commenced in 1992, psychiatric services for the residents of Cape York and the Torres Strait region of northern Queensland were delivered by the RAMHS. Clinical data on all patients who received treatment between 1992 and 2015 were entered by the clinical team into a purpose-built electronic database (initially Filemaker Pro subsequently imported into Microsoft Access). From the RAMHS database, we identified all Indigenous patients diagnosed with a psychotic disorder – including schizophrenia, schizoaffective disorder, delusional disorder, schizophreniform disorder, acute or transient psychotic disorder, drug- or alcohol- induced psychosis, depressive episode with psychotic symptoms, bipolar disorder with psychotic symptoms, and organic psychotic disorder. Clinical diagnoses were made by RAHMS psychiatrists (including authors E.H., B.G. and K.O.) and were informed by International Classification of Diseases, Ninth Revision (ICD-9) and International Classification of Diseases, 10th Revision (ICD-10), and by Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev; DSM-III-R, 1987), Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV, 1994) and Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5, 2013), as appropriate depending on the year of diagnosis. From these patient records, we extracted demographic and patient history information including ethnicity, sex, age of psychosis diagnosis and harmful substance use. This study examines RAHMS patient data over a 20-year period, 1995 to 2015.
We define incarceration throughout this paper as imprisonment and exclude incarceration in a watch house. Identifying information from the RAMHS database was used to probabilistically link the Queensland Corrections Service (QCS) database to identify RAMHS patient interactions with the justice system, including admission and release dates for all periods of incarceration between 1985 and 2015. Offence data was recorded as the most serious offence associated with incarceration. The most serious offence was determined using Australian and New Zealand Society of Criminology (ANZSOC) categories (Australian Bureau of Statistics, 2011). We collapsed these categories into nine categories: homicide, assault (robbery/assault), sexual, dangerous acts (abduction/drink driving/go armed), property (stealing/break and enter/fraud), justice, nuisance (public nuisance/weapon possession/driving/property damage) and drug offences. We dichotomised ANZSOC 1-6 as violence offences, the rest as non-violent.
Statistical analysis
All statistical analyses were undertaken in Stata 15 (StataCorp, 2015). Analyses were limited to patients who entered custody from the age of 17, whom during the study period were considered adults by QCS.
Descriptive statistics were calculated to compare characteristics between those incarcerated and those not incarcerated during the study period and to quantify patterns of incarceration including types of offences, time spent in custody and frequency of incarceration. Categorical variables are presented as counts and percentages, estimates of central tendency and variation are described by median and interquartile range (IQR), respectively, due to the skewed distribution of data. Comparisons of medians (e.g. age of diagnosis) were calculated using the nonparametric K-sample equality of means test.
Multivariate Cox regression analysis was used to assess associations between reported variables and a dependant variable ‘first incarceration’ as identified by QCS records. All variables that were likely to have an association, based on existing literature and clinical expertise, with incarceration were identified by a preliminary univariable Cox regression. We included predictor variables with univariate relationship of p < 0.20 in the multivariate Cox regression analysis. Specific interactions between variables were not specified prior to multivariate modelling; instead, all possible interactions were tested one at a time for significance and excluded if the interaction term was non-significant – the ‘elimination scheme’ (UCLA: Institute for Digital Research and Education, n.d.). To assure that the Cox models were specified correctly, the assumption of proportional hazards was tested for each multivariate model and compared using the Akaike information criterion (AIC). Adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) for each predictor variable were calculated from the parameter estimates and standard errors. Tests of significance were two-tailed, with the alpha level set at 0.05.
Probability of non-incarceration was assessed graphically using Kaplan–Meier survival curves assessing the time interval between diagnosis and first incarceration and stratified by ethnicity, sex and time of diagnosis.
Ethical considerations
Ethical approval for this study was obtained from Far North Queensland Human Research Ethics Committee and the University of Queensland (reference HREC/16/QCH/5 – 1024) and the University of Queensland (approval 2016000921). Approval for the research was also obtained in accordance with the Queensland Public Health Act 2005 (approval RD006276).
As this is a retrospective study, it was not possible to obtain consent from patients and a waiver of consent was obtained during the Ethics approval process. The information recorded in the RAMHS database was gathered in the course of normal clinical service delivery. The results are published with no disclosure of community of origin other than being located in Cape York and the Torres Strait.
Results
Of the 426 individuals identified through patient record extraction, 4 (0.9%) were under the age of 17 at the time of first incarceration and were excluded from analyses. Of the remaining 422, 42% were incarcerated at some point in their lifetime (n = 176). Forty-five percent of Aboriginal patients (n = 116) were incarcerated compared with 31% of Torres Strait Islanders (n = 41) (p < 0.01), and the proportion of males incarcerated (51%, n = 141) was approximately twice that of females (24%, n = 35; p < 0.01). Aboriginal males accounted for 55% of those who had been incarcerated. The median age of those incarcerated in 2015 was 28 (IQR: 25–40). Patient characteristics can be found in Table 1.
Demographic characteristics (N = 422).
