
Abstract
Objective:
We consider insights from the second Australian National Survey of High Impact Psychosis (2010) in order to identify the key policy and service development implications.
Method:
The Survey of High Impact Psychosis (SHIP) provides an updated description of the experiences of people living with psychosis in Australia. We discuss the SHIP survey participants’ greatest challenges for the future in light of the strength of existing literature, highlighting prospective opportunities for policy and service planning.
Results:
Targets for future policy development and service initiatives are informed by the survey participants’ leading challenges: financial difficulties, social isolation, lack of employment, physical and mental ill health, accommodation, and access to services.
Conclusions:
Many of the areas of need identified by survey participants are supported by quality research that may be more widely translated into effective services. For areas of need where the evidence is lacking, more clinical research is urgently needed. A targeted approach is vital to secure necessary investment in the wider dissemination of efficacious interventions and their systematic evaluation in ordinary clinical practice, enabled by both research investment and active integration of the research effort within ordinary clinical settings.
Introduction
Among the psychoses, schizophrenia and bipolar disorder have been ranked among the top five causes of disease burden due to disability in those aged 15–44 worldwide, and together account for almost 10% of total disease burden in this age group (World Health Organization, 2001). In Australia, it is generally considered that nearly all people with these severe disorders are in treatment or have been treated at some time (Andrews et al., 2003), although definitive evidence for this is lacking. In contrast, people with the more common but less severe mental disorders, such as anxiety, depression and substance misuse, as surveyed by the Australian Bureau of Statistics in 2007 (Slade et al., 2009), often do not seek or receive treatment. Treatment for mental disorders can be expensive. The costs of treating the psychoses are particularly high, largely due to frequency of hospitalisation, and the costs of lost productivity are twice as high again (Carr et al., 2003). But there has often been dissatisfaction with treatment delivery systems.
A string of reports since the early 1990s has documented the plight of people with severe mental disorders in Australia and the shortcomings of treatment systems and other support services (e.g. Commonwealth of Australia, 1993; Mental Health Council of Australia, 2005). Media reports have repeatedly highlighted failings in mental health care for these people. The first National Survey of Mental Health and Wellbeing in 1997 strongly influenced the National Mental Health Strategy and led to Commonwealth policy initiatives such as a national primary mental health care initiative and the Better Outcomes in Mental Health and Better Access to Psychiatrists, Psychologists and General Practitioners programs (Whiteford et al., 2008). These developments were targeted mostly at improving the treatment rates for common mental disorders. On the other hand, the first survey of psychoses in 1997–98, the Low Prevalence (Psychotic) Disorders Study (Jablensky et al., 2000), together with its bulletins and over 40 journal publications, did not generate consistent national policy responses of similar scope or magnitude. National service reform for these disorders is more challenging as the responsibility for services has traditionally rested more with state and territory governments than the Commonwealth, and involves portfolios such as community services and housing as well as health. In 2006, the Council of Australian Governments (COAG) agreed to the National Action Plan on Mental Health 2006–2011 (COAG, 2006). This was the first time that all heads of government committed to ensuring coordinated care for people with severe mental illness and complex needs, people who are most at risk of falling through gaps in the service system. The plan had two flagships: coordinating care and governments working together. However, despite the initial optimism over this new policy direction, the flagships have not been formally evaluated and it is unclear whether either the flagships or the plan itself has made any impact on the lives of people with severe mental illness. Into this climate of uncertainty have stepped lobby groups representing various interests, not always advocating similar or complementary initiatives, and experiencing varying degrees of success in influencing policy and funding decisions. Mental health reform under these conditions is inevitably piecemeal and fragmented. While some sound initiatives may result, they not only need to be integrated within a comprehensive and coherent policy framework but, most importantly, effectively implemented and evaluated. This will be essential if the financial allocations announced in the 2011 Commonwealth budget for early psychosis services and for services to individuals with severe, persistent mental illness are to achieve the best possible outcomes.
Epidemiological data on the psychoses in Australia have the potential to provide important information for decision making in the areas of policy development and service planning for severe mental disorders. This was a key aim in undertaking the Survey of High Impact Psychosis (SHIP) in 2010, the main findings of which are reported in a government publication (Morgan et al., 2011) and in this journal (Morgan et al., 2012). Data are provided on prevalence, extent of disability, patterns of comorbidity, accommodation, service utilisation and treatments; that is, a snapshot of the extent of need in this population. Need, however, must be matched with initiatives of demonstrable effectiveness in reducing such need. This requires consideration of the quality and strength of evidence for interventions and other initiatives, which can then be translated into policies and service developments. Where such evidence is lacking more research is necessary, and if research is not feasible or timely then reason and ethical considerations based on the best available evidence must guide policy and service planning.
