
Abstract
Objective:
Clinical studies consistently identify alcohol- and drug-related treatment populations as more likely to die prematurely compared with an age-matched general population. However, demographic characteristics and primary drug of concern as predictors of mortality risk following treatment have not been adequately explored. This paper examines relationships between substance use, demographic factors and mortality among alcohol and drug treatment clients.
Method:
A retrospective cohort incorporating 7 years of data was utilised to examine mortality outcomes in the 2 years following treatment among Victorian clients recorded on the Alcohol and Drug Information Service (ADIS) database by linking partial client identifiers with the National Death Index (NDI). A cohort of 18,686 clients engaged in at least one course of treatment over a 12-month period was included. Analysis was of crude and standardised mortality rates across client groups in terms of the presenting drug of concern for treatment and demographic characteristics.
Results:
A higher risk of premature death was associated with older age, being male, not being employed, living alone, medical and psychiatric comorbidity, recent injecting, and a history of intensive drug treatment access. Alcohol treatment clients had the worst prognosis. After adjustment for client characteristics, alcohol treatment clients experienced a significantly higher rate of death compared with other clients.
Conclusions:
Findings from these previously unexplored data highlight the need to increase awareness of the range and magnitude of risks associated with harmful alcohol use, and to identify approaches to enhance treatment effectiveness to reduce negative outcomes following treatment for populations at elevated risk of harm.
Introduction
People with alcohol- and other drug (AOD)-related problems in treatment are more likely to die prematurely when compared with age-matched peers in the general population (Gossop et al., 2002; Oppenheimer et al., 1994; Warner-Smith et al., 2001). Demographic factors that elevate the risk of death among alcohol and drug users identified previously include physical characteristics such as male gender (Bell et al., 2009; Bird et al., 2003; Clausen et al., 2008; Degenhardt et al., 2009; Hickman et al., 2003; Ravndal and Amundsen, 2010) and older age (Bell et al., 2009; Bird et al., 2003; Degenhardt et al., 2009; Hickman et al., 2003; Lewis et al., 1995; Moos et al., 1994), physical co-morbidities such as chronic medical conditions (McCowan et al., 2009; Moos et al., 1994; Saitz et al., 2007), psychiatric comorbidity (Gossop et al., 2002; McCowan et al., 2009; Saitz et al., 2007), homelessness (Gossop et al., 2002; Langendam et al., 2001; Saitz et al., 2007) and low social support (Lewis et al., 1995; Moos et al., 1994). Drug use characteristics have also been identified as risk factors for elevated risk of death, and include injecting drug use (Bird, 2010; Hickman et al., 2003; Langendam et al., 2001; Quan et al., 2007), polydrug use (Gossop et al., 2002) and alcohol or heroin as substance of choice compared with cocaine (Saitz et al., 2007). Thus, both direct risks associated with the physiological effects of specific drugs (such as central nervous system (CNS) depressants like alcohol and heroin) and cumulative impacts of alcohol and drug use on health and related social factors contribute significantly to the risk of death among drug users.
Recent research examining mortality outcomes for people with a drug use history indicates that treatment engagement is protective against premature mortality within certain treatment modalities (Darke et al., 2011; Degenhardt et al., 2009). Mortality rates among opioid pharmacotherapy clients were typically lower in treatment than after leaving treatment. For instance, Degenhardt et al. (2009) found that opioid pharmacotherapy clients had an in-treatment crude mortality rate of 6.0 (95% confidence interval (CI): 5.7–6.4) per 1000 person-years compared with an out-of-treatment rate of 11.5 (95% CI: 11.1–12.0) per 1000 person-years. There is evidence indicating that there are certain vulnerable time periods both during and after treatment where risk of death may be elevated for treatment populations. The first 4 weeks after commencing treatment and the first 4 weeks post-treatment witness clients at an increased risk of drug-related mortality among some populations, with elevated mortality risk among opioid pharmacotherapy clients in the first 2–4 weeks after ceasing treatment (Clausen et al., 2008; Degenhardt et al., 2009). The first 1–4 weeks of induction into treatment is also a time of elevated risk (Buster et al., 2002; Degenhardt et al., 2009). While Saitz et al. (2007) reported mortality following treatment across a number of drugs of concern, and found that alcohol predicted a higher risk of death following detoxification when compared with cocaine, this study was only able to report on one treatment modality – detoxification. Less is known about longer-term mortality outcomes following treatment that does not involve opioid pharmacotherapy or for clients who have sought AOD treatment, and this represents a substantial gap in the literature that has resulted in the absence of an evidence base to support policy responses and clinical planning. Given the high proportions of clients seeking treatment for alcohol use or other non-opioid substances from specialist alcohol and drug agencies (Australian Institute of Health and Welfare (AIHW), 2011), there is a need to examine longer-term outcomes following AOD treatment cessation as a potential period of increased risk due to disengagement from care and clinical management across different presenting drugs of concern.
Effective management of AOD use disorders is a fundamental issue for clinicians, including the role of correlates and comorbidities (e.g. Sara et al., 2012; Schroder et al., 2008; Teeson et al., 2012), with a focus on outcomes and recovery following dependence of central importance (Best and Lubman, 2012).