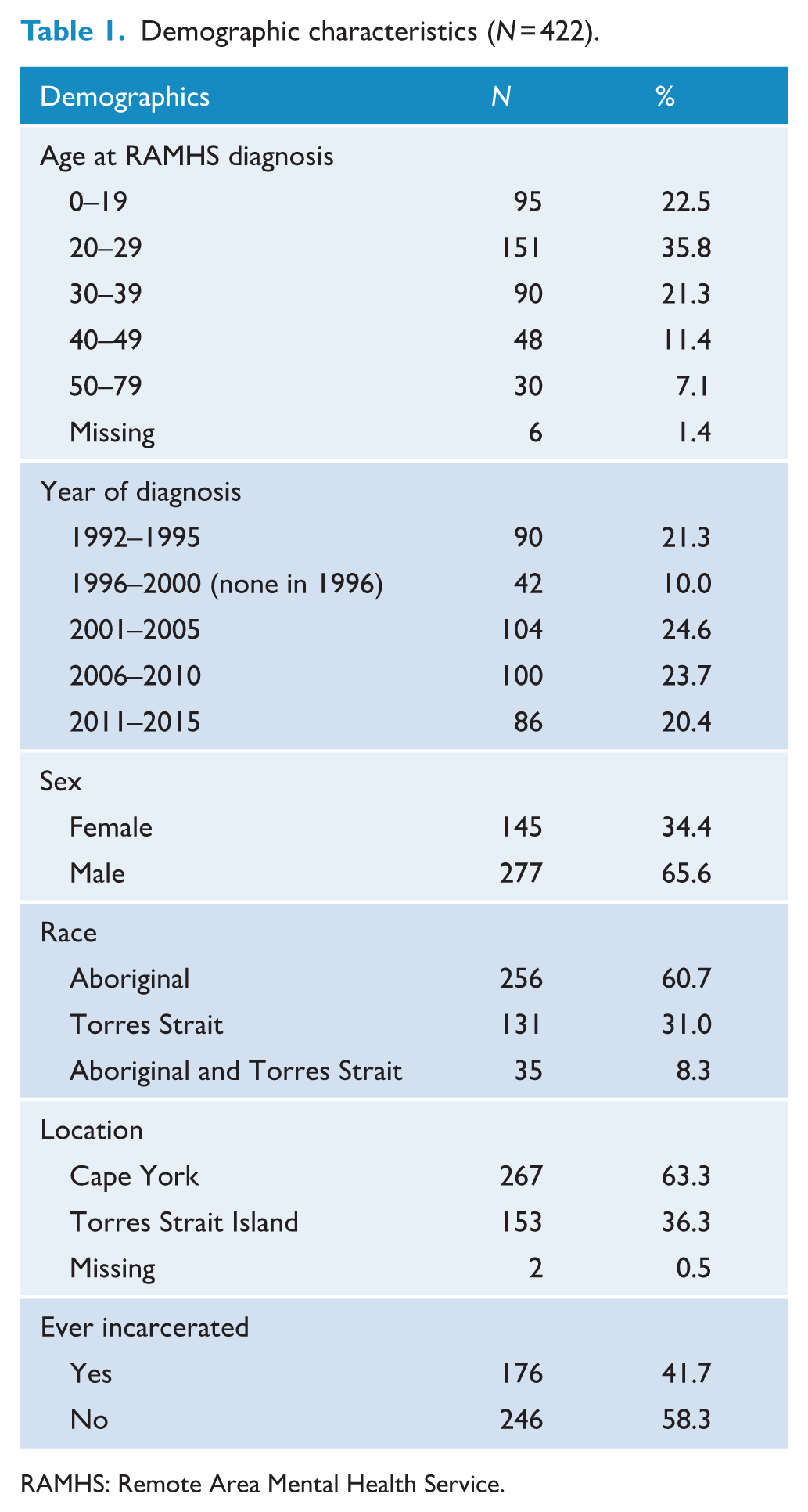
RAMHS: Remote Area Mental Health Service.
Age of diagnosis of psychosis and first incarceration
The median age of first incarceration was 21 years (IQR: 18–27); 25 (IQR: 20–29) for females and 20 (IQR: 18–25) for males. The largest number of first incarcerations occurred between ages 17 and 20 (N = 84), including more than half of male first incarcerations (N = 75). Both male and female incarcerations tapered over the lifespan; however, this trend was most marked in males. Few first incarcerations occurred after age 40 (N = 5) (Figure 1).
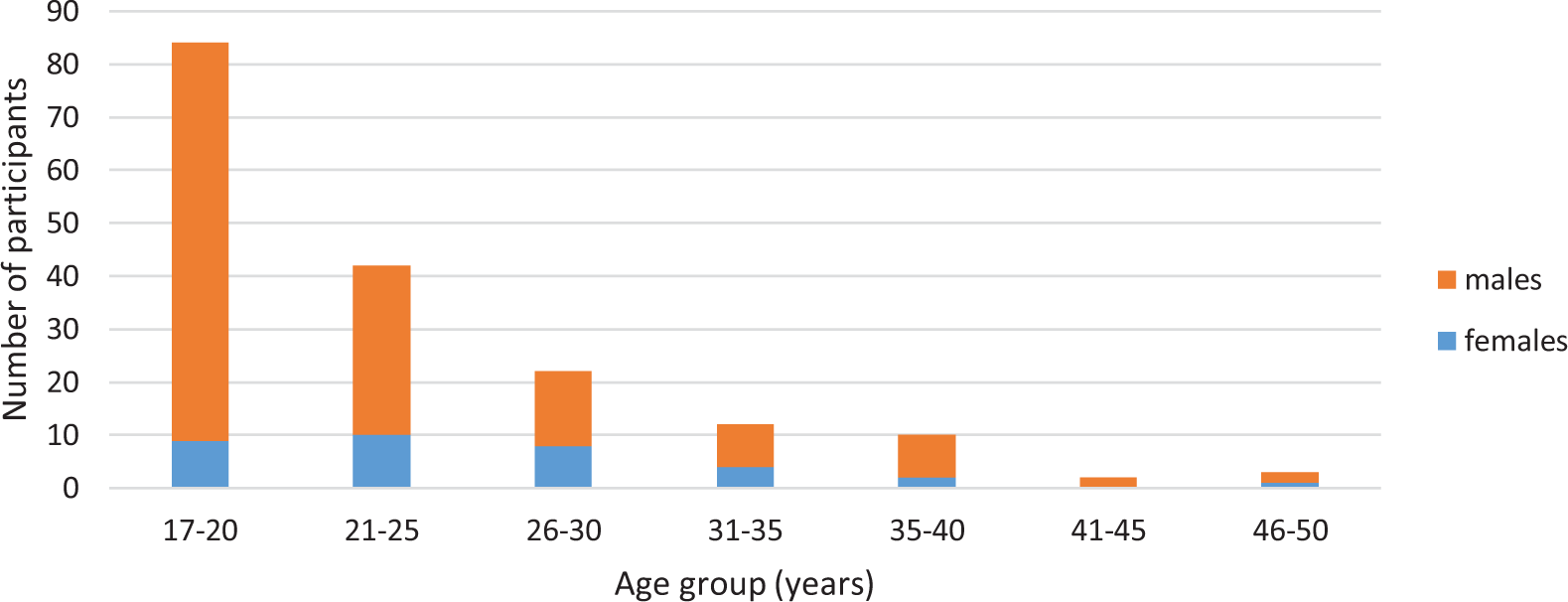
Age of first incarceration, by sex.
