
Abstract
Psychotic disorders constitute a worldwide public health problem. According to World Health Organization/World Bank estimates [1], no less than 25%% of the total ‘burden of disease’ in the established market economies is at present attributable to neuro-psychiatric conditions. Measured as a proportion of the disability-adjusted life years (DALYs) lost, schizophrenia, bipolar affective disorder and major depression together account for 10.8%% of the total, and inflict on the community losses that are comparable to those due to cancer (15%%) and higher than the losses due to ischaemic heart disease (9%%). The life-time risk for schizophrenia, according to the WHO 10-country study [2], is in the range of 0.50–1.72%% and varies little across diverse populations and cultures. However, schizophrenia is only part of the spectrum of morbidity associated with the psychotic disorders which, as a group, share a range of symptoms and a tendency to a lifelong, chronic or recurrent course. Persons with such disorders tend to experience significant behavioural and personality disorganisation and long-term dependency on treatments and services. Thus, bipolar disorder and unipolar major depression with psychotic features may be more akin to schizophrenia in their course and outcome than to the non-psychotic affective disorders.
The clinical and public health significance of the psychotic disorders (which, in the public perception, epitomise ‘mental illness’) increases during the transition from predominantly institutional to predominantly community-based care for people living with such disorders. Being in the first echelon of this global transition, the Australian health services (and society as a whole) face the entire gamut of problems associated with the fundamental changes in values, attitudes, required professional skills and principles guiding resource allocation that accompanies the ‘third psychiatric revolution’. The National Mental Health Strategy, which chartered the way of the transition, is clearly in need of up-to-date epidemiological information on this important group within the population. Although estimates of the prevalence, incidence and lifetime risk of psychotic disorders can, arguably, be extrapolated from research done elsewhere [3],[4], such extrapolations tend to be too general, lack essential socioeconomic, clinical and service provision context, and are therefore of limited usefulness for specific policy and planning decisions. To generate an up-to-date evidence base of psychotic disorders in Australia within the framework of the National Survey of Mental Health and Wellbeing [5], the present study was designed to: (i) estimate the point and period prevalence of psychoses in urban areas; (ii) identify profiles of current and lifetime symptoms, impairments and disabilities associated with psychosis; (iii) gather information on services received and needed; and (iv) explore aspects of quality of life in a broadly representative sample of people with psychotic illnesses. This communication provides an overview of the methods and main results. Detailed descriptive statistics from the study and its findings are available in Jablensky et al. [6].
Design and methods
The study was conducted over four urban or predominantly urban sites in the Australian Capital Territory (Canberra); Queensland (a sector of Brisbane and contiguous peri-urban and rural localities); Victoria (two inner-city areas in Melbourne); and Western Australia (an inner-city area and several suburbs in Perth).
The total population of these areas within the age range 18–64 (estimated resident population, 30 June 1997) was 1 084 978. In terms of the Index of Relative Socioeconomic Disadvantage [7], the four sites were only marginally more advantaged compared with the national median.
The inclusion criteria were set so as to identify and recruit people aged 18–64 with psychotic disorders that could be classified according to ICD-10 as: schizophrenia (F20); schizoaffective disorders (F25); manic episode with psychotic symptoms (F30.2); bipolar affective disorder with psychotic symptoms (F31.2, F31.5); severe depressive episode with psychotic symptoms (F32.3); recurrent depressive disorder with psychotic symptoms (F33.3); persistent delusional disorder (F22); acute or transient psychotic disorder (F23); or other and unspecified non-organic psychotic disorder (F28, F29). Brief psychotic episodes secondary to psychoactive substance intoxication or a medical condition were excluded. Other exclusion criteria were: temporary visitor status in Australia; significant cognitive deficit (dementia or moderate to profound intellectual handicap); severe communication impairment (e.g. post-stroke aphasia); residence in a nursing home or prison; and inability to communicate in English to a degree allowing a valid interview.
The core of the study was a two-phase survey. The first phase involved a census of all individuals who made contacts with ‘mainstream’ mental health services during a period of 1 month (30 consecutive days between June and September 1997) and a screening procedure which aimed to select persons with psychotic disorders. Here and in the subsequent text we use the term ‘mainstream’ to denote the predominantly public, specialist psychiatric inpatient, outpatient and day patient services, as distinct from the services provided, on one hand, by general practitioners or psychiatrists in private practice, and, on the other hand, by social, welfare, and other ancillary services and agencies. In the second phase, a stratified random sample of the screen-positive individuals within each of the major recruitment sources was selected for interview to gather data on current and lifetime symptoms, sociodemographic characteristics, impairments in daily life, use of services, and unmet needs. In addition to screen-positive users of the mainstream services, sampling for interview also involved special groups: (i) persons with psychotic disorders under the care of general practitioners or private psychiatrists; (ii) persons of no fixed abode or in marginal accommodation; and (iii) persons with previous service contacts but not in contact with the services in the census month.