Despite the lack of a nationally coordinated policy response to the needs of people with psychosis, there have been changes taking place and it is important to keep these in mind when comparing the findings of the first psychosis survey in 1997–98 and the survey of 2010. This period has seen the primary mental health care reforms mentioned above and changes to the specialist mental health services, including a reduction in inpatient beds per capita, gradual expansion of early psychosis teams, policy to promote employment of people with disabilities, a dramatic increase in the number of community mental health clinical services and increased support services in the community such as the Personal Helpers and Mentors Program (Department of Health and Ageing, 2010). In addition, clinical presentation has been complicated by changes in exposure to illicit drugs (Sara et al., 2011) and options for clinical treatment have changed with proliferation of second-generation antipsychotics and the withdrawal of several of the older antipsychotics (Monshat et al., 2010).
The scope of psychosis in Australia
The SHIP survey used a two-phase design. Phase 1 was a psychosis screen to identify people likely to meet diagnostic criteria for a psychotic disorder in seven catchment areas of five Australian states who were in contact with public mental health services in the census month or in the 11 months prior to that month, or in contact only with non-government organisation (NGO) service providers during the census month. Phase 2 consisted of a structured clinical interview of a random sample (N = 1825), stratified for age, of those who screened positive for psychosis (N = 7955) in Phase 1 (see Morgan et al., 2012, for more methodological detail and discussion of the study’s limitations).
One-month prevalence estimates indicate there are some 43,800 people aged 18–64 years with psychosis who are in contact with mental health services and a further 6200 solely in contact with NGOs (Morgan et al., 2011). Of the total, 63% have an ICD-10 diagnosis of schizophrenia or schizoaffective disorder and the bulk of the remainder have affective psychoses. There would be additional numbers, not captured in this survey, treated solely in the private sector by general practitioners or psychiatrists, an unknown number in no current treatment at all, further cases in prisons 1 or among the homeless, and more lying outside the age range of the present survey. It is not known precisely how many people would fall into these categories, but 15,000 would be a conservative estimate (Morgan et al., 2011). Neither is it known what their profiles of need might be, and so the contents of this paper will be confined to what we do know about the 50,000 people with psychotic disorders in contact with public sector treatment services and NGOs.
The striking feature of participants in the survey is the wide range of variation that defies simple characterisation. For example, age at onset is less than 25 years in the majority of cases, but as many as one-third report onset after this age. Most cases begin gradually, but almost one-third have an acute onset. Most experience an episodic course, but 30% have a chronic continuous course. While often regarded as disorders predominantly of young people, almost 60% of cases are over the age of 35 years, highlighting the lifelong nature of psychosis for many people. In addition to delusions, hallucinations and high levels of negative symptoms, many patients report symptoms not traditionally identified with psychosis that are often overlooked, such as anxiety in various forms and depression. In spite of low educational achievement compared to the general population, almost half had obtained a post-school qualification of some kind. Although reliance on support benefits is high, almost one-third had been employed during the previous year, and while the majority report varying degrees of social disability, almost 18% had no disability or only mild difficulties.
Such variation indicates that a single sweeping policy initiative will be inadequate to meet the wide range of needs suggested by this diverse profile. The Commonwealth Government, anticipating that policy responses on a broad front were necessary, announced in May 2011 a number of measures for improving the lives of people with severe, debilitating mental disorders. These included the Care Facilitator initiative, expansion of the Support for Day to Day Living program, expansion of the Personal Helpers and Mentors service, adjustment of the Better Access Initiative and increases to the Early Psychosis Prevention and Intervention Centres (EPPIC) (National Mental Health Reform, 10 May 2011). It is important that these initiatives be coordinated, including with state services, when they are being provided as part of the overall care of an individual.
These programs require systematic evaluation for effectiveness, as with other mental health initiatives (Pirkis et al., 2011), in order to ensure that investments being made are adequately justified and, if necessary, the programs modified and/or expanded. Initiatives directed at children and youth (e.g. Schoollink, EdLiNQ, headspace) may have flow-on effects by detecting young people vulnerable to severe mental illness, helping to build resilience and providing early clinical care and treatment, all of which could help mitigate any subsequent onset of psychosis. Again, for similar reasons, thorough effectiveness evaluations ought to be built in as integral components of these programmes.