Changes in incarceration rates over time
Incarceration rates among Aboriginal and Torres Strait Islander people living with psychosis varied between 14% and 35% and averaged 25% across the study period (Figure 2). A reduction in incarceration is observed in the mid-2000s. The proportion of incarcerated female Indigenous patients increased between 1995 and 2015, particularly in the female Aboriginal population (Supplemental Figure S1); however, this increase was not statistically significant. Incident rates of incarceration among the cohort were consistently higher in males than females throughout the study period; however, the male-to-female ratio decreased over time with the ratio being its smallest (0.9) in 2015 (Supplemental Figure S2).
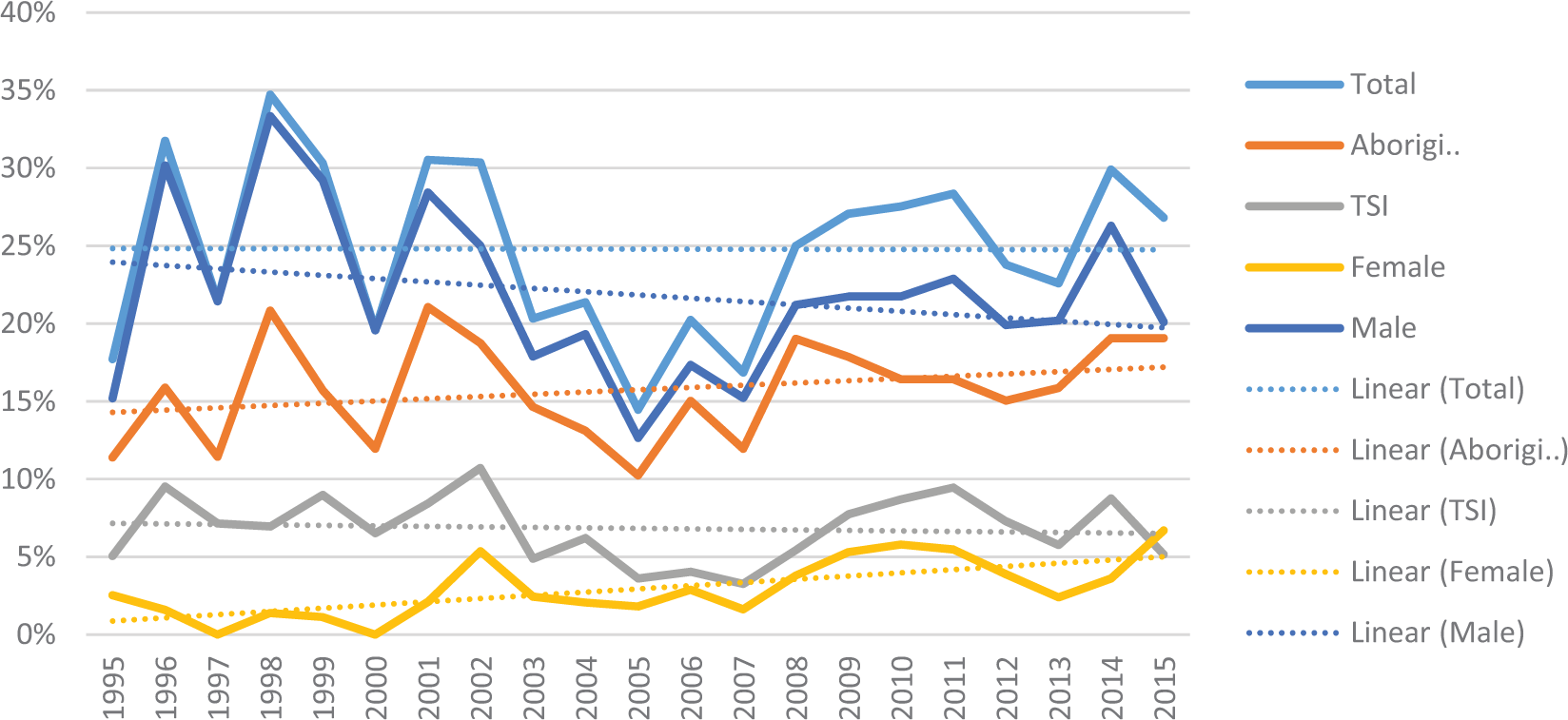
Proportion of participants with a current psychosis diagnosis experiencing a period of incarceration, by year, race and sex.