The screening protocol developed for the study, the Psychosis Screen (PS), included a set of six questions targeting specific psychotic symptoms (current or at any time in the past) and an item recording the clinical judgement of the key worker administering the PS as to whether, on the basis of all information available, psychotic symptoms were present and the case met the criteria for inclusion. Following a pilot study on 116 patients of whom one-third had a documented history of psychotic episodes, a cut-off at two or more positive screen items was selected as the threshold of ‘caseness’. With sensitivity and specificity at 0.67 and 0.84, respectively, the positive predictive value (PPV) of the screen was 0.70 and the negative predictive value (NPV) 0.80. In instances where the key workers felt unsure whether to score 1 or 2, they were instructed to include rather than exclude the case. All doubtful instances were reviewed with the field work supervisor.
The main assessment tool was the Diagnostic Interview for Psychosis (DIP), a semistructured, standardised interview consisting of three modules: (i) demography and social functioning; (ii) diagnostic module (OPCRIT-SCAN); and (iii) service utilisation. The DIP incorporates elements of internationally established instruments such as the Operational Criteria for Psychosis (OPCRIT) [8]; the WHO Schedules for Clinical Assessment in Neuro-psychiatry (SCAN) [9]; and the WHO Disability Assessment Schedule (DAS) [10]. The DIP is therefore capable of generating data that are comparable with those produced by researchers in other parts of the world.
The DIP was designed for use by a variety of mental health workers, including psychiatrists, clinical psychologists and nurses. As the majority of the interviews were to be conducted by research nurses, training procedures were implemented to ensure quality and reliability of the assessments. In addition to training within each centre, inter-centre workshops were conducted in which 14 interviewers jointly rated videotapes of DIP interviews and calibrated each other's ratings against the glossary criteria and the clinical judgement of an expert panel of psychiatrists. Inter-rater reliability was assessed in the course of the field interviews and the level of diagnostic agreement achieved among interviewers was acceptably high (generalised kappa of 0.73 for ICD-10 diagnoses).
Prevalence of psychotic disorders across the four sites
Prevalence is an estimate of the total number of individuals who manifest a disorder at a specified time (or during a specified period) divided by the population at risk at that given time. All rates refer to any ICD-10 diagnosis of schizophrenia, schizoaffective disorder, delusional and other psychoses, bipolar disorder, mania or severe depression with psychosis. Four sets of estimates were generated from the census and the ‘special focus’ studies: (i) point (1-month) prevalence rate of persons with ICD-10 psychotic disorders making contact with mainstream inpatient and outpatient services; (ii) point (1-month) prevalence rate of persons with ICD-10 psychotic disorders making contact only with services provided by private psychiatrists and general practitioners; (iii) period (12-month) prevalence rate of persons with ICD-10 psychotic disorders making contact with mainstream inpatient and outpatient services; and (iv) point (1-month) prevalence rate of persons with ICD-10 psychotic disorders who are marginalised or homeless and not identified in other service settings. As the psychotic disorders included in this study tend to be persistent, and a change of status from caseness to non-caseness within 1 month would be an exception rather than the rule, we assume that prevalence rates calculated on the basis of a census month and on the basis of a census day are practically identical. Therefore, we refer to the 1-month prevalence as point prevalence.
Estimated prevalence of ICD-10 psychotic disorders by service type (rate per 1000 of estimated resident population aged 18–64)
Estimated prevalence of ICD-10 psychotic disorders by catchment area (rate per 1000 of estimated resident population aged 18–64)
Characteristics of the interviewed sample
The interviewed sample of 980 individuals included 586 men and 394 women. The percentage born overseas (24.1%%) was close to the figure for the Australian general population (23.0%%) [11]; 3.7%% of the sample were of Aboriginal or Torres Strait Islander descent, slightly higher than Australian Bureau of Statistics population estimate for 1996 of 2.1%% [12]. The majority of the interviewed sample (70.1%%) was recruited through the mainstream mental health services, including 26.8%% inpatients and 43.3%% outpatients. Another 173 participants (17.7%%) were recruited through their general practitioners or private psychiatrists. Lastly, 120 persons (12.2%%) of no fixed abode or living in marginal accommodation in the study areas (and not identified through treatment services in the census month) were recruited through shelters or community aid services for the homeless.
Distribution of screen-positive and interviewed samples by source of recruitment (%%)
Diagnostic distribution
Although the majority of the participants had been diagnosed at the time of previous service contacts, each participant in the study had a face-to-face research interview which produced a criterion-based diagnosis using the computerised OPCRIT algorithm. In terms of ICD-10, schizophrenia and schizoaffective disorders accounted for 62.4%% of the 1-month census sample. A further 19.5%% were diagnosed with bipolar mania or depression with psychotic features and 14.8%% were assigned to the category of other non-organic psychosis. The remaining 3.3%% did not meet at interview the ICD-10 criteria for one of the above diagnoses but were retained in the study sample on grounds of other clinical information suggestive of psychosis. The diagnostic distribution of the sample in terms of DSM-III-R was, by and large, similar to the ICD-10 classification with 80.0%% of the sample being assigned to the same diagnostic category by the two systems (Fig. 1).