Despite numerous studies demonstrating lower mortality outcomes for those engaged in drug treatment, the role of demographic characteristics and primary drug of concern as predictors of longer-term mortality risk in the 2 years following cessation of treatment engagement has not been adequately explored. This paper helps address this gap by examining the relationship between substance use characteristics and demographic factors and mortality outcomes using a population level cohort of AOD treatment clients across a range of treatment modalities outside of general practice-based pharmacotherapy in Victoria, Australia to provide evidence to support targeted clinical service delivery and post-treatment follow-up.
Method
Retrospective cohort data were utilised to examine mortality outcomes among Victorian clients. Client data were drawn from the Alcohol and Drug Information Service (ADIS) database (including detailed information regarding all specialist treatment occurring in Victoria) and this was linked to the National Death Index (NDI; which includes all detailed information regarding cause of death for all deaths occurring in Australia). Linkage between the two databases was established by linking partial client identifiers between the two databases.
Cohort
The ADIS database is a register of government-funded, specialist AOD treatment services. Members of the cohort for analysis had to have completed at least one course of AOD treatment (e.g. counselling, residential withdrawal) in the 12-month period between 1 July 2000 and 30 June 2001, with their first course of treatment (COT) starting on or after 1 January 2000. Records were only included in the cohort if they had a valid date of birth and start date of their first COT. Based on these criteria our cohort consisted of 18,686 clients. To construct a unique identifier we used a unique combination of partial name identifiers (second two letters of first name and first two letters and last letter of surname), date of birth and gender (e.g. John Doe, 17/01/1969, male, would be ‘ohdoe170169m’). These codes were used to identify cohort individuals and link their information across ADIS and NDI.
Data sources
ADIS
Cohort codes were matched across 8 years of data from ADIS, including COTs that terminated between 1 July 2000 and 30 June 2008. Multiple COTs were common among the cohort, with a median of 2 (interquartile range (IQR) 1–5) COTs. COTs could be continuous, indicating a change of treatment type, agency or drug of concern. Multiple COTs could be sequential, overlapping or embedded within other COTs (e.g. a short episode of outreach could occur within a 6-month-long course of counselling).
All categories of drugs of concern as reported in ADIS were reported, including COTs where tobacco was recorded as the primary drug of concern. It is important to note that in cases where tobacco is recorded as the primary drug of concern, clients also have other drugs of concern, as the specialist AOD service system in Victoria does not provide treatment for nicotine dependence unless this is an adjunct to treatment for other drugs of concern. To provide data to support the capacity for clinicians and services to identify clients potentially at elevated risk of harm, it was necessary to present data that reflected all client populations accessing specialist AOD treatment services in terms of reported drugs of concern.
COTs were excluded if they started before 1 January 2000 or after 1 January 2007. The total number of COTs provided to the cohort was 89,764. A series of data extraction algorithms were applied to clean and prepare the data to ensure that the data accurately reflected the nature of treatment engagement for consecutive and concurrent COTs, including amendment of overlapping COTs and recoding multiple consecutive COTs. After cleaning, approximately 15% of records were removed; the total number of COTs provided was 76,342.
National Death Index (NDI)
The cohort codes extracted from ADIS were submitted to the AIHW for data matching with the NDI. AIHW ran three linkage passes. The first involved using an exact match unique identifier. The second pass was the same as the first except matched on only month and year of birth. The third involved cases where the client had been recorded validly as deceased within ADIS. Where a match occurred, death had to have occurred after the date of last contact in ADIS.
Almost all (532; 94%) deaths were linked using the exact method with NDI. A further 10 clients (2%) were linked to NDI records using the second pass method and the remaining 23 (4%) deaths were linked using the third pass method.
Analysis
Data were examined using survival analysis, and conducted using Stata 11 (StataCorp LP, College Station, TX, USA).
Predictor variables
Demographic, drug and treatment variables available in ADIS were included as predictors in survival time analysis. Static demographic variables included sex, country of birth (born in Australia or not) and indigenous status. All other demographic variables were time-varying covariates and included age, employment status (employed or not employed), living status (alone or with family/others), temporary or homeless accommodation status, and current involvement in the justice system (through community-based orders, parole, bail, custody, etc). Primary drug of concern and injecting drug use were measured at the start of each COT. Medical and psychiatric comorbidities were also included as covariates. Treatment-related variables included type of treatment received, number of COTs per client and reason for treatment termination.
As a proxy measure of polydrug use, individuals who had received multiple COTs with different primary drugs of concern were classified as polydrug users. While this provides a conservative measure of polydrug use, it has utility in identifying clients with multiple drugs of concern requiring treatment.
Crude mortality rates and standardised mortality ratios
To calculate crude mortality rates (CMRs) and standardised mortality ratios (SMRs), time at risk (in person-years) was calculated from date of first contact with ADIS (between 1 January 2000 and 30 June 2001) to either date of death or, for right-censored cases, the earliest of 2 years after the last COT ended or 31 December 2006. The last COT was used for calculation of mortality risk, as the purpose of these analyses was to examine mortality following cessation of treatment engagement – using data related to other COTs would not enable such exploration as multiple courses of treatment were a common feature of patterns of treatment utilisation among clients in this cohort (as described above).