Within the Aboriginal population, male non-violent offences fell but then began rising again around the mid-2000s, while the proportion of Aboriginal male patients incarcerated for violent offences remained high (Figure 3).
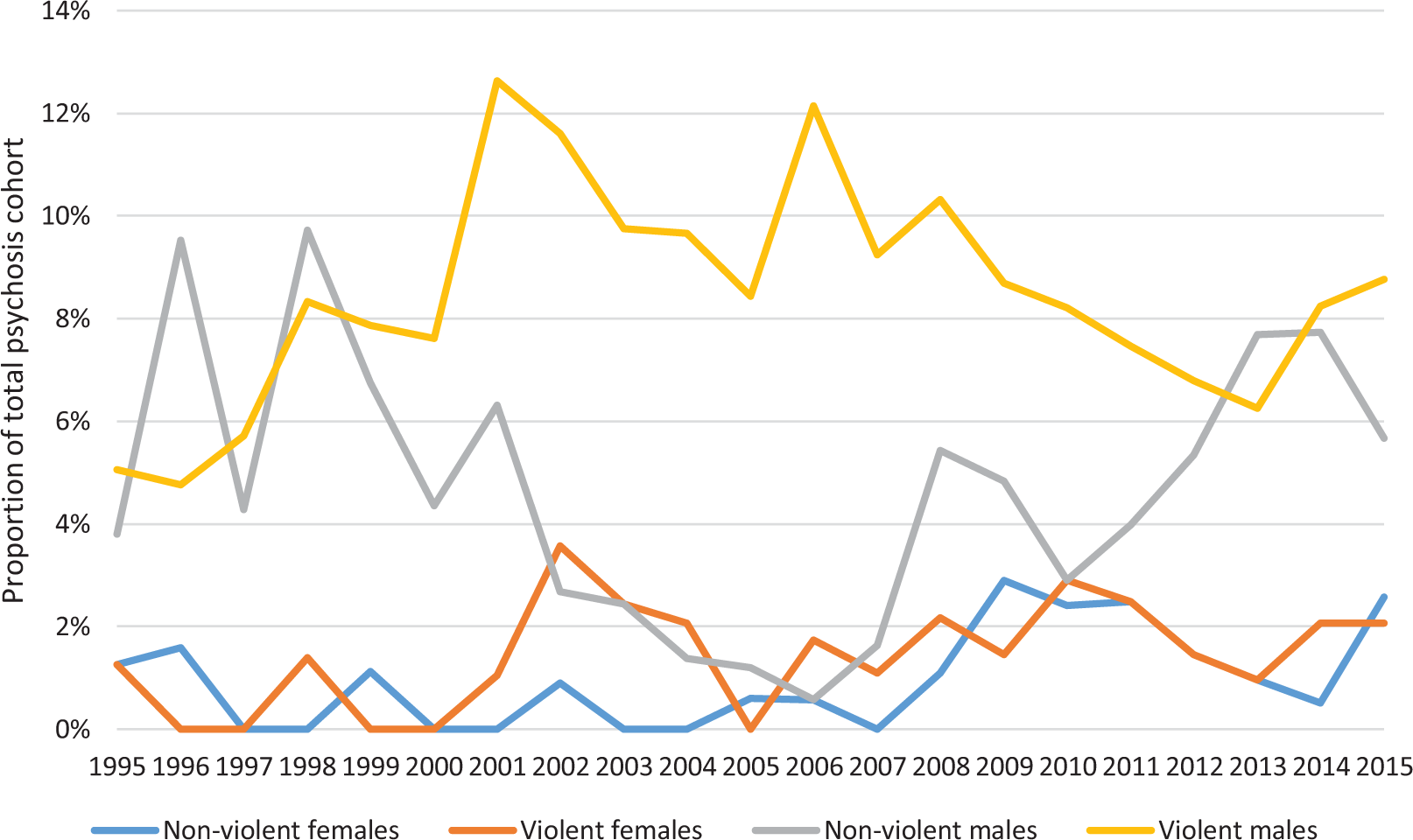
Proportion of Aboriginal participants with a current psychosis diagnosis experiencing a period of incarceration, by year, sex and offence type.
Survival curves examining the probability of being incarcerated as a function of time since diagnosis are presented in Supplemental Figures S3 and S4. After receiving a diagnosis of psychosis, there was greater probability of being incarcerated in Aboriginal patients (vs Torres Strait Islanders) and males (vs females). However, examination of whether diagnosis of psychosis was made pre- or post-2000 demonstrates a considerable reduction in the differences between these groups over time. No differences in rates of incarceration between Aboriginal and Torres Strait Islanders, and males and females, respectively, were observed post-2000.
Types of offences
Males accounted for approximately 85% (n = 328) of sentences – this proportion did not change when comparing violent and non-violent offences. The most common and most serious offence was causing physical harm to others (assault – n = 122, 31%); this was followed by nuisance (n = 75, 19%) and property charges (n = 65, 17%) (Figure 4). Non-violent offences (n = 219, 56%) outnumbered violent offences (n = 170, 44%) and this trend was observed across all subgroups – Aboriginal patients, Torres Strait Islanders, males and females.