Challenges for people with psychosis
What is clear is that improved outcomes for people with severe mental disorders requires more than good clinical care. It has been recognised since the start of the National Mental Health Strategy that, at a minimum, a tripod of care – clinical treatment, stable accommodation and support services focused on recovery – is required (Whiteford, 1994). The coordinated care needed remains a policy and service reform challenge (COAG, 2006). Confirming the importance of the non-clinical needs, participants in the current survey identified the most important challenges facing them in the year ahead (Morgan et al., 2011, 2012). These are illustrated in Figure 1 and discussed in descending rank order below.
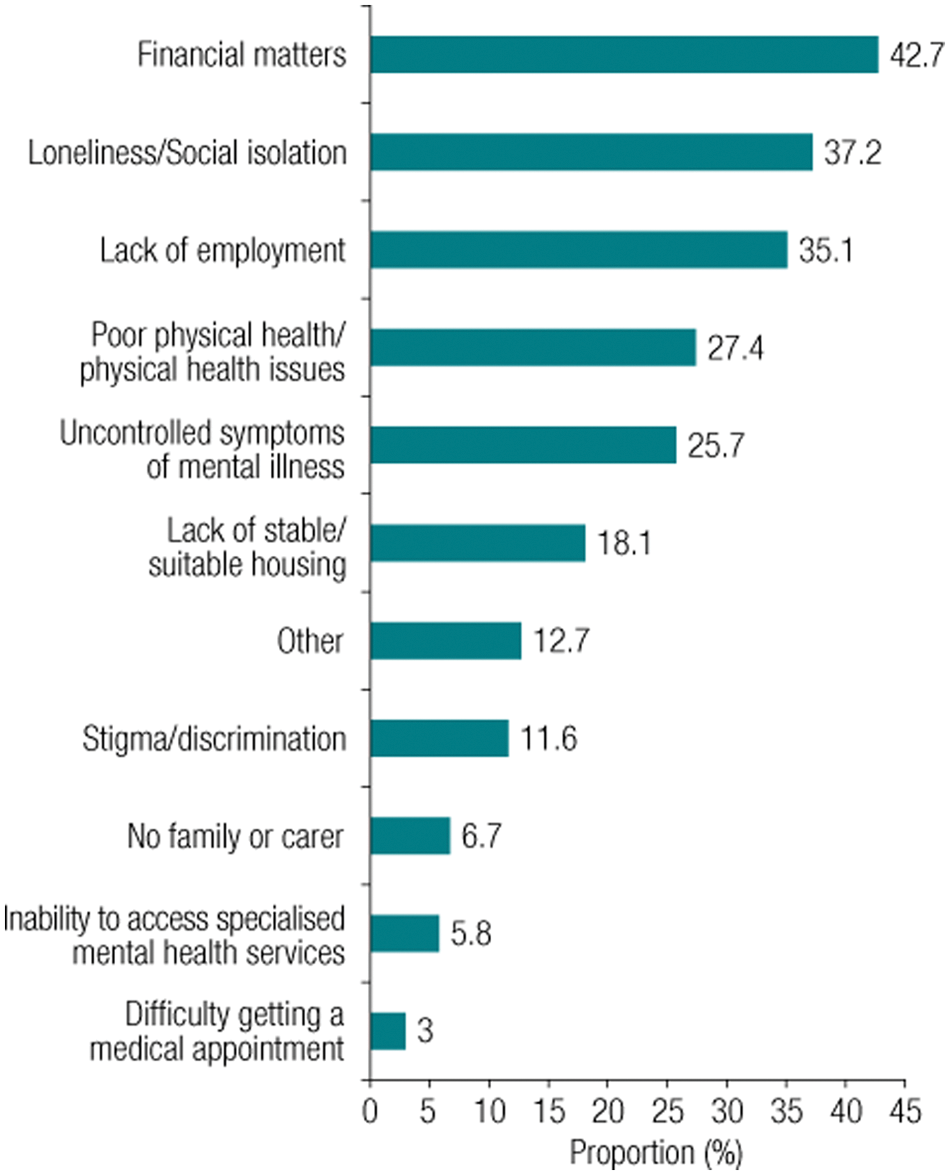
Challenges over the next year as identified by people with psychotic disorders.