All-cause CMRs were calculated by dividing the total number of deaths by the equivalent sum of person-years of observation. CMRs are presented per 1000 person-years (PY). Indirect all-cause SMRs were calculated by 10-year age groups based on death rates of the Victorian population in the year 2000. Two-sided 95% confidence intervals (95% CI) were based on Poisson distribution.
Factors predicting mortality after treatment discharge
As some cohort members either died during treatment or were in treatment at the end of the observation period, the number in the cohort used to predict mortality after treatment discharge was reduced from 18,686 to 17,861 (825 observations deleted), which reduced the number of deaths from 570 to 423 – the decrease reflecting the high risk of death during early stages of treatment. Time at risk was calculated from the date of termination of last COT to death or censorship. Censorship occurred at the earliest of 2 years after the last COT ended or 31 December 2006. The median survival time was 2 years.
Cox proportional hazards models were run to assess bivariate relationships between indicator variables and time to death. Variables that did not meet the proportional hazards assumption (Hosmer and Lemeshow, 1999) in bivariate models were interacted with time (defined as the first and second years of follow-up) by entering two ‘heaviside’ functions into models. When heaviside functions are used, fixed hazard ratios for specified time intervals are generated (Kleinbaum and Klein, 2005). Proportional hazards assumptions were tested again with these time-interacted variables and all models were well-specified.
Only covariates with p-values < 0.05 in univariate models were included as controls in the multivariate Cox proportional hazards models. These models controlled for age, sex, not being employed, living alone, medical comorbidity, psychiatric comorbidity, recent injecting and total number of COTs received. Unadjusted and adjusted models were run separately for each drug of concern, with the reference group defined as all other cases.
Results
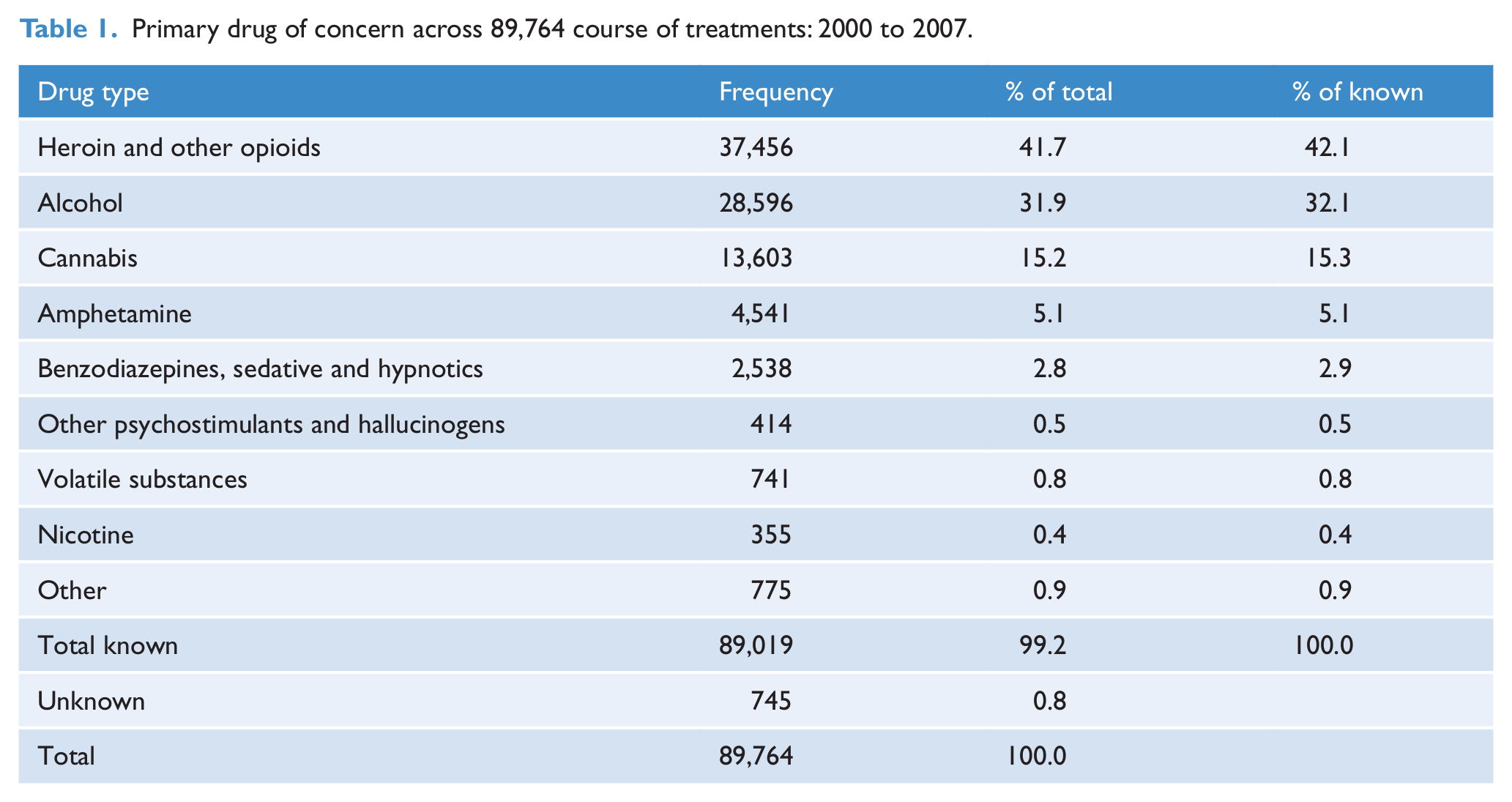
Treatment data of 18,686 individuals was available for analysis. This represents 69,270 PY over 89,764 COTs. Two-thirds (65%) of the cohort were male and the median age on commencement of treatment was 28 years (IQR 21–36). Heroin and other opioids and alcohol were the most commonly reported primary drugs of concern on entry into a COT within the cohort. Heroin and other opioids accounted for 42% of COTs with a known drug of concern, and alcohol accounted for a further third (Table 1).