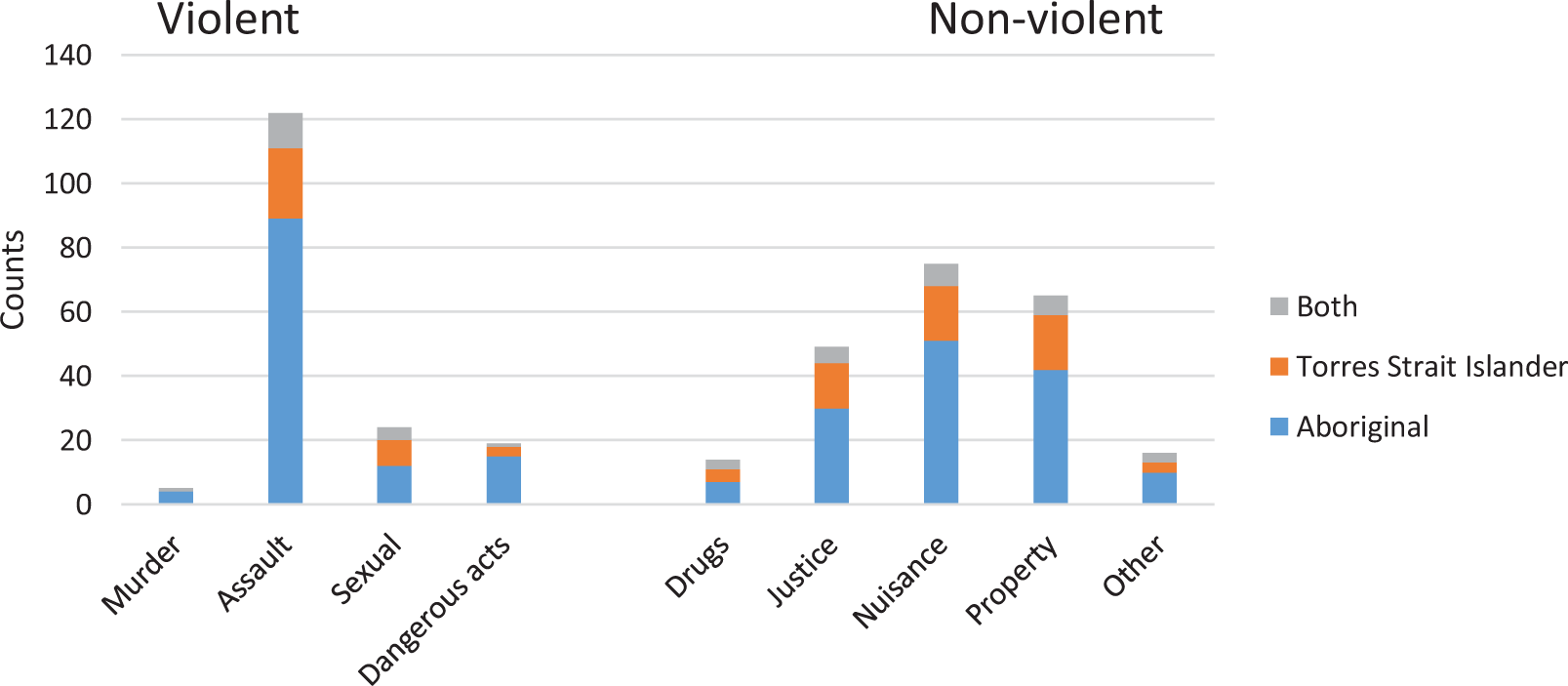
Frequencies of most serious offence type per incarceration, by race. Note: x-axis represents the frequency of most serious offence for each incarceration. Participants may have multiple ‘most serious offences’ across the study period.
Frequency and duration of incarceration
Of those in our sample who had ever been incarcerated, the median number of incarceration periods was 3 (IQR = 2–6). Of the 175 individuals who experienced at least one incarceration during the study period, 43 (25%) people experienced only one incarceration. The median cumulative time spent in custody was 3 years with a maximum of 18 years.
Overall, both the median number of times and cumulative time spent in custody for males were greater than those for females (p = 0.03 and p = 0.01, respectively). There were no differences between ethnicity. Statistically significant differences in median number of times in custody were observed between Aboriginal males and females (4 and 2 years, respectively, p = 0.04); however, there was no statistically significant difference observed between Torres Strait Islander males and females. Those incarcerated prior to diagnosis of psychosis had greater median cumulative time spent in custody than those who were incarcerated post-diagnosis (4 and 2 years, respectively; p < 0.01).
Time relationship between diagnosis and incarceration
Patients were being diagnosed with psychosis both before and after first entering custody; however, a cluster of first incarcerations are observed in close time proximity to diagnosis of psychosis (Figure 5). A total of nine patients were diagnosed with psychosis during the period of their first incarceration, and of the most serious offences for these incarceration episodes, five were classified as violent offences and four were non-violent.