Financial security
The leading challenge, identified by 43% of the survey sample, related to financial matters. Three-quarters of individuals with psychosis earn less than half the national estimated average disposable income, and the main source of income for 85% is the Disability Support Pension. Thus, many patients live in poverty, and are at risk of all of the adverse consequences of belonging to an underclass. Low disposable income implies limited capacity for expenditure on food, clothing, housing, utilities, and such items as private health insurance, expensive medications unavailable through the Pharmaceutical Benefits Scheme and ‘healthy lifestyle’ pursuits such as sport or other recreational activities. Indeed, around 9% of survey participants reported not receiving a necessary service because they could not afford the cost. These financial constraints need to be taken into account in any policy initiatives, and the use of public health and other government or NGO services ought to be assumed for the majority.
Tailoring programmes designed to provide financial counselling and budget management for people with mental disorders could help individuals with psychosis better manage their low incomes and maximise disposable income. This is especially the case where individuals are unaware of benefits or service discounts for which they are eligible. However, as discussed below, access to remunerated employment, even if very limited, would be the most effective means of addressing the problem of low income and financial challenges.
Social exclusion
Loneliness and social isolation were common in those surveyed, with almost half never having been in an enduring intimate relationship and 13% having no friends at all. Underpinning social exclusion is an impairment in socialising abilities, reported by 63.2%; psychotic illness interferes with establishing and maintaining relationships (Fett et al., 2011). Such impairment has been attributed to deficits in social cognition (Penn et al., 2008), that is, difficulties in detecting, correctly interpreting and responding appropriately to social cues. Deficits of social and emotional perception have broad implications for day-to-day social interactions and community participation (Fett et al., 2011). There are numerous innovative approaches to increasing social participation among people with psychosis (Kurtz and Mueser, 2008) that deserve broad implementation, but there remains a clear unmet need for effective policy initiatives addressing impairments in social functioning.
Policy initiatives aimed at increasing social support and enhancing social inclusion for people with psychosis, such as the provision of opportunities to meet and engage socially in a variety of contexts, will not succeed as well as expected unless fundamental impairments in social cognition are taken into consideration by those who provide such opportunities. A growing body of research has begun to map the nature of deficits in social cognition in individuals with psychosis (Hoekert et al., 2007; Penn et al., 2008), and this could be used to inform policy development in this area. Moreover, early investigations have shown some benefits for therapeutic remediation of social cognition with modest improvements in social behaviours (Horan et al., 2008). Treatment and rehabilitation services could integrate and apply this growing body of knowledge in their clinical care plans, preferably early in the course of illness before social skills deficits become well established and habitual (Hoekert et al., 2007). However, it must be recognised that knowledge of treatment efficacy in this domain is comparatively new and has many gaps (Horan et al., 2008). Further research is required to identify the specific interventions that have greatest efficacy and can be applied in clinical services.
Lack of employment
Employment rates were much lower than in the general population (around 65%), with 32.7% having been in paid employment in the past year and 21.5% at the time of interview. This supports existing Australian literature suggesting that labour force non-participation may reach 75% among people with psychotic disorders (Waghorn et al., 2004). Paid employment has not only the potential to increase disposable income and thereby help to address the leading challenge for people with psychosis, namely financial difficulties, but it is also an important form of community engagement that brings with it a degree of self-esteem and sense of self-efficacy (Marwaha and Johnson, 2004). There is a sound evidence base for the effectiveness of supported employment programmes using an individual placement and support model (Campbell et al., 2011). Although typically applied to those with well-established disorders, there is some evidence for the effectiveness of this approach in the context of first-episode psychosis as well (Killackey et al., 2008; Rinaldi et al., 2010). Data from the EPPIC services (Killackey et al., 2006) suggest that this population is less likely to be dependent on disability pensions or other sources of support, and so may have greater inclination to seek employment. The model can also be applied to education and training as well as employment (Bond et al., 2001). However, these interventions are not as widely disseminated in Australia (Waghorn, 2011; Waghorn and Lloyd, 2005) as the evidence of their effectiveness suggest that they ought to be. Consequently, there is much scope for service enhancements in this field and the potential for improvement through ongoing evaluations of their effectiveness. In parallel with supported employment programmes, efforts are required to reduce structural barriers to employment and financial disincentives for people on disability support to transition to paid employment.
Poor physical health
People with psychosis have poor nutrition and are affected by physical ill health at rates far above those of the general population and, according to the literature, have high rates of premature mortality (Saha et al., 2007). A recent study showed life expectancy was reduced by 18.7 years for men and 16.3 years for women with schizophrenia, and 13.6 and 12.1 years for men and women with bipolar disorder (Laursen, 2011). There is a major effort under way to close the gap in life expectancy between Indigenous Australians and the general population (currently 11.5 years for males and 9.7 years for females) (Australian Bureau of Statistics, 2009). There could be little argument that a similar high-profile effort is needed for Australians with psychosis. The overall improvements in mortality that have been made with the general population in Australia in the last century have not been reflected in people with mental disorders (Doessel et al., 2010).