Primary drug of concern across 89,764 course of treatments: 2000 to 2007.
Overall, the cohort was followed up for a median of 2.8 years (IQR 2.1–5.7) or a total of 69,270 PY. In that period there were 570 deaths, giving an overall CMR of 8.2 deaths per 1000 PY (95% CI: 7.6–8.9; Table 2). The mortality rate among this cohort was 6.8 times the SMR of the age-matched Victorian population (95% CI: 6.3–7.4). CMRs were significantly higher among males, although SMRs did not significantly differ (Table 2). CMRs increased with age, in contrast to SMRs which decreased with age. For all ages, higher mortality rates were noted for treatment clients compared with the age-matched Victorian population.
Crude mortality rates and standardised mortality ratios by sex, age group and primary drug of concern (n = 18,686).
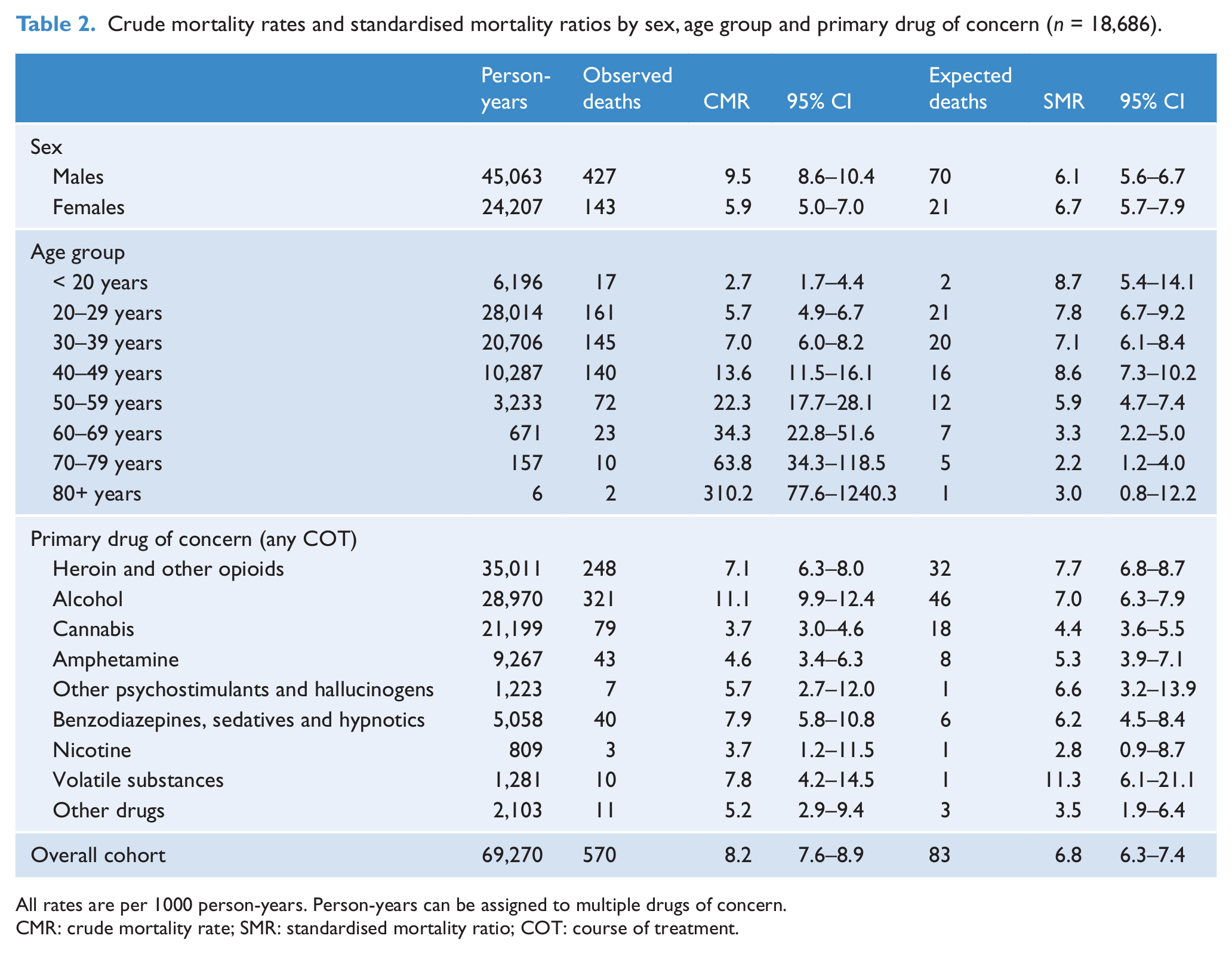
All rates are per 1000 person-years. Person-years can be assigned to multiple drugs of concern.
