
Abstract
Objective:
Repetition of suicide attempts is common, but little is known about the relationship between switching methods of suicide attempt and the probability of completed suicide. This study aimed to determine the transition of methods chosen by individuals who repeat suicide attempts, and how the switched methods of suicide attempts influence the risk of suicide death.
Method:
All consecutive individuals (n = 2052) with an episode of non-fatal suicide attempt registered in a surveillance database provided by the Department of Health of the Keelung City Government from 1 January 2006 to 31 December 2010 were enrolled and followed up until the end of 2011. The earliest attempt recorded in the database was defined as the index attempt. Data on the time of subsequent completed suicide and methods chosen for repeated self-harm during the follow-up period were analyzed by performing a Cox proportional hazards regression.
Results:
Of the total subjects, 374 (18.2%) had at least one other attempted suicide and 50 (2.4%) eventually died by suicide. Subjects who used highly lethal methods in the index self-harm tended to switch methods in the next suicide attempt (p<0.001). Switching to a more lethal method was a significant predictor of completed suicide (adjusted hazard ratio (aHR) 7.05, 95% confidence interval (CI) 3.52–14.14). In addition, subjects who used charcoal-burning in the index self-harm attempt had a higher risk of subsequent suicide death (aHR 3.47, 95% CI 1.57–7.68).
Conclusions:
The findings in this study give us some insight into the patterns of methods in repeat suicide attempters. The intent behind switching methods of suicide attempt might be considered as an important item of clinical assessment of the seriousness of suicidal behavior.
Introduction
Suicide is one of the leading causes of premature mortality worldwide (Hawton and van Heeringen, 2009), and is also an important public health issue in Taiwan. Since 1997, suicide has become the ninth leading cause of death in Taiwan (Lin and Lu, 2008). Among the risk factors of suicide, a history of suicide attempt was identified as a main predictor of future attempts (Beghi and Rosenbaum, 2010; Beghi et al., 2013; Cedereke and Ojehagen, 2005). About one-half to two-thirds of people who attempt suicide are documented to have made a previous attempt (Sakinofsky, 2000). Comprehensive reviews found that the proportion of repeated suicide within 1 year was approximately 16% with non-fatal results and 2% with fatal outcomes (Carroll et al., 2014; Owens et al., 2002). In a recent hospital-based survey of suicide survivors in Taiwan, 38.2% had repeated suicide attempts and 3.4% died by suicide within 12 months after their index self-harm (Lee et al., 2012). Therefore, investigations of suicidal behavior and early recognition of high-risk groups are crucial steps in preventing subsequent suicide (Chung et al., 2008).
The method used during the previous or index suicide attempt has been demonstrated to serve as an important predictor of subsequent completed suicide (Runeson et al., 2010). Among the various suicide methods, poisoning and self-injuries with sharp instruments are generally identified as low-lethal methods, but the use of firearms, hanging and jumping from high places and drowning are methods with high lethality (Chen et al., 2009, 2011; Elnour and Harrison, 2008; Miller et al., 2004). Suicide by charcoal-burning has risen to epidemic levels in East Asia in recent decades (Chen et al., 2012; Wu et al., 2012; Yip et al., 2012) and has emerged as one of the leading methods contributing to suicide mortality in Taiwan (Chang et al., 2010; Lin et al., 2010; Pan et al., 2010; Thomas et al., 2011). Chen et al. (2011) reported that use of more lethal methods in the index self-harm was associated with higher mortality, but this was accounted for by gender. Runeson et al. (2010) indicated that individuals who previously attempted suicide by hanging, strangulation, or suffocation had the worst prognosis. Previous community studies in Taiwan demonstrated that non-fatal suicide attempters who used hanging or charcoal-burning in their index suicide attempt had the highest risk of subsequent suicide deaths, compared with people who took an overdose (Kuo et al., 2008, 2012).
Repetition of self-harm is common, and the switching of methods by suicide attempters during the next attempt may indicate they are trying another method to increase the likelihood of death (Sakinofsky, 2000). Our previous report showed that most people who used low-lethal methods stayed at the same lethality level of methods in their second attempt, but those using high-lethal methods were more likely to change methods in their second attempt (Huang et al., 2014). In individuals with repeated episodes, it may be preferable to look at the last non-fatal episode, as it is closer in time and therefore potentially more relevant to the fatal act. Nishimura et al. (1999) suggested that although many people who attempt suicide tend to choose the same method in their next attempt, they may switch to a different level of lethality and thus be more likely to die. Runeson et al. (2010) reported that most of those who completed suicide used the same method as they did at the index attempt. Moreover, Bergen et al. (2012) found that method-changing in repeated self-harm was not associated with suicide deaths. To date, few studies have explored variations in methods of suicide attempts in individuals exhibiting repeated self-harm behaviors. Thus, the relationship between changes in methods of suicide attempts and the risk of completed suicide continues to be unclear.