Amongst the current survey participants, half had metabolic syndrome, a quarter were at high absolute risk of cardiovascular disease in the next 5 years, 45% were obese, a third reported no or very little daily physical activity, and two-thirds smoked tobacco. As recently highlighted in The Lancet, there should be no mental health without physical health (The Lancet, 2011). Antipsychotic medications, particularly some of the newer ones, are known to contribute to weight gain and the metabolic syndrome (Foley and Morley, 2011; Newcomer and Haupt, 2006), but their contribution to premature mortality is not yet decided (Weinmann et al., 2009).
Although several Australian states have introduced programmes aimed at addressing the physical health problems of people with psychosis, these are yet to be evaluated for effectiveness. There is not a great deal of evidence in the published literature about how best to approach physical health problems among people with psychosis. While extrapolating from the literature on treating these vital health matters in the general population is a reasonable place to start, more research is required to determine what works more effectively in the psychosis population, given its special characteristics, including the use of antipsychotic drugs. Clearly, baseline and regular monitoring of blood pressure, body mass index, waist circumference, and fasting blood glucose and lipids would be the bare minimum standard requiring universal implementation. Beyond this, there is high-quality evidence for the effectiveness of cognitive behavioural therapy and nutritional counselling for both weight reduction and the prevention of weight gain (Álvarez-Jiménez et al., 2008), but somewhat less robust evidence for the effectiveness of psychoeducational therapies, dietary advice and exercise plans (Lowe and Lubos, 2008). Interventions along these lines ought to be widely available and systematically evaluated in real-world clinical settings because there is no single intervention that stands out clearly as uniformly effective. Less conclusive evidence supports the use of pharmaceutical treatments for weight gain (Faulkner et al., 2007). Drugs such as metformin and lipid-lowering agents ought to be provided as indicated for the general population with metabolic abnormalities, but their particular effectiveness in the psychosis population requires more research to determine whether they are more or less effective in this group.
There are treatment guidelines incorporating algorithms to help clinicians tackle the complex area of metabolic abnormalities in psychosis, including early psychosis in young people (Curtis et al., 2011; Stanley and Laugharne, 2011) and these ought to be widely implemented and systematically evaluated. The high rates of other medical problems reported reinforce the importance of the patient’s general practitioner in addressing physical morbidity in this population and also the importance of gaining access to relevant medical specialists in a timely fashion.
Mental health
The burden of poor mental health in psychosis encompasses inadequately controlled symptoms (both psychotic and non-psychotic), medication side effects, impairment in activities of daily living, difficulties in socialising and deficits in cognitive functioning. Suicidal thinking and suicidal behaviour are both highly prevalent and were reported by 67% and 50% of participants, respectively. Furthermore, substance use is widespread; 66% smoke tobacco, and lifetime alcohol and other drug abuse or dependence was identified in 50% of cases, a dramatic increase since the psychosis survey of 1997–98. These proportions are very much higher than the general population.
(a) Medication was being taken by over 90% of the sample; 63% were taking more than one class of medication and 27% were taking at least two different antipsychotics. The majority reported some relief from medications, notwithstanding the high rates (77%) of side effects, frequent weight gain and extrapyramidal symptoms. In spite of the well-demonstrated efficacy of medications used in the treatment of psychosis (Leucht et al., 2009), psychotic symptoms often persist, non-psychotic symptoms are common, and medications are of little or no benefit for negative symptoms (Murphy et al., 2006) or cognitive deficits (Woodward et al., 2005). While efficacy is demonstrated in clinical trials of highly selected patients prior to government approval and marketing, such trials often have limited generalisability to a wider psychosis population, and post-marketing effectiveness trials are rare. Consequently, there is little evidence to guide clinicians working in real-world clinical settings. There is a lack of high-quality evidence for individualised options concerning drug choice in relation to differential effectiveness and experience of adverse effects, as well as for widespread polypharmacy, where various drug combinations may be prescribed based on very limited information (Correll et al., 2009). Greater understanding of the influence of factors such as patient characteristics on treatment response may assist the development of more systematic, tailored treatment guidelines (Kane and Correll, 2010, Weiden et al., 2007). There is thus enormous scope for conducting pragmatic clinical trials to improve the evidence base for optimal prescribing by clinicians and to improve patient outcomes, especially the risk to benefit ratio (March et al., 2010; Tunis et al., 2003).