CMR: crude mortality rate; SMR: standardised mortality ratio; COT: course of treatment.
Mortality associated with specific drug types was calculated by summing the person-years and number of deaths related to any client coded with that primary drug of concern (Table 2). Among clients with cannabis as a primary drug of concern, the SMR was 4.4 (95% CI: 3.6–5.5) times higher than the age-matched Victorian population. The CMR for alcohol (11.1; 95% CI: 9.9–12.4) was significantly higher than heroin and other opioids (7.1; 95% CI: 6.3–8.0); however, SMRs were not significantly different for alcohol and heroin and other opioids (7.0 vs 7.7). The highest SMR was associated with volatile substances – among clients with volatile substances as a primary drug of concern the SMR was 11.3 (95% CI: 6.1–21.1) times higher than the age-matched Victorian population.
Client characteristics and risk of death
Of the 18,686 unique clients available for analysis, 678 clients were in treatment at the end of the study period (December 2006) and 147 clients died whilst in treatment. Data from these clients are not included in further analysis. Table 3 explores the characteristics of 17,861 clients representing 423 deaths. Characteristics associated with a significantly increased risk of death after adjustment for the presence of other factors included older age, being male, not being employed, living alone, medical comorbidity, psychiatric comorbidity, recent injecting drug use and a history of intensive drug treatment service access (multiple COTs). Recent injecting drug use on entry into treatment significantly increased the hazard of death by 55 per cent (95% CI: 13–111%) in the first year of follow-up, but not in the second year.
Client characteristics and associated risk of death (n = 17,861).
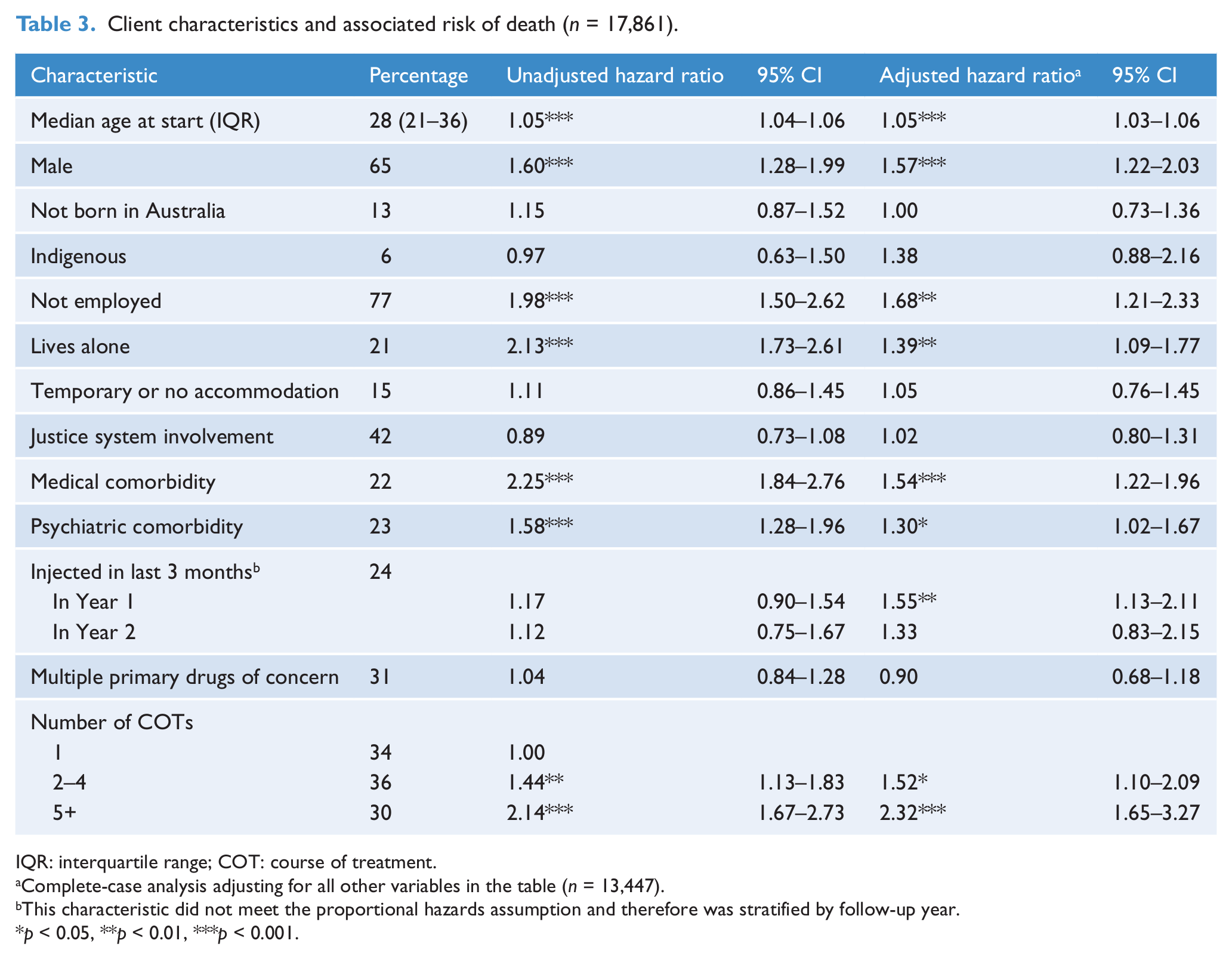
IQR: interquartile range; COT: course of treatment.