Distribution of disorders by diagnostic classification system. □, ICD-10; ▪. DSM-III-R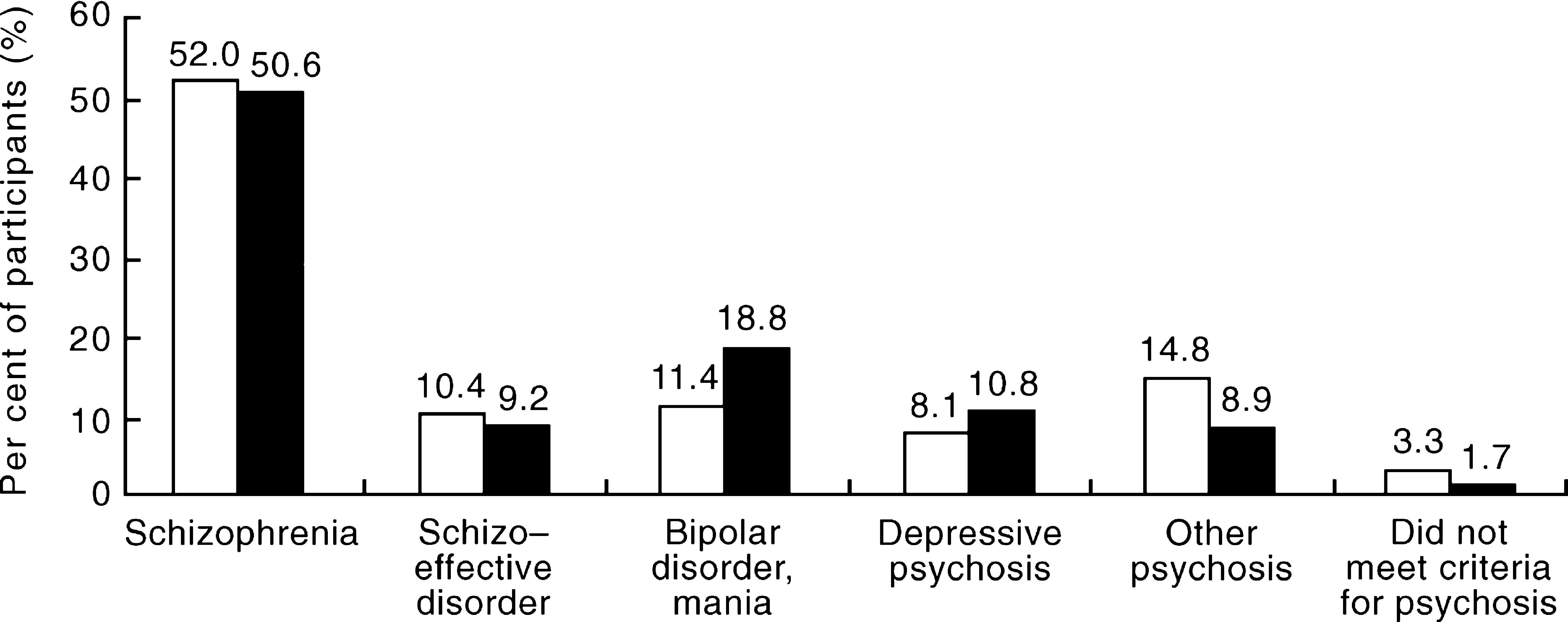
Length of illness and pattern of course
The mean length of illness prior to interview was 15.1 years. The majority had a history of illness spanning 10 years or more and only 19.8%% had had a first onset of psychotic illness within the previous 4 years. In the majority, the onset of psychotic symptoms was in the early to mid-twenties, with the exception of those with depressive psychoses where the mean age at onset was in the late-twenties. Females tended to have a later onset than males, but the difference was not statistically significant. There were no significant differences in mean age at onset between the four study sites.
In terms of longitudinal pattern of course, the psychotic illness was chronic or recurrent with incomplete remissions in 70.8%% of the cases. Deterioration of functioning, compared with the peak level achieved prior to onset, was present in 79.5%%. Nevertheless, a sizeable minority (20.7%%) had had periods of complete remission and 8.5%% had experienced a single episode of psychosis followed by a stable remission.
Symptom profile: present and lifetime
In the majority of the patients, the present mental state (including the 4 weeks prior to interview) was dominated by delusions (48.8%%) and hallucinations (36.1%%). These two symptoms also occupied the highest rank in lifetime symptomatology. Persecution and reference were the most common delusional themes, and voices of a derogatory, accusatory or per-secutory nature were the most typical content of the auditory hallucinations. Varying, but generally high, percentages of the patients had experienced first-rank (Schneiderian) symptoms of thought interference and will replacement. In 50.6%% of the subjects, the experience of positive psychotic symptoms was accompanied by a compelling sense of reality and poor insight. Affective symptoms were also common: current depressed mood or dysphoria was present in 23.1%% (73.1%% lifetime); anhedonia in 21.1%% (65.4%% lifetime); and suicidal ideation in 18.2%% (67.7%% lifetime). Mania or hypomania was less common (5.5%% present state and 34.8%% lifetime).