(b) Where medications clearly have limitations the role of psychosocial interventions takes on considerable importance. Cognitive behaviour therapies are demonstrably efficacious adjuncts to drug treatment for psychotic symptoms (Pfammatter et al., 2006) as well as for comorbid depression and anxiety (Lawrence et al., 2006), although the longer-term outcomes are less clear, and their efficacy for negative symptoms is uncertain (Jones et al., 2004), notwithstanding some promising recent research (Grant et al., 2012). Behavioural family interventions have well-established efficacy for reducing relapse and improving symptoms (Pfammatter et al., 2006). Cognitive remediation for cognitive deficits shows promising evidence for benefit (McGurk et al., 2007). Notwithstanding this range of evidence, the SHIP data indicate that less than a third of participants received counselling, less than a quarter received cognitive behaviour therapy and only 10–15% received family intervention. Although between 1997–98 and 2010 there have been increases in outpatient/community clinic contacts (75% to 93%) and participation in community rehabilitation/day programmes (23% to 37%), the rates with which the foregoing interventions of known efficacy have been delivered are not clear but appear to have remained unsatisfactorily low. Improvements in access to such treatments could be a future goal.
(c) Substance abuse/dependence comorbidity has risen dramatically, from around 30% to more than 50% since 1997–98 and tobacco use remains extraordinarily high. Although there has been an increase from 2% to 12% since 1997–98 in patients accessing drug and alcohol services or programmes, the literature on treatments for substance use disorders in psychosis provides moderate to low quality evidence for little or no efficacy of treatments in reducing substance use in this population, including both pharmaceutical (Wobrock and Soyka, 2008) and psychosocial therapies (Cleary et al., 2008). Results of intervention studies for reducing or quitting smoking are similarly disappointing, showing only short-term benefit of bupropion for reducing smoking, and limited efficacy of a variety of psychosocial treatments for nicotine dependence in schizophrenia (Tsoi et al., 2010). Therefore, because substance use is a growing problem and one that is associated with a number of adverse outcomes in psychosis (Archie and Gyomorey, 2009), novel or improved treatments need to be encouraged and accompanied by thorough evaluations of their effectiveness. It cannot be assumed that generic quit smoking programmes and other drug or alcohol prevention and interventions programmes suitable for the general population (e.g. varenicline is potentially harmful in people with mental illness) are suitable for people with psychosis. Services need to be developed that are better tailored to the special characteristics of this group.
(d) Lifetime suicidal thinking and behaviour were reported in the survey at 67% and 50%, respectively, and the population lifetime risk of suicide for people with psychosis has been estimated at about 5% (Hor and Taylor, 2010). The literature on reducing suicide rates in psychosis shows no robust evidence for the effectiveness of any particular form of intervention (Asenjo Lobos et al., 2010; Pharoah et al., 2006), and therefore any initiatives to reduce suicide in this population require rigorous evaluation, with clinicians in the meantime continuing to treat depression and remaining vigilant for risk indicators (Hawton et al., 2005).
Accommodation
Not only does stable housing enhance a person’s security and quality of life, it helps ensure access to services. If services cannot locate a person because of residential instability, continuity of care is impossible. Ongoing clinical care and support services are often vital to ensure individuals with psychosis can remain stable and on a trajectory towards improved functioning.
Improvements in the pattern of housing compared to 1997–98 were observed, with more people in their own home or rented accommodation, a doubling of the proportion in supported housing and a halving of the proportion that had been homeless. However, a lack of stable or suitable housing was identified by 18% of participants as a key challenge for the future. The survey findings reflect the partial effectiveness of housing initiatives over the past decade, and clearly point to the critical importance not only of their continuation but further expansion.
Stigma and discrimination
Stigma or discrimination was experienced by 38% of study participants and was reported more frequently by women than men. In around one-fifth of the sample the fear of stigma or discrimination, or the actual experience of these phenomena, stopped people from doing some of the things they had wanted to do.
Negative attitudes and behaviours towards the mentally ill appear to be associated with biogenetic causal beliefs in general populations and among health professionals whereas psychosocial explanatory beliefs are associated with more positive attitudes (Read et al., 2006). Self-stigmatisation is the consequence of individual acceptance or ‘internalisation’ of these negative attitudes. The science is generally better at measuring stigma, its correlates and consequences (Livingston and Boyd, 2010; Mak et al., 2007) than interventions to reduce it. Actions to reduce stigma are diverse and probably have an influence to some degree, but there is no consensus on the most effective approaches for the diverse contexts and targets of anti-stigma programmes, and the published evidence is insufficient to give clear policy direction here. Indeed, ‘there is still much to be done to provide an empirical basis for evidence-based interventions’ in this field (Angermeyer and Dietrich, 2006).