Complete-case analysis adjusting for all other variables in the table (n = 13,447).
This characteristic did not meet the proportional hazards assumption and therefore was stratified by follow-up year.
p < 0.05, **p < 0.01, ***p < 0.001.
Drug of concern and risk of death in the first and second year following treatment
After adjustment for covariates, cohort members whose last COT was for alcohol experienced a significantly higher rate of death compared with all others in the cohort: the hazard of death increased by 62% (95% CI: 20–118%) in the first year of follow-up and 123% (95% CI: 41–251%) in the second year of follow-up (Table 4). Figure 1 provides a representation of how survival rates changed over the 2 years following treatment cessation, and reflects the higher rate of death for cohort members whose last COT was for alcohol, as shown in Table 4. Cohort members whose last COT was for cannabis experienced a significantly lower rate of death: the hazard decreased by 57% (95% CI: 34–72%) across the follow-up period. The risk of death for clients whose last COT was for benzodiazepines, sedatives or hypnotics increased by 69% in the first year of follow-up compared with the rest of the sample; however, this was not statistically significant. No deaths attributable to benzodiazepines, sedatives or hypnotics during the second year of follow-up were indicated.
Most recent drug of concern and associated risk of death (n = 17,682).
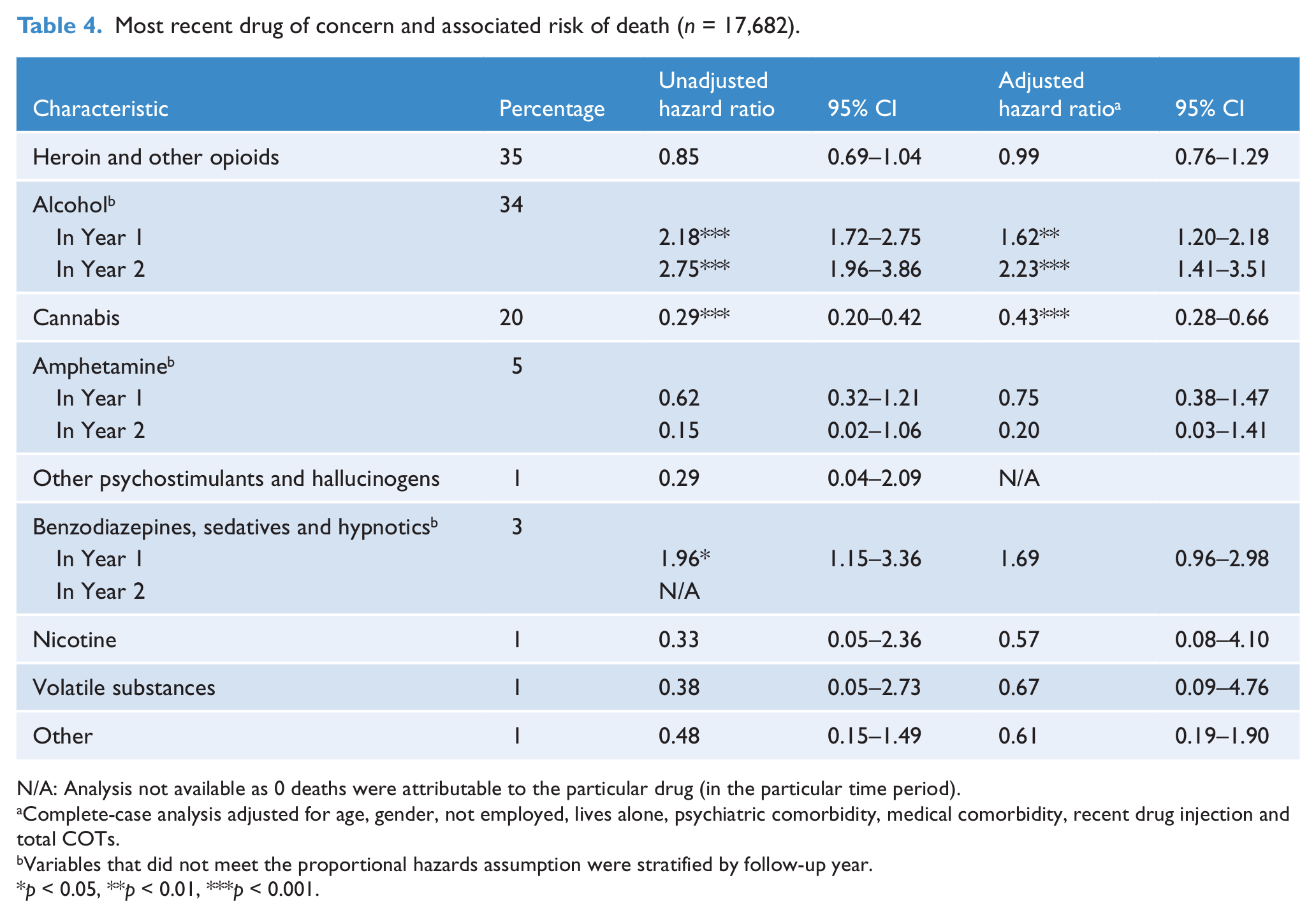
N/A: Analysis not available as 0 deaths were attributable to the particular drug (in the particular time period).