The negative symptoms characteristic of schizophrenia and related disorders were less prominent on mental state examination (restricted or blunted affect was observed during the interview in 28.8%%, and less than 10%% showed extreme poverty of thought or speech). Since such symptoms were rated only on the basis of a limited sample of behaviour (observation during the interview), the percentages are likely to underestimate the actual presence of negative symptoms. However, the behavioural impairments described below provide indirect evidence of a higher frequency of deficit symptoms.
Substance-use comorbidity
Psychoactive substance abuse emerged as a major comorbidity problem among people with psychotic illnesses. Current smoking was reported by 73.2%% of the men and 56.3%% of the women in the study (compared with 27.3%% and 20.3%% in the general population of Australia according to the 1995 Australian Bureau of Statistics National Health Survey [13]). The proportion of participants with a lifetime diagnosis of alcohol abuse or dependence, according to OPCRIT diagnostic criteria, was 38.7%% of the men and 17.0%% of the women (compared with 9.4%% and 3.7%% respectively for alcohol-use disorder in the past 12 months in the general population according to the National Survey of Mental Health and Wellbeing population-based survey [14]). Similarly, a lifetime diagnosis of drug abuse or dependence was made in 36.3%% of the men and 15.7%% of the women in the sample (compared with 3.1%% and 1.3%% respectively in the general population with a substance-use disorder in the past 12 months [13]). In decreasing order of frequency, the most commonly reported substances were cannabis, amphetamines, LSD, heroin and tranquillisers, with 19.1%% of the participants having used more than one drug. Twelve per cent of the sample had wanted, but felt unable, to stop or cut down their drug use, or had experienced withdrawal symptoms on attempts to do so.
Socioeconomic profile
The life histories of the majority of people with psychotic disorders were marked by long-term educational and economic disadvantage. Thus, 58.1%% had left school at age 16 years or earlier and 47.8%% neither had completed secondary schooling nor had attained any post-school qualification (compared with a proportion of 36.8%% for the Australian population aged 15-64 [15]). However, 11.6%% had achieved a tertiary education diploma or degree and 15.0%% were continuing their education full-time or part-time.
In the month prior to interview, only 14.5%% were living in a home they owned, and another 14.9%% were staying in a home owned by their family. Rented accommodation (public or private) was used by 31.4%%. A high proportion were in a lodge or hospital (19.6%%); hostel or group home (16.4%%); and 11.3%% were in a marginal accommodation such as supported housing (2.6%%), rooming houses, hotel rooms, crisis shelters, or had no fixed address (8.8%%). Individuals who used several forms of accommodation in the month prior to interview are counted more than once.
The great majority (72.0%%) were unemployed (with employment broadly defined to cover formal employment, study and home duties) at the time of the interview and 58.3%% were unable to describe any ‘main occupation’ during the previous 12 months. Of the 273 individuals (27.9%% of the sample) who were in formal employment, only 96 had been working full-time throughout the previous 12 months. Notably, 55 of those in employment had been working at managerial, professional or associate professional levels, and another 39 had been working in trades or in occupations at the advanced clerical and service level.
Social isolation
The majority of the participants, 63.5%% (76.6%% of males and 43.9%% of females) were single and 20.6%% (13.3%% of males and 31.5%% of females) were divorced, separated or widowed. A high proportion (31.3%%) were living alone in single-person households. Although 33.1%% (21.3%% of men and 50.5%% of women) had children, only 8.0%% of the total sample had children under 18 years of age living with them and 6.7%% (2.6%% of men and 12.9%% of women) considered themselves to be the main person responsible for the care of the children. Only 9.3%% had a person at home they could describe as a carer to look after their own needs. The extent of social isolation is further illustrated by the high proportions of respondents who did not participate in ordinary home activities like sharing meals with others (47.1%%); watching television programs with others (40.0%%); playing games (21.0%%); or doing chores or errands for others (39.8%%). Although as many as 87.1%% stated they knew people who they regarded as friends, 39.1%% had no ‘best friend’ with whom they could share thoughts and feelings and 44.9%% felt they needed ‘good friends’. Of the 499 participants (50.9%% of the total) who volunteered responses about their sex lives, 49.9%% had had no sexual relationships over the previous year.
Impairments in daily living
Impairment in self-care was rated as present in 29.8%% of the sample. In 3.6%% of participants, this amounted to marked self-neglect. Impairment in the maintenance of a general interest in the world around (including keeping up with the local and world news, sports, reading and hobbies) was present in 39.6%%, including 9.7%% in whom the loss of interest was pervasive.
Dysfunction in daily household activities (including cooking, cleaning, sharing meals and other tasks or behaviours involving interactions with others) was rated as present in 49.1%% of the participants for whom such activities were relevant (those living with a family or household) or in 25.8%% of the total sample. Dysfunction in socialising outside the home (in contrast to spending time alone) was present in 59.1%% of the total sample.