Therefore, the aim of this study was (1) to determine the changes in methods of suicide attempts chosen by individuals who repeatedly self-harm, and (2) to investigate how the switched methods influence the risk of completed suicide.
Methods
Study sample and data collection
The study received approval from the Institutional Review Board of Chang Gung Memorial Hospital. All consecutive individuals with an episode of non-fatal suicide attempt registered in a surveillance database provided by the Department of Health of the Keelung City Government from 1 January 2006 to 31 December 2010 were enrolled. Keelung City, which has approximately 0.4 million inhabitants, is a harbour city located in north-eastern Taiwan, and has had one of the highest suicide mortality rates in Taiwan this past decade (the average suicide mortality rate per 100,000 people was 25.1) (Lin et al., 2010). In collaboration with the local health authority, the Suicide Prevention Center was established in 2005 to collect a surveillance database and set up a suicide prevention program. In this system, once the staff in the health sectors (emergency departments at hospitals, general practice and local public health centers) notice any individual with self-harm, a structured case notes form is used to record the subjects’ basic information and methods of suicide attempts. A suicide attempt was defined as any potentially life-threatening act of self-harm requiring treatment. All of the health sectors are required to complete and submit the written form and fax it to the Suicide Prevention Center of Keelung City after each attempt. The surveillance database was collected in electronic format, and the demographic variables consisted of sex, dates of birth and death, marital status, educational levels and methods of suicide attempts.
During the study period, 2052 unique subjects who survived a non-fatal index suicide attempt constituted the sample. If a subject had made several suicide attempts during the study period, the earliest one recorded in the database was considered as the index attempt. Follow-up was then carried out to the end of 2011, and all subjects were followed for at least 1 year. A suicide death was confirmed by linking the surveillance database with the Death Certification System (DCS) of the Department of Health in Taiwan compiled from 1 January 2006 to 31 December 2011. Of the study subjects, 374 (18.2%) had at least one other attempted suicide and 50 (2.4%) eventually died by suicide during the follow-up period. Figure 1 is a flow chart of study sampling and data collection .
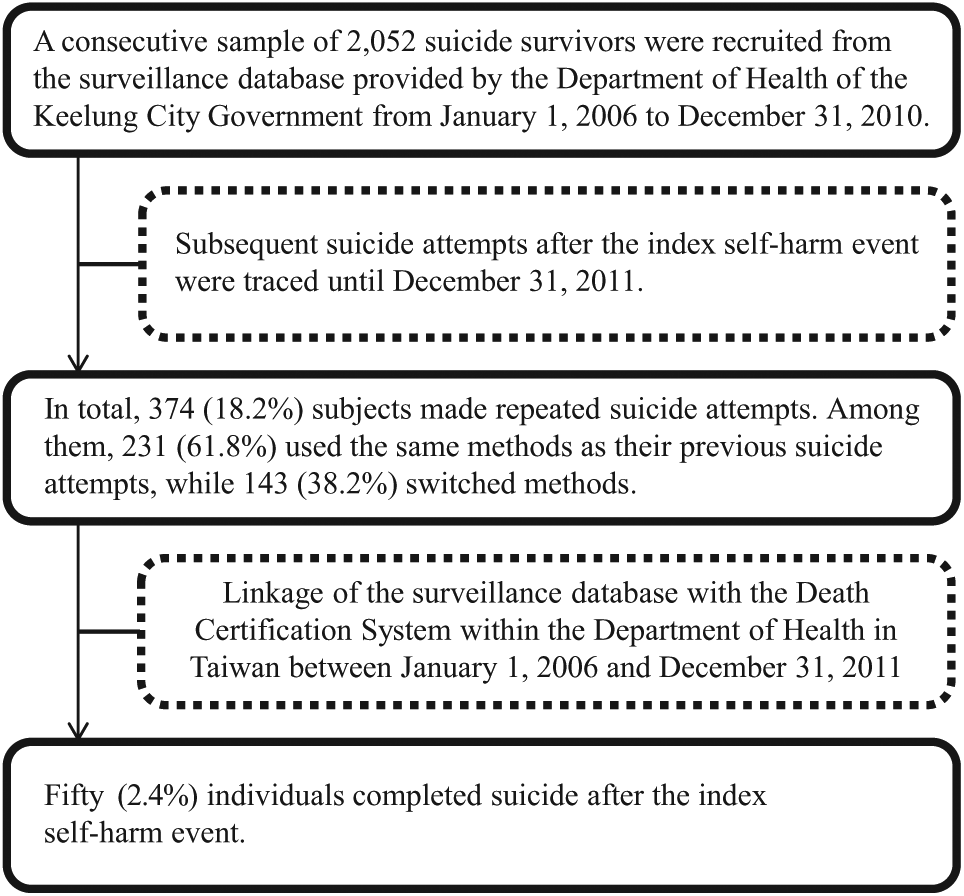
Flow chart of study sample and data collection (the unique subjects with a non-fatal suicide attempt, suicide repetition, and subsequent suicide mortality).