Complete-case analysis adjusted for age, gender, not employed, lives alone, psychiatric comorbidity, medical comorbidity, recent drug injection and total COTs.
Variables that did not meet the proportional hazards assumption were stratified by follow-up year.
p < 0.05, **p < 0.01, ***p < 0.001.
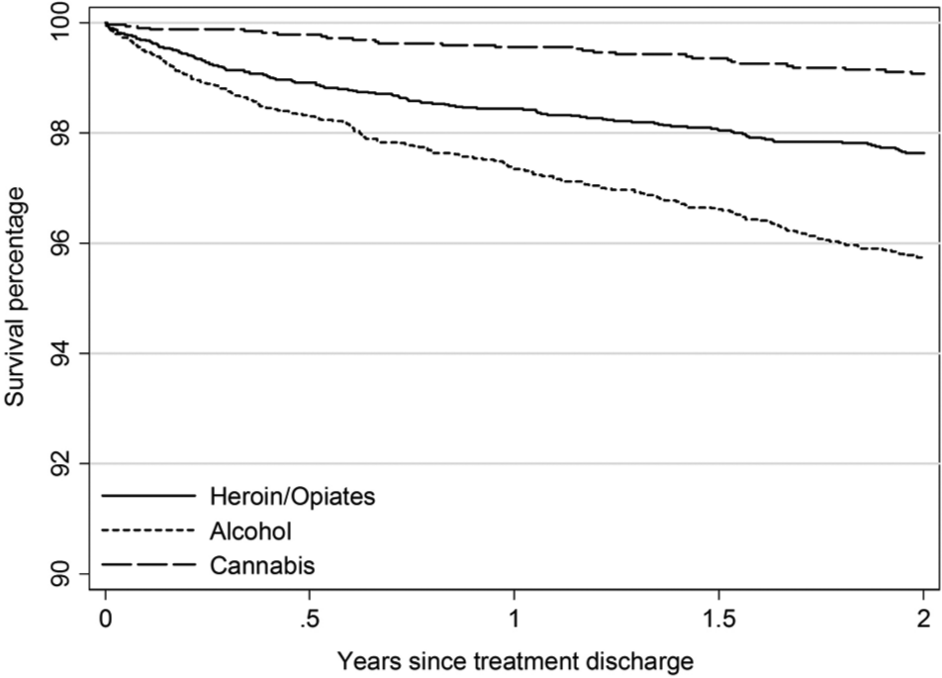
Kaplan-Meier estimates by selected drugs of concern: heroin and other opiates, alcohol and cannabis.
Discussion
This paper reports CMRs for a cohort of Victorian clients who sought and engaged in specialist treatment for a wide range of drug types. Our all-cause CMR for opioid users of 7.1 (6.3–8.0) per 1000 PY was lower than the rate measured in the largest study of Australian opioid treatment clients in pharmacotherapy, who died at a rate of 8.9 (8.6–9.2) per 1000 PY (Degenhardt et al., 2009). In Victoria, most opioid pharmacotherapy treatment is provided by general practitioners, and is not captured in the data presented here. The lower mortality rate among the opioid users in the present study may be due to the cohort being drawn from treatment populations outside of the primary pharmacotherapy system and engaged in other forms of treatment, or a combination of pharmacotherapy and other treatment modalities. This may in turn mean that this study’s findings reflect a cohort experiencing less negative health consequences impacting upon mortality compared with other studies that have cohorts of pharmacotherapy clients, and also differences in treatment system designs (Clausen et al., 2008; Degenhardt et al., 2009; Gibson et al., 2008; Gossop et al., 2002). This distinct population of clients represents a cohort likely to be fundamentally different from opioid pharmacotherapy clients in terms of drug use, consistent treatment engagement, broader service engagement and other characteristics.
While there are no current studies that are directly comparable with the findings presented here in terms of drugs of concern, matching procedure or treatment delivery, international data provides some context for interpretation of these results. The mortality rate from the largest study of drug users accessing treatment in Europe (Bird, 2010) found 8.2 drug-related deaths per 1000 PY of follow-up. While this rate was the same as the overall rate found in the current study, our overall rate included all causes of mortality, not just drug-related. On this evidence, our estimates are likely to indicate a lower rate of premature death in the Victorian cohort compared with the European cohort, and with all other international cohorts reviewed in the introduction. These rates do largely accord with comparable Australian rates where available. One of the contributing factors for lower mortality rates in this cohort than those reported in a number of international studies is likely to be the low rates of HIV infection among illicit drug users in Australia (Guy et al., 2007), while the selection of a sample of clients not primarily engaged in pharmacotherapy treatment is another factor that will have influenced mortality rates. These findings provide interesting insights regarding outcomes following treatment that can inform clinical service delivery, and it is hoped that future studies will enable further examination of our results with more comparable Australian and international populations. Exploration in differences in cause of death may also yield findings that could reflect population differences in risk and harm.