Performance in a main occupational role (job, housework or studying) could be rated for only 38.2%% of the participants, either because they had not carried out any such role in the previous year or because their work performance could not be assessed in the course of the interview. Of these, 46.2%% had experienced obvious or severe dysfunction. Among the 273 participants (27.9%%) who had any formal employment, 145 had lost 2109 person-weeks off role (14.7%%) out of the total 14352 person-weeks during the year. However, a significant minority had experienced no dysfunction in their main occupational role performance during the year. Thus 89 (32.6%%) of those in employment had not been incapacitated at all and another 41 (15.0%%) had had less than 1 week off role, giving a total of 47.6%% (130 individuals) with little or no incapacitation.
Service utilisation
Contact with treatment services in past year and current medication (%%)
A high proportion (43.9%%) had had at least one contact with an emergency service during the preceding year, including 20.2%% who had attended a general hospital emergency department only; 10.1%% who had contacted a psychiatric emergency team only; and 13.6%% who had made contacts with both hospital emergency departments and psychiatric emergency teams. Of all individuals who had used emergency services, drug overdose, other self-inflicted harm, or alcohol- and drug-related problems were reported by 22.6%%.
During the year preceding the interview, 60.1%% of all participants had attended an outpatient or community mental health service, with 43.1%% of the total sample reporting frequent or regular visits. Of all the participants who had attended a community or other outpatient service, 63.7%% had made visits to a community mental health centre and 25.8%% had made visits to psychiatric outpatient departments in general hospitals. The majority (56.2%%) had a case manager in the community team. The case manager was a nurse in 43.7%% of instances and a social worker in 21.6%%. Less commonly, the case manager was a medical officer (12.9%%) or a psychologist (9.3%%). However, 90.0%% of those attending a community clinic said that the health professional they saw most often was a psychiatrist or other medical officer. A high proportion (81.3%%) had seen a general practitioner at least once during the past year, with a mean number of 12 visits and a median of five. Private psychiatrists were seen at least once during the year by 24.4%%. Only 6.6%% had made visits to private psychologists. The proportion of respondents who had private health insurance was 13.2%%, considerably lower than the national average of 31.9%% for hospital insurance and 31.6%% for ancillary insurance [16].
Types of services received
Respondents were asked whether, on one or more occasions during the year, they had received any of seven specified services. Medication prescription was the service most frequently provided (91.0%%) while help with self-care was the least frequently provided (25.2%%). Psychotherapy, cognitive-behavioural therapy or counselling were identified as a service provided to 39.1%% of the participants. The prescribing of medication was not only the most frequently provided service, it was also felt to be the service that met the needs of a greater proportion of the sample using the service (87.7%%) than any other service. The remaining services were perceived as less than adequate by an almost invariable proportion of about one-quarter of the participants.
Participation in a rehabilitation or a day hospital program during the previous year was reported by a very small percentage (19.1%%). Only 6.3%% of the sample had been involved in rehabilitation programmes for 6–12 months.
The participants were asked about services received in the previous 12 months from 13 types of agencies and organisations. Three government agencies were among the most frequently sought resources: (i) the Commonwealth Department of Social Security (services provided to 68.5%% of the sample, with 87.0%% of those who had received these services feeling that their needs had been adequately met); (ii) state housing services (used by 24.5%%, with 70.8%% being satisfied); and (iii) the Commonwealth Employment Service (sought by 25.4%%, with 57.4%% being satisfied). Other government agencies, including departments of community services, local councils, legal aid, family courts, ethnic services and community counselling had been used by smaller percentages of the respondents with lower levels of satisfaction. Notably, assistance provided by the churches or by various non-governmental agencies and self-help organisations had been widely used, with high percentages of the users reporting that their needs had been adequately met.
Pharmacological treatment
The great majority (86.2%%) stated that, in the previous month, they had been taking prescribed medication for 1 month or more and were able to identify the drugs from a table listing both the generic and trade names (the interview did not aim to ascertain actual adherence). ‘Typical’ antipsychotic agents were being used by 54.4%%; this included the 25.6%% of the participants who were receiving depot preparations. The share of the ‘atypical’ antipsychotics was 30.8%%. Use of any mood stabilisers (lithium, carbamazepine or sodium valproate) was reported by 24.3%%. The percentage reporting the use of any antidepressants was 26.4%%; the majority (19.3%% of the total) had been prescribed selective serotonin reuptake inhibitors (SSRIs) or reversible inhibitors of the monoaminoxi-dase (RIMA) class.
The majority (83.4%%) felt that their psychotic symptoms responded to medication. However, 63.2%% described themselves as impaired in their daily life due to side effects of treatment. Dryness of mouth or hypersalivation (48.2%%), drowsiness (47.7%%), restlessness (36.0%%), tremor (34.9%%) and inability to relax (31.9%%) were the most common complaints. Symptoms of tardive dyskinesia were reported by 12.7%%.