Service utilisation
There have been substantial improvements in patterns of service use with increases in use of outpatient/community clinics and community rehabilitation/day programmes, allocation of case managers, care provision by general practitioners and service provision by NGOs. What is less clear is the extent to which these services are providing interventions with a sound basis in empirical evidence. The low rates of cognitive behaviour therapy, for example, suggest that there may be considerable scope for ensuring that such interventions are provided more widely than currently appears to be the case.
Annual rates of inpatient admissions for mental health reasons have declined from 59% to 38% and involuntary admissions from 31% to 23% since 1997–98. The extent to which reductions in bed availability and increases in use of community services over this time have contributed to this pattern is not clear because cause and effect cannot be disentangled. However, it is clear that hospital admissions remain significant and constitute an important component of the spectrum of services required in treating psychosis. We have little systematically collected information on the level, quality and effectiveness of care provided by inpatient units for people with psychosis, who happen to be overwhelmingly the main users of specialised mental health inpatient services (Carr et al., 2008). While quality of care is likely to vary across units, there are data to suggest that some inpatient facilities are working under considerable strain with high levels of involuntary admissions and unacceptable rates of aggressive behaviour and other adverse incidents (Carr et al., 2008), with these therapeutic environments becoming ‘toxic’ as a result (Lewin et al., 2011). To respond to this serious problem, an audit of a representative sample of psychiatric inpatient facilities could be undertaken with a re-examination of the roles and functions of inpatient care so that hospital and community mental health services can be better planned to complement and support each other in the future.
Parenting
A remarkable finding of the survey was that 56% of females and 26% of males were parents and a substantial proportion (24% of females and 6% of males) had dependent children of their own (or stepchildren) living with them, with the majority of mothers being the primary carers for their children. Such children would be regarded as at risk of mental ill health and also a potential source of stress for the parent with psychosis, particularly if the child has developed mental health problems. Campbell and colleagues (2012), in this issue, have shown that 17% of fathers and 25% of mothers are caring for children with behavioural or medical problems. There is clearly scope for preventative interventions in this context. Programmes for children of parents with a mental disorder have been established in some jurisdictions, but what constitutes an effective form of intervention has not been established (Reupert and Maybery, 2009) and there is clearly scope for evaluating new initiatives in this area that benefit both the parents and children.
Early intervention
Use of early intervention psychosis programmes was reported by 8.4% of the participants (16.8% in the 18–34 age group). The term ‘early intervention’ has different meanings in different contexts. In the context of ‘early in illness’ it means detection and best practice treatment of the first stages of psychosis, attempting to reduce the duration of untreated first-episode psychosis on the premise that the shorter the duration, the better the outcome (Marshall et al., 2005). While high-quality integrated treatment in the early stages of psychosis is associated with improved outcomes in the short term (Marshall and Rathbone, 2011), medium to longer term outcomes, beyond the first 2 years, do not appear to be any better than for ‘standard treatment’ (Bertelsen et al., 2008). The effectiveness of high-quality interventions and support maintained beyond the early stages of the disorder is not yet entirely clear, however early trials seem to point toward a positive effect of longer duration of high-quality intervention (Norman et al., 2011). It would have to be an extraordinarily powerful early intervention indeed to make a long-term difference in the years after it was withdrawn, and to expect as much is unrealistic. There are not many treatments in medicine for recurring or chronic illnesses with this level of efficacy. However, the EPPIC service model is important in several respects. First, it is a self-evident good to relieve suffering, where possible, sooner rather than later. Second, it has demonstrable short-term benefits. Third, it usually provides a gentler, less traumatic entry to mental health care than an acute psychotic crisis and involuntary hospitalisation. Fourth, its early benefits might be maintained for longer if high-quality treatments and support are sustained over time. Thus, the philosophy and model of care developed by EPPIC needs to be translated into continuing service provision beyond the early years of the disorder, and evaluated systematically.