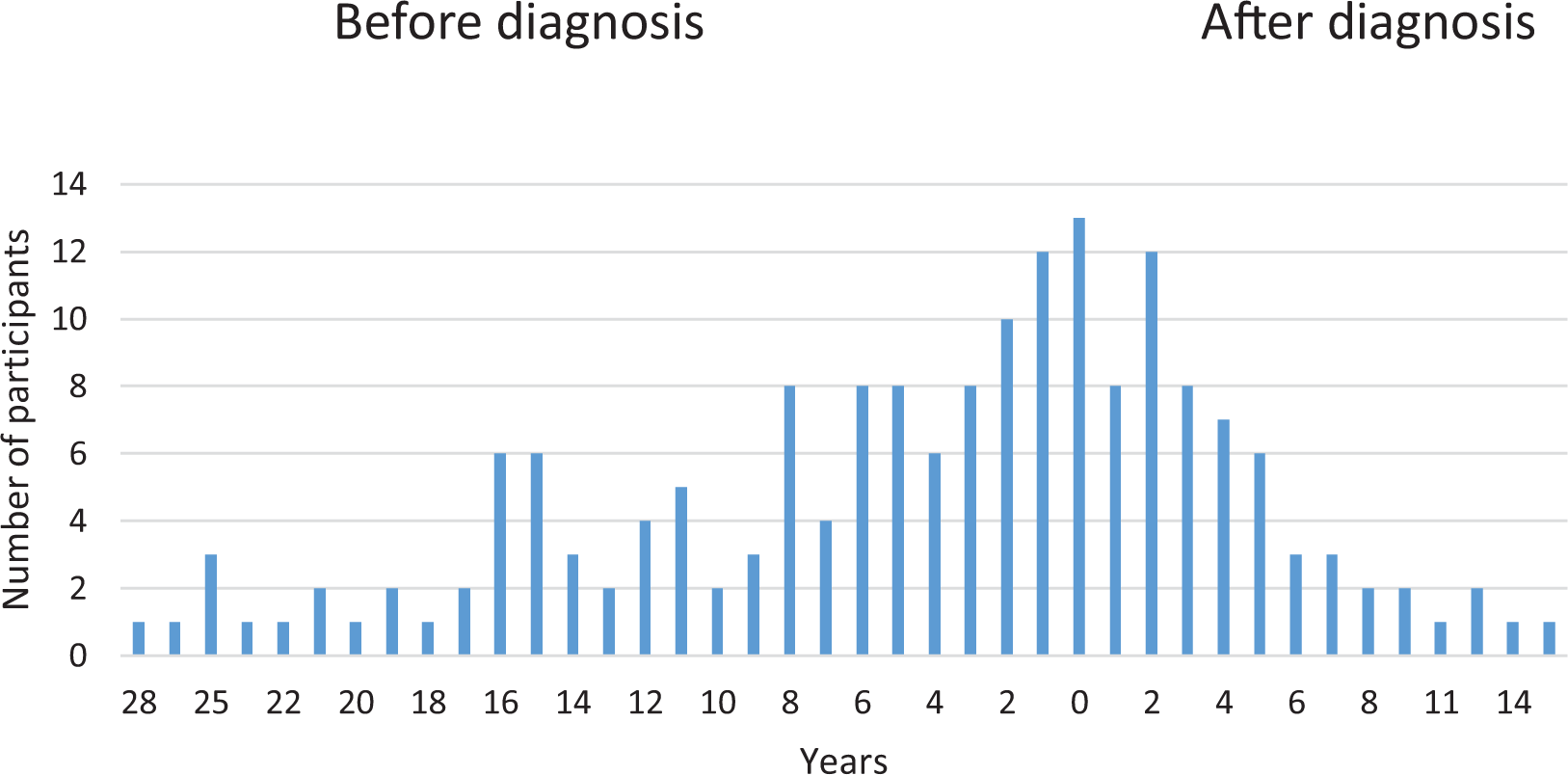
Time between first diagnosis and first incarceration.
Predictors of incarceration
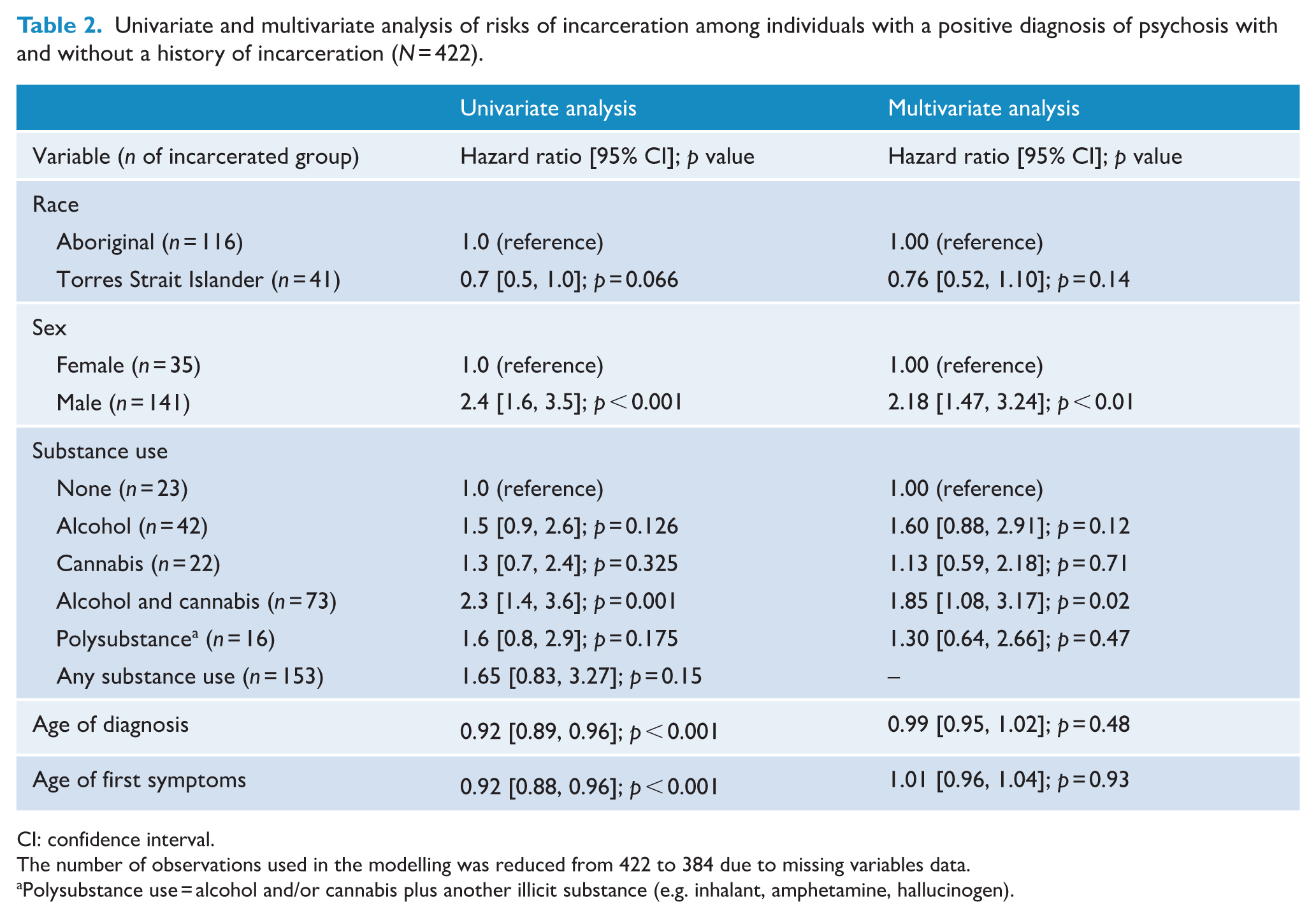
Ethnicity, sex, substance use, age of diagnosis and age of first symptoms were fit in our multivariable model (Table 2 and Supplemental Table S1). After adjusting for model covariates, individuals who had a history of both alcohol and cannabis use had approximately two times higher risk of being incarcerated following positive diagnosis compared to those without a history of substance use (HR = 1.85; 95% CI: [1.08, 3.17]; p = 0.028) (Table 2). Males diagnosed with psychosis at some point in their life were more than twice as likely to be incarcerated as females (HR = 2.18; 95% CI: [1.47, 3.24]; Table 2). However, these differences were moderated in the sample subsets who were incarcerated for the first time post-diagnosis (Supplemental Table S2).
Univariate and multivariate analysis of risks of incarceration among individuals with a positive diagnosis of psychosis with and without a history of incarceration (N = 422).
CI: confidence interval.
The number of observations used in the modelling was reduced from 422 to 384 due to missing variables data.
Polysubstance use = alcohol and/or cannabis plus another illicit substance (e.g. inhalant, amphetamine, hallucinogen).
Discussion
In this paper, we have described for the first time, the patterns of incarcerations in a cohort of Aboriginal and Torres Strait Islander people living with psychosis in North Queensland using data linkage. We found extremely high rates of incarceration among Indigenous people in North Queensland who received a diagnosis of psychosis, with 4 out of 10 incarcerated at some point during their lifetime. The rates of incarceration among this population remained relatively consistent over two decades. In comparison with the previous study by Hunter et al. (2012), self-reported incarceration rates for Aboriginal patients and males were found to be very similar (approximately half of Aboriginal patients and half of males). However, we found much higher incarceration rates for Torres Strait Islander patients with psychosis (31% compared to 10%) and female patients (24% compared to 4%). Our findings are of major concern and clearly indicate that repeated calls to reduce the overrepresentation of people with mental illness (World Health Organization Europe, 2007) and Indigenous Australians in prison (Australian Government, 2018) have failed.