Aspects of quality of life
Quality of life items were incorporated in the interview, including impairment in daily life; disablement in social or occupational roles; aversive mood states or cognitions; and objective adversity associated with social isolation, marginalisation and socioeconomic deprivation (such as feeling unsafe in the residential locality, being a victim of violence, occurrence of self-harming behaviour, arrests and being charged with an offence). Overall, 15.3%% described feeling unsafe in their present neighbourhood or locality, and 17.6%% reported having been a victim of violence in the last 12 months. Of the 172 respondents reporting such incidents, 62.2%% had been physically assaulted (including 7.0%% sexually assaulted). The remaining 37.8%% referred to robbery incidents (4.7%% of the total) or did not provide specific details of the offence. Instances of self-inflicted harm or overdose during the previous 12 months were reported by 16.5%% (4.8%% had three or more such episodes). A total of 10.2%% of the sample reported having been arrested at least once in the past year (2.9%% had more than one arrest). In the respondents' own description, the charges were for non-violent offences in 33.0%% of the instances and for violent offences in 10.0%% of the instances. Insufficient detail was provided at interview on 57.0%% of the reported instances.
Impairments, disabilities and lifestyle variables by sex
Perception of unmet need
In the 12 months prior to interview, 47.0%% of the sample had experienced a need for a particular kind of service but had been unable to access it. They were asked in an open-ended question to specify the nature of the service and to note if availability and/or afford-ability were the reasons that their need for the service was unmet. For 251 of the 425 respondents who named a specific kind of service, the main concern related to access to treatment, continuity of care and the need for information. Of those experiencing an unmet need for services, 65.5%% referred to at least one service that was not available, and 49.5%% mentioned at least one service that was available but not affordable.
People with psychoses who are marginalised or homeless and not identified in other service settings
In comparison with the ‘mainstream’ service users, the marginalised group with psychotic disorders had several distinctive demographic characteristics: (i) a larger proportion of males (72.5%% compared with 60.8%% in the ‘mainstream’ group); (ii) a larger proportion of single persons (71.7%% compared with 63.3%%); (iii) a higher percentage lacking school or post-school qualifications (58.3%% compared with 47.9%%); and (iv) a lower percentage who had had any history of employment in the previous 12 months (10.0%% compared with 17.0%%). No major differences were apparent between the two groups with regard to lifetime or current psychopathology, but the marginalised group tended to have more prominent thought and speech disorders, passivity experiences and subjective thought disorder. The percentage currently experiencing such symptoms was 40.8%% among the homeless or marginalised people compared with 34.5%% among the ‘mainstream’ treatment service users. Chronic, unremitting illness with deterioration was more common among the marginalised group (54.2%%) than among the ‘mainstream’ group (41.2%%). On several measures the homeless or marginalised people with psychotic disorders appeared to be more severely ill. The high prevalence of alcohol and other substance abuse (45.8%% with alcohol abuse and 21.7%% with other substance abuse, compared with 29.0%% and 13.2%%, respectively, in the ‘mainstream’ group) is likely to be a major contributing factor in the severity and chronicity of psychotic symptoms in this group.
Consistent with the overall way of life, the rate of utilisation of both inpatient and outpatient mental health services by the homeless was much lower than that by the patients recruited through the census of the ‘mainstream’ services. Thus, only 27.5%% had been admitted as inpatients during the previous year (compared with 62.9%% of the ‘mainstream’ group), and only 35.8%% had received any outpatient mental health care (compared with 75.3%% of the ‘mainstream’ group). However, a higher percentage of the homeless (50.8%% compared with 47.6%% of the ‘mainstream’ group) had used hospital emergency services, and also a higher percentage (85.8%% compared with 76.7%% of the ‘mainstream’ group) had seen a general practitioner at least once during the previous year.
People with psychoses attending general practitioners or private psychiatrists
The group of patients who had been under the sole, or predominant, care of a general practitioner was in many respects different to the ‘mainstream’ users. Thus, the group included a high proportion (53.2%%) of females and individuals who had been married (41.6%%), many of whom had children living with them. A high proportion (60.1%%) had a school or post-school qualification and a relatively high proportion (30.6%%) had been working during the preceding 12 months. There were no major differences between the patients in this subsample and the ‘mainstream’ patient sample with regard to the lifetime occurrence of psychotic symptoms and the pattern of course. However, the patients under the care of general practitioners or private psychiatrists tended to have less severe current symptoms, as shown by the lower percentages exhibiting hallucinations and delusions, subjective thought disorder, blunted affect, poverty of speech and lack of insight.
Compared with the mainstream patient sample, the group identified through general practitioners and private psychiatrists tended to have less dysfunction in social roles and in daily functioning, and were less likely to have a history of psychoactive substance use, attempted suicide or self-harm, or to have been a victim of violence. Similarly to the homeless group, but for different reasons, this group made considerably less use of both inpatient and outpatient services than the ‘mainstream’ patients with psychoses. In contrast to both the ‘mainstream’ patients and the homeless people with psychoses, the patients under the care of general practitioners or private psychiatrists also made less use of other governmental and non-governmental welfare organisations.