As predicted by previous research, higher risk of premature death among this cohort was associated with older age, being male, not being employed, living alone, medical and psychiatric comorbidity and recent injecting. Having a history of intensive drug treatment service access (multiple COTs) – which is likely to reflect a greater severity of complexity of substance use and related issues – also significantly increased the risk of premature death. In contrast to previous findings, being homeless (defined in these data as not having access to safe, secure and adequate housing) was not associated with significantly increased mortality risk.
Most significantly, clients discharged from alcohol treatment had the worst prognosis over the 2-year follow-up period. After adjustment for client characteristics, cohort members whose last COT was for alcohol continued to experience a significantly higher rate of death compared with all others in the cohort. These findings add to those of a US cohort of treatment clients followed after discharge, in which alcohol and heroin clients were at greater risk than cocaine clients (Saitz et al., 2007). The greater mortality risk for this group may be due to the impact of alcohol-related chronic conditions that have developed due to chronic alcohol use prior to treatment engagement, or may relate to the high level of alcohol availability and cultural acceptability of alcohol consumption. To explore this, further research with cohorts of alcohol treatment clients is needed.
Clients discharged from cannabis treatment experienced a significantly lower rate of death. It is important to note, however, that CMRs for clients following treatment for cannabis use were significantly elevated when compared with age-matched general population peers – highlighting a population under-represented in the literature in terms of evidence-based intervention developed and evaluated with robust outcome measures that meaningfully assess effectiveness of treatment, but potentially at risk of elevated harms.
Clients who had engaged in treatment in relation to volatile substance use were found to have the highest rate of death. This may reflect the younger age of many volatile substance users, and also a combination of factors that increase complexity of case presentation and therefore increased risk of premature death. Further exploration of factors that influence outcomes of this high-risk population are needed to disentangle the relationships between substance use and other factors that contribute to harm for this population.
Limitations
This study has three main limitations: the accuracy and completeness of linkage methodology, the absence of key variables in ADIS, and the size of the extracted cohort group.
First, the completeness and accuracy of the data linkage between ADIS and NDI was limited by the use of deterministic methods with partial client identifiers. While it is likely that deterministic linkage methods underestimate mortality by missing clients who use nicknames or who have incomplete data, more evidence is needed regarding the extent to which linkage using partial identifiers underestimates rates. Despite this, the linkage process yielded robust results and a sufficiently large cohort to enable analysis of factors influencing mortality among this population. Furthermore, this approach is routinely used as a valid and appropriate methodological approach by the data custodian of the NDI, and has been utilised previously to provide valuable data to contribute to the understanding of patterns of mortality in cohorts of individuals with a history of substance use problems (e.g. Stoové et al., 2008, 2009).
Second, key variables were not recorded in ADIS, which are likely to influence the survival of drug treatment clients. Some variables in ADIS, such as polydrug use, were available but were not used due to incompleteness. Other potentially useful variables in ADIS, such as significant treatment goal achievements, are not consistently collected. Other variables that have been shown as important covariates for mortality among drug users that were not available include age of initiation into drug use and age of first injection (Bird, 2010). Furthermore, coding practices for predictor variables may have changed systematically over the time period examined as a result of policy changes. For example, additional drugs of concern, and different categories of existing drugs of concern, have been adopted during this time. To minimise the impact on results, only complete and consistently accurate variables were included in the analyses.
Another important issue is that most pharmacotherapy treatment provided in Victoria is not recorded in the ADIS dataset, as the pharmacotherapy treatment system in Victoria primarily involves treatment provided by general practitioners rather than specialist AOD treatment services. Accordingly, this study differs from most treatment mortality research in the addiction field, where the primary client population examined tends to consist of clients seeking treatment for opioid dependence in the form of opioid substitution pharmacotherapy. Whilst this may be seen as a limitation in terms of comparability of findings, this research provides an insight into diverse AOD treatment populations.
Conclusion
There is little international evidence examining mortality among populations of drug users following treatment engagement and cessation across multiple drugs of concern, and less is known in an Australian context. Whilst previous research has focused primarily on heroin and other opioid users engaging in pharmacotherapy treatment as a population perceived to be at greatest risk of premature death, this study has found that, after controlling for a range of demographic, health and drug use characteristics, risk of premature death is greatest for patients whose primary drug of concern is alcohol – with risk of death increasing with time since cessation of treatment. These findings highlight the need to increase awareness in the community as well as among clinicians of the range and magnitude of risks associated with harmful alcohol use patterns. Furthermore, the elevated risk of harm for clients following treatment for cannabis use compared with the general population reflects a group not well understood in terms of factors that influence risk of harm, or health and social benefits following treatment. There is an urgent need to identify risk and protective factors relevant to treatment engagement, treatment delivery and reduction of negative outcomes following cessation of treatment that support recovery and global improvements in health and social functioning for patients beyond the treatment episode. This information is necessary to inform optimal clinical care models, and for improved outcomes for clients following treatment engagement and cessation.
Footnotes
Acknowledgements
The authors would like to acknowledge and kindly thank the Australian Institute of Health and Welfare for access to NDI data, and the Victorian Department of Health for access to ADIS data.
Funding
This project was funded by the Victorian Department of Health.
Declaration of interest
We declare that none of the authors are in receipt of financial support, or have any relationship that may pose a conflict of interest in relation to the content presented in the submitted manuscript. Dan Lubman has received speaking honorarium for AstraZeneca and Janssen, as well as travel support from Lundbeck.