In 2014, the incarceration rate for our sample was approximately 30,000 per 100,000 people. In the same year, the general Australian incarceration rate was approximately 200 prisoners per 100,000 and 2000 for Indigenous Australians (150- and 15-fold that of our study sample, respectively) (Australian Bureau of Statistics, 2018). Furthermore, while we are not able to ascertain imprisonment rates for the broader Indigenous population of our study location, it has been reported that the imprisonment rate for Indigenous people who live in remote areas is more than 40% higher than for those not living in remote areas (Queensland Productivity Commission, 2019). However, it remains apparent that the rates of incarceration are significantly higher in our study cohort than those not living with psychosis. While a direct comparison of these incarceration rates are limited by issues such as age standardisation and denominator, the magnitude of difference warrants urgent consideration with a view to policy reform. This finding raises questions about the pathways into the criminal justice system for Indigenous Australians as previously described for individuals in other jurisdictions (Baldry et al., 2015) and in other studies (Heffernan et al., 2012b). As social disadvantage is a common determinant of mental ill-health and criminal justice system involvement (Marmot, 2020), addressing Indigenous disadvantage in Northern Queensland would likely improve mental health and redress rates of Indigenous incarceration and should be a public policy priority.
Although absolute numbers are low, our findings show increasing rates of incarceration of Indigenous women over the period from 1995 to 2015. In 2018, the Queensland imprisonment rate for Indigenous males was 8.8 times that of Indigenous females (Queensland Government Statistician’s Office, 2018). However, our study found a male-to-female ratio of only 0.9 in 2015. Compared to women in the community, women in prison are 23 times more likely to have psychosis (Tye and Mullen, 2006). Prior research has also observed a higher prevalence of mental health disorders and mental health comorbidity among women compared to men in prison (Baranyi et al., 2018; Butler et al., 2011). An over-representation of Indigenous women with a psychotic disorder was reported by Heffernan et al. (2012b) which estimated the 12-month prevalence of psychotic disorder in Indigenous people in Queensland prisons to be 8% for males and 25% for females (Heffernan et al., 2012a). When taken together, this suggests that psychotic disorders are a key correlate of incarceration for Indigenous women and a critical target for public health intervention in remote communities in Australia.