People with psychoses not in current service contact
The census of people with psychotic disorders based on current service contact was likely to miss individuals who rarely use services or who have dropped out of service contact. It was therefore important to establish whether such low-intensity service users: (i) represent a subgroup that has drifted away from service provision; (ii) are mainly individuals who have reduced their contacts with services because of a relatively good outcome and recovery; (iii) are actually receiving care from sources other than the mainstream public services. To answer these questions, an additional sample of 801 individuals with psychotic disorders was identified by searching the registries of the hospitals and clinics. A total of 146 were interviewed with the DIP. Of these, 98 had been in contact with the services within 11 months of the census and 48 had been in contact 1–3 years prior to the census, but none had had a recorded contact in the census month. Because of the difficulty in tracing individuals in this subsample, the set of persons interviewed may not be representative of the entire out-of-contact sample. This limitation being considered, the 146 low-intensity service users were compared with a subset of the census month sample that included those 687 individuals (out of the total 980) who had been receiving care from the same mainstream services. Three important findings emerged from this comparison that will require further replication. First, the two groups did not differ significantly from one another in terms of lifetime symptom profiles (except for the lower frequency of hypomanic symptoms in the out-of-contact group). However, they differed markedly with regard to present state (last month) symptoms, with generally lower levels of symptomatology in the out-of-contact sample compared with the mainstream service users. Second, a pattern of course characterised by a single episode of psychotic illness followed by good recovery was twice as common, while chronic course with severe deterioration was three times less common in the out-of-contact group. Third, significantly fewer people in the out-of-contact group had a history of alcohol, cannabis or other substance abuse and lower percentages had attempted suicide or other self-harm, had been arrested, or had been victims of violence during the previous year. It appears, therefore, that the out-of-contact sample included mainly people with better clinical and psychosocial outcomes. Further study of the characteristics of this group might highlight factors and predictors associated with better outcomes of psychotic disorders.
Discussion
Main conclusions from the study
To place these findings in a broader perspective, comparisons with similar studies conducted elsewhere would be of interest, with the proviso that any such comparisons must take into account differences in study design and methodology, as well as differences related to the background characteristics of populations, the health care context and the point in time of data collection. As regards the point prevalence of psychotic disorders, the findings of this study, a weighted mean of 4.7 per 1000 for 1-month prevalence, fall within the range of prevalence rates for schizophrenia and related disorders reported by the majority of European and North American studies (reviewed in [17],[18],[19]). Adjusting this rate downward to exclude affective disorders with psychotic features (19.5%% of the interviewed sample, according to ICD-10 criteria), will result in an estimated rate of 3.7 per 1000 for schizophrenia and other non-affective psychoses in the present study. This rate is very close to the median point prevalence rate of 3.2 per 1000, estimated by Eaton et al. [19] on the basis of a comprehensive review of some 25 prevalence studies of schizophrenia. Thus, the findings of the present study lend further support to the notion that the rates of manifestation of the schizophrenic syndrome are strikingly similar in populations of comparable demographic characteristics. In the light of this central tendency, which has been amply documented by numerous investigations around the world, the variation of rates across the four sites of this study (range 2.8–5.1 per 1000, all psychoses) appears to be relatively minor. Such variation is entirely compatible with the sociodemographic differences between the selected urban areas, with higher rates as might be expected in predominantly inner-city areas (Perth and Melbourne) compared with areas containing suburban and semi-rural tracts (Canberra and Brisbane). This is well in accord with findings from research into the urban ecology of schizophrenia [20],[21] which has highlighted the tendency (‘urban drift’) for persons with psychotic disorders or prepsychotic features to concentrate in inner-city areas providing greater anonymity, cheap accommodation and access to a variety of formal and informal helping agencies.
However, establishing the prevalence rate of psychoses in urban areas is not in itself sufficient for an understanding of the true extent of disability-impaired quality of life, and need for services associated with such disorders. Moreover, whereas the prevalence of psychotic syndromes appears to be relatively stable across populations and over time, there is good evidence [2] that the impact of psychotic illness on social adjustment and daily living varies greatly as a function of culture, economic factors, social attitudes and systems of support and care. In this regard, the present study has definite advantages over many previous epidemiological investigations, as a broad range of relevant variables were explored in depth. Among the limited number of studies that provide useful reference points for comparison, three British studies stand closer to the present one in terms of population characteristics, setting and service provision context. A follow-up study of a cohort of 532 patients with schizophrenia discharged from hospital between 1975 and 1985 [22] found a pattern of symptomatology and social impairments similar to the one described in the present study. Comparable findings have also been reported on a community sample of 350 people with psychosis interviewed in the context of the Office of Population Censuses and Surveys study of psychiatric morbidity in Great Britain [23]. Better comparability, however, is provided by the surveys conducted in the inner London borough of Camden in 1986–87 [24] and in 1991 [3]. In this study, a point prevalence of 5.3 per 