Identification of methods of suicide
The methods of suicide were classified using the codes of the International Classification of Disease, Ninth Revision (ICD-9-CM). Based on previous epidemiological evidence (Chen et al., 2009, 2011; Elnour and Harrison, 2008; Miller et al., 2004), suicide methods were classified into a low lethality group and a high lethality group. However, suicide by charcoal-burning, as a special method, was categorized as a single group. In the end, three groups of suicide methods were used in this study. The first, the low-lethal group, consisted of poisoning by solid or liquid substances (drug overdose, E950) and using cutting and piercing instruments (self-cutting, E956). The second, the charcoal-burning group, included subjects with self-harm by poisoning using other gases and vapours (E952). If a victim completed suicide by burning charcoal in Taiwan, the cause of death was classified as E952. In Taiwan, the proportion of E952 suicides has increased rapidly since 1999 (Pan et al., 2010). Previous reports have suggested that nearly all (95.6%) of the E952 suicides in Taiwan likely resulted from charcoal-burning (Chang et al., 2010; Liu et al., 2007), and suicide by charcoal-burning is highly lethal (the fatality rate reached 50.1%) (Lee et al., 2014). We assumed that all of the E952 cases in this study were charcoal-burning suicides. The third group, the other high-lethal group, involved poisoning by gas used domestically (E951), hanging (E953), drowning (E954), firearms, air guns and explosives (E955), jumping from high places (E957), and other and unspecified means (E958).
Statistical analysis
Data were analyzed using the statistical software package SPSS, version 16.0 (SPSS Inc., Chicago, IL, USA). Variables are presented as either the mean (standard deviation) or frequency. Two-tailed p-values <0.05 were considered statistically significant.
The McNemar–Bowker test was used to examine the proportion of switching methods among individuals with repeated suicide attempts. Subjects were categorized into those who used the same methods as their previous suicide attempts and those who switched methods. Each person’s first presentation within the study period was used in the calculation of risk over time. All individuals traced until 31 December 2011 for any length of time from their index self-harm event were entered into survival analysis. The time function in the survival analysis was calculated as the number of months from the index episode of self-harm to December 2011 (end of follow-up) for those who survived until then, or until the date of suicide death if it preceded the end of the follow-up interval. Cox regression models were fitted to estimate the effects of switched methods on subsequent suicide death, controlling for sex, age, marital status, educational levels and methods of the index suicide attempt. Unadjusted hazard ratios (HRs) and adjusted HRs (aHRs) with 95% confidence intervals (CIs) were calculated, respectively. Survival curves stratified by suicide methods that have been repeated or switched during the follow-up period were also expressed by Cox regression.
Results
The mean age of the 2052 subjects with non-fatal suicide attempts was 40.4 ± 15.6 years. Overall, 1388 (67.6%) of the subjects were women and 664 (32.4%) were men; 537 (26.2%) were single, 773 (37.7%) were married, and 728 (35.5%) were divorced or widowed (14 subjects did not supply information on marital status); 760 (37.0%) were educated until junior high school or lower, and 1292 (63.0%) had an educational level of high school or above. The methods of the index self-harm included drug overdose (n=1250, 60.9%), self-cutting (n=469, 22.9%), charcoal-burning (n=158, 7.7%), jumping from a high place (n=32, 1.6%), drowning (n=38, 1.9%), hanging (n=37, 1.8%), gas inhalation (n=12, 0.6%) and other violent methods (n=56, 2.7%). The mean follow-up time of the total subjects was 37.5 ± 20.2 months.