In our previous paper (Gynther et al., 2019), we suggested that marked instability in remote Aboriginal communities of Cape York, from the mid-1980s to the early 2000s, had impacts on childhood development which may have contributed to a greater vulnerability to the later development of a psychotic disorder. With the relationship of childhood trauma to incarceration being particularly strong for women (Moore et al., 2013), it may be that the increasing number of women in our sample being incarcerated is also related to that earlier period of dramatic social instability and exposure to adverse childhood events including abuse.
We observed a reduction in probability of being incarcerated following a diagnosis of psychosis in Aboriginals diagnosed post-2000 compared with those diagnosed pre-2000 (Supplementary Figure 3). Despite this reduction, the proportion of Aboriginal patients with a current diagnosis of psychosis experiencing a period of incarceration remained high throughout the study period (Figure 2), possibly due to multiple and/or prolonged incarcerations.
We have previously reported the presence of high rates of combined alcohol and cannabis use in incidence cases of psychosis in Aboriginal and Torres Strait Islander populations (Gynther et al., 2019). In this study, we found a significant association with combined alcohol and cannabis use with incarceration, and a relative reduction in incident incarcerations and the aggregate number of patients in prison during the mid-2000s when controls on alcohol availability in Cape York were initiated and most consistently enforced. As diagnosis and first incarceration cluster temporally, it is tempting to infer that substance misuse leads both to incarceration and the emergence of psychotic symptoms. However, our data suggest that the relationship between substance use, psychosis and incarceration is more complex. Incarceration rates can be affected by government policy and by police and judicial discretion. The reduction in the proportion of Aboriginal patients incarcerated due to non-violent offences through the 2000s may have resulted from introduction and enforcement of alcohol control measures in Cape York. The cause of the persisting high proportion of Aboriginal male patients incarcerated due to violent offences during this same period needs further investigation but may reflect the increased risk of violent offending associated with psychotic disorder and persistent substance misuse other than alcohol.
A major limitation of our study is the lack of a comparison group of non-psychotic Indigenous patients and of the general Indigenous population from Cape York and the Torres Strait. Data regarding the incarceration rates of Indigenous people in Cape York and the Torres Strait, as distinct from the Queensland-wide rates, are unavailable. Social disadvantage and instability that contribute to high rates of psychosis in Cape York are also likely to result in increased general rates of incarceration. It is thus difficult to interpret the contribution of psychosis to the high rates of incarceration found in our study, which is crucial for the development of mitigatory policies and strategies. An additional limitation of our study is that it may be underpowered to detect significant differences, such as the disaggregated risks of alcohol and other drug use as predictors of incarceration among Indigenous people who received a diagnosis of psychosis. Our data linkage design substantially limits the possibility of attrition; however, moving is not common within this population and we do not anticipate any significant impact on findings. We searched public mental health service data to confirm psychosis diagnoses made by another service; however, there may have been some patients who went undiagnosed in community for a period of time prior to RAMHS being established. Similarly, for some patients, there may have been periods of incarceration prior to 1985 (the earliest date for which data is available).
Conclusion
Psychotic disorder is a health problem and warrants a health response. Our study found that for Aboriginal and Torres Strait Islander people with a psychotic disorder in North Queensland, criminal justice responses with resultant incarceration occurs frequently. It is crucial that Indigenous Australians with psychotic disorder access culturally safe and culturally informed mental health responses. This should be the case particularly when there is contact with the criminal justice system and early access could prevent the ‘predictable pathway’. Across Australia there is a dramatic shortfall in such services (Davidson et al., 2020). Access to appropriate mental health services and diversion options for Indigenous Australians with mental disorder who come into contact with police, courts and watch houses should be a key public health and justice priority, but is sadly lacking despite being highlighted three decades ago.
Supplemental Material
sj-pdf-1-anp-10.1177_0004867420985247 – Supplemental material for Incarceration among adults living with psychosis in Indigenous populations in Cape York and the Torres Strait
Supplemental material, sj-pdf-1-anp-10.1177_0004867420985247 for Incarceration among adults living with psychosis in Indigenous populations in Cape York and the Torres Strait by Fiona Charlson, Bruce Gynther, Karin Obrecht, Ed Heffernan, Michael David, Jesse T Young and Ernest Hunter in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-pdf-2-anp-10.1177_0004867420985247 – Supplemental material for Incarceration among adults living with psychosis in Indigenous populations in Cape York and the Torres Strait
Supplemental material, sj-pdf-2-anp-10.1177_0004867420985247 for Incarceration among adults living with psychosis in Indigenous populations in Cape York and the Torres Strait by Fiona Charlson, Bruce Gynther, Karin Obrecht, Ed Heffernan, Michael David, Jesse T Young and Ernest Hunter in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The clinician authors of this paper (B.G., E.Hu. and K.O.) are indebted to the Aboriginal and Torres Strait Islander patients and their families who have enriched their understandings of cultural diversity and strengths, and resilience in the face of adversity.
Author Contributions
E.Hu., K.O. and B.G. undertook data collection. F.C., B.G., E.He., E.Hu. and J.Y. were responsible for study design. F.C. and M.D. undertook statistical analyses. F.C., B.G., E.He., E.Hu. and J.Y. were responsible for interpretation of results. All authors were responsible for writing and editing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by Queensland Health who are the custodians of this database. The funder had no role in study design, data analysis, data interpretation, writing of the report or submission for publication. All authors had full access to all the study data. The corresponding author had final responsibility for the decision to submit for publication. F.C. is supported by an Australian National Health and Medical Research Council (NHMRC) Early Career Fellowship (APP1138488) and J.T.Y. receives salary and research support from an NHMRC Investigator Grant (GNT1178027).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.