1000 was estimated from a census for a ‘broad’ definition of schizophrenia and 528 patients were assessed in 1986–87 using a psychopathology scale, a social behaviour schedule and a questionnaire on activities of daily living and service use. In many respects, this sample was closely similar to the sample interviewed in the present study. Almost identical proportions were living in the community (83.0%% in Camden, 80.4%% in this study), in single-person households (30.0%% and 31.3%%) or hostels (22.0%% and 27.8%%). The majority had never married (63.0%% and 63.5%%) or were divorced/separated (23.0%% and 20.6%%). The mean lengths of illness were 17.0 years (Camden) and 15.1 years (this study) and similar proportions were experiencing psychotic symptoms, depression and suicidal ideation. In both settings the unemployment rate among patients was extremely high (81.0%% in Camden, 72.0%% in this study) and the majority had no meaningful daytime occupation. Compared with the Camden sample, however, the Australian patients had a higher utilisation rate of specialist services (as an example, 90.0%% of the participants in this study had seen a psychiatrist in the last year compared to 39.0%% in Camden; 25.0%% of the Camden cases had had no contact with the specialist services and were receiving care from general practitioners only). It should be noted that the repeat survey in the same London area in 1991 [3] established a significant trend towards increased specialist supervision and closer links between primary care and the specialist services. It appears, therefore, that the patterns of service provision to people with psychotic disorders in the two settings are on converging paths. There is little evidence from either study, however, that high or increasing specialist coverage alone has any impact on the aggregate burden of social disability among people with psychotic disorders in the community. The social burden is likely to be more strongly determined by factors operating at the social system level, such as the exclusion of the mentally ill from the employment market and their marginalisation in the community, rather than at the clinical and service provision level. While the complexity of the problem of psychotic illness and its attendant burden of high social and economic cost [25] can hardly be overstated, an understanding of the problem should spur to action rather than lead to acceptance of the status quo.
CONCLUSION
The general conclusion of this study is that the socalled ‘low-prevalence’ psychotic disorders represent a major public health problem in Australia today affecting at any time between three and five out of every 1000 adults. In Australia, as well as elsewhere, these disorders are associated with a heavy burden of disease and disability and with great personal distress. The majority of the people with persisting psychotic disorders now live in the community, but only a minority attain a level of functioning and well-being that is commensurate with good quality of life. Many of the services available to them tend to be provided on a crisis-response basis. The need for therapeutic, housing, rehabilitative and support measures that are likely to have an impact on the course of their disorders and their social adjustment remains largely unmet. There is at present international consensus [26] that, even in the absence of primary prevention and radical cure, much of the disability and distress associated with the psychotic disorders can be prevented or reduced if the effective interventions and management strategies that exist today are widely available and applied consistently and systematically over the various stages of the illness. This calls for a broad programmatic approach on a national basis. Such an approach must be complex, balanced, and mindful of the fact that, in order to tackle the multiple dimensions of clinical disorders, personal functioning and socioeconomic environment, concerted action across many sectors of the society is required.
The full report of the study [6] is available for downloading in PDF format at the following address: http://www.health.gov.au/hsdd/mentalhe/pubs/index.htm. It may also be ordered through Mental Health Branch, MDP 37, Commonwealth Department of Health and Aged Care, GPO Box 9848, Canberra, Australian Capital Territory 2601, Australia.
Footnotes
Acknowledgements
The present report is based on data collected in the framework of the Collaborative Study on Low-prevalence (Psychotic) Disorders, an epidemiological and clinical investigation which is part of the National Survey of Mental Health and Wellbeing, Australia 1997–98. The members of the Low-prevalence Disorders Study Group are: Assen Jablensky, Project Director and Team Leader, Western Australia; Vaughan Carr, Adviser; David Castle, Deputy Team Leader, Western Australia; Mandy Evans, Team Leader, Australian Capital Territory; Oye Gureje, Deputy Team Leader, Victoria; Carol Harvey, Deputy Team Leader, Victoria; Helen Herrman, Team Leader, Victoria; Ailsa Korten, Statistician; John McGrath, Team Leader, Queensland; Vera Morgan, Project Database Manager. Other investigators at the four sites included: Scott Henderson, Stephen Rosenman, Jo Medway (Australian Capital Territory); David Chant, Susette Cardy, Chris Young, Ben Chapple (Queensland); Ian Gordon, Tom Trauer, Helen Evert, Tony Pinzone (Victoria); Anna Waterreus (Western Australia). A complete list of the investigators is available in Jablensky et al. [![]() ]. The study was funded by the Commonwealth Department of Health and Aged Care (Brisbane, Melbourne and Perth), by local sources (Canberra), and by the Diagnostic Assessment Consortium of the NH&MRC Network for Brain Research in the Major Mental Disorders. This report also acknowledges, with thanks, the mental health professionals who assisted in the preparation and conduct of the survey and the many Australians with psychotic disorders who agreed to participate. Without them, this study would not have seen the light of the day.
]. The study was funded by the Commonwealth Department of Health and Aged Care (Brisbane, Melbourne and Perth), by local sources (Canberra), and by the Diagnostic Assessment Consortium of the NH&MRC Network for Brain Research in the Major Mental Disorders. This report also acknowledges, with thanks, the mental health professionals who assisted in the preparation and conduct of the survey and the many Australians with psychotic disorders who agreed to participate. Without them, this study would not have seen the light of the day.