After the index self-harm event, 374 (18.2%) subjects made another suicide attempt (including fatal and non-fatal) during the study period. Among those individuals with repeated suicide attempts, 231 (61.8%) used the same method again and 143 (38.2%) switched methods. Among the subjects who used low-lethal methods, charcoal-burning, and other high-lethal methods in the index self-harm event (Table 1), the proportion who repeated the same level of lethality in their second suicide attempt were 83.2%, 50% and 42.9%, respectively (McNemar–Bowker test: 23.84, p<0.001).
Distribution of methods used in the index suicide attempt and in the second suicide attempt (n = 374).
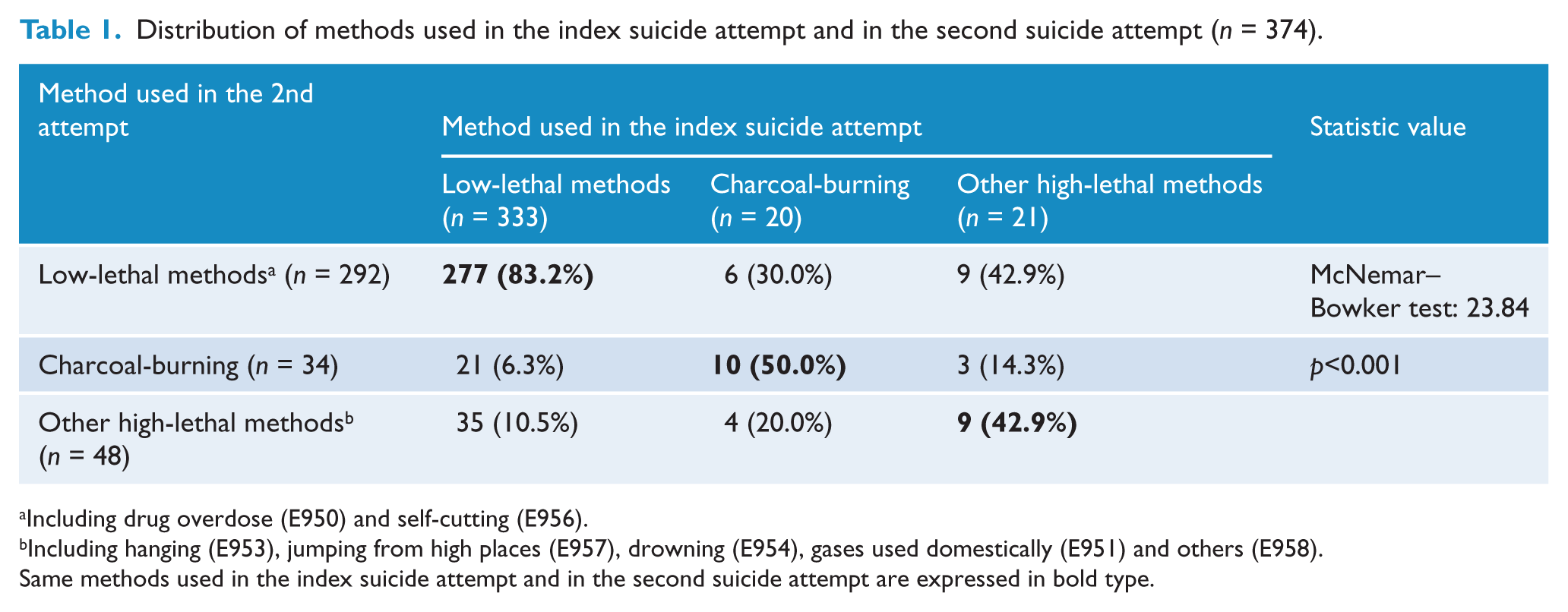
Including drug overdose (E950) and self-cutting (E956).
Including hanging (E953), jumping from high places (E957), drowning (E954), gases used domestically (E951) and others (E958).
Same methods used in the index suicide attempt and in the second suicide attempt are expressed in bold type.
Among the 50 subjects that eventually died due to suicide, the most common suicide methods included hanging (40%), followed by charcoal-burning (34%) and jumping from high places (14%). Only 11 (22%) of the suicide mortalities used a method classified at the same lethality level as in the penultimate non-fatal suicide attempt; 39 (78%) of the mortalities switched to a method classified at a different lethality level to complete suicide (Table 2). The proportions of subjects who used low-lethal methods, charcoal-burning, and other high-lethal methods in the penultimate episode of self-harm that maintained the same method to complete suicide were 5.3%, 71.4% and 80%, respectively (McNemar–Bowker Test: 36.33, p<0.001).
Distribution of methods used in the penultimate suicide attempt and in the completed suicide (n = 50).
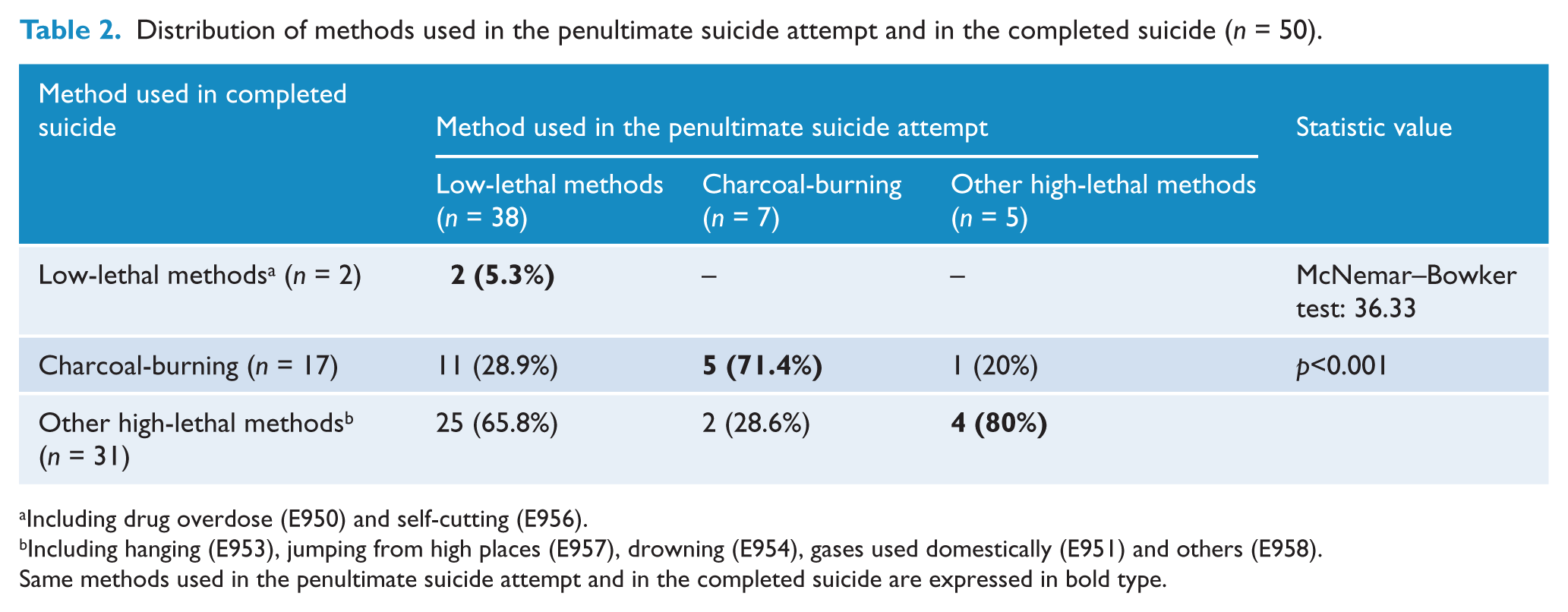
Including drug overdose (E950) and self-cutting (E956).
Including hanging (E953), jumping from high places (E957), drowning (E954), gases used domestically (E951) and others (E958).
Same methods used in the penultimate suicide attempt and in the completed suicide are expressed in bold type.
The HR of related variables for suicide death (n=50) after the index self-harm event among repeated suicides were calculated (Table 3). In unadjusted Cox regression analyses, suicide death was more likely among males (HR=3.30, p<0.001), subjects older than 65 years (HR=4.45, p=0.001), when charcoal-burning was used in the index self-harm event (HR=4.43, p<0.001), and among subjects who switched methods of suicide attempts (HR=6.83, p<0.001). In the adjusted Cox proportional hazard model, males (aHR=2.14, p=0.015), subjects aged from 50 to 64 years (aHR=3.11, p=0.019), those older than 65 years (aHR=7.44, p=0.001), those who used charcoal-burning in the index self-harm event (aHR=3.47, p=0.002), and subjects who had switched methods of suicide attempts (aHR=7.05, p<0.001) independently predicted suicide mortality.
Hazard ratio (HR) of suicide death (n=50) after the index self-harm event for related variables by Cox proportional hazards model.