Another shade of meaning of early intervention derives from the fact that most psychotic disorders have their onset in adolescence or early adulthood. This is the ‘early in life’ context. But the survey data show that one-third of the psychoses begin after the age of 25, the usual age cut-off for EPPIC-like services. Apart from the arbitrariness of such a cut-off, there is a problem of equity here in that an older person ought to be as entitled to the benefits of early psychosis intervention as a younger person. After all, one’s health is just as important to the individual regardless of age. Thus, the EPPIC philosophy and model needs to be adapted and extended to other age groups and its effectiveness tested in this context.
The early intervention term has also been applied to the period before the onset of psychosis, the ‘early pre-illness’ context. This has entailed identification of people at ‘ultra-high risk’ of psychosis or with ‘at risk mental states’ (Yung et al., 2005), a concept that has evolved into the DSM-5 draft ‘psychosis risk syndrome’ (DSM, 2010). Such individuals usually have genuine mental health problems requiring clinical care, are help-seeking, and may benefit from various treatments tailored to those problems in the short term (De Koning et al., 2009). However, the subset that actually go on to develop a psychotic disorder cannot be identified with sufficient reliability to justify antipsychotic drug treatment, with all of its attendant risks of harm, particularly to the 50–80% who will not go on to develop psychosis (Corcoran et al., 2010; Nelson and Yung, 2011). This is very definitely an area that requires more research, and interventions designed to delay or prevent the development of psychosis must be treated as experimental, an important subject for research, but not the domain of ordinary clinical practice.
Conclusions
There are encouraging signs of change for the better on several fronts since 1997–98. The course of illness appears to have shifted in a favourable direction in which more have experienced an episodic course with good inter-episode recovery and fewer have reported a chronic course with deterioration. Use of community-based health services has increased, and hospital (including involuntary) admissions have declined. Use of NGO services has also increased, although we need a stronger evidence base to justify the growing investment in these services (Siskind et al., 2011). There have been improvements in the pattern of accommodation. Features that seem to have remained the same over the past decade include financial disadvantage, low employment rates, social isolation and loneliness. New problems have emerged or been documented for the first time at a population level in Australia, including alarmingly high rates of physical health problems and increases in substance abuse/dependence. While use of atypical antipsychotics has increased, side effects remain a substantial problem that often impair functioning, and the limitations in the effectiveness of these drugs are highlighted by the persistence of symptoms, continuing levels of disability and significant cognitive impairment. Psychosocial interventions with a strong evidence base do not appear to be nearly as widely deployed as they should be.
We have identified potential areas of policy and service development where we could be doing better by more widely implementing those interventions we already know to be effective. Increasing access to such evidence-based treatments is partly a problem of adequate resources and partly a problem of clinical governance. It is not sufficient merely to increase resources to enhance the availability of effective interventions; sound clinical governance is also required to ensure that those resources deliver what is intended and outcomes are measured.
On the other hand, there are problems for which effective interventions are unknown or uncertain, and for which basic and clinical research is urgently needed. A recurring theme in this paper has been the need for systematic evaluations of the effectiveness of various interventions and there is a clear need for clinical research to be integrated more widely and effectively into routine service provision to ensure that this can occur.
Over the past 25 years there have been steady improvements in mortality and survival rates among women with breast cancer, a disease that has been stigmatised in the past, like psychosis today. These improvements have been due not to a dramatic curative breakthrough but to a combination of earlier detection through public education and increased awareness, incremental improvements in clinical practice, technological and treatment advances and wider availability of treatments. Much of this has been underpinned by clinical trials. Mental health could well take a leaf out of this book. Evidence is building that a coordinated approach at a population level to promote early detection of severe mental disorder is effective and service developments should reflect this. We need to continue to systematically examine the effectiveness of existing treatments and combinations of treatment in ‘real-world’ settings, invest in testing novel treatment approaches and extend the reach of clinical services to all communities. In this way, we could emulate the successes that have been achieved with breast cancer. This would require both research investment and active integration of the research effort within ordinary clinical settings. It is time to take that step by making a national investment in mental health clinical trials and service evaluation infrastructure, ideally administered by a national institute established for this purpose; this would bring benefits measurable in the next national survey of psychosis 10 years from now.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis (SHIP). The members of the SHIP Study Group are: V. Morgan (National Project Director), A. Jablensky (Chief Scientific Advisor), A. Waterreus (National Project Coordinator), R. Bush, V. Carr, D. Castle, M. Cohen, C. Galletly, C. Harvey, B. Hocking, A. Mackinnon, P. McGorry, J. McGrath, A. Neil, S. Saw, H. Stain. Ethics approvals for the study were obtained from relevant institutional human research ethics committees. This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Notes
Funding
This paper did not receive any specific funding. The original SHIP study was funded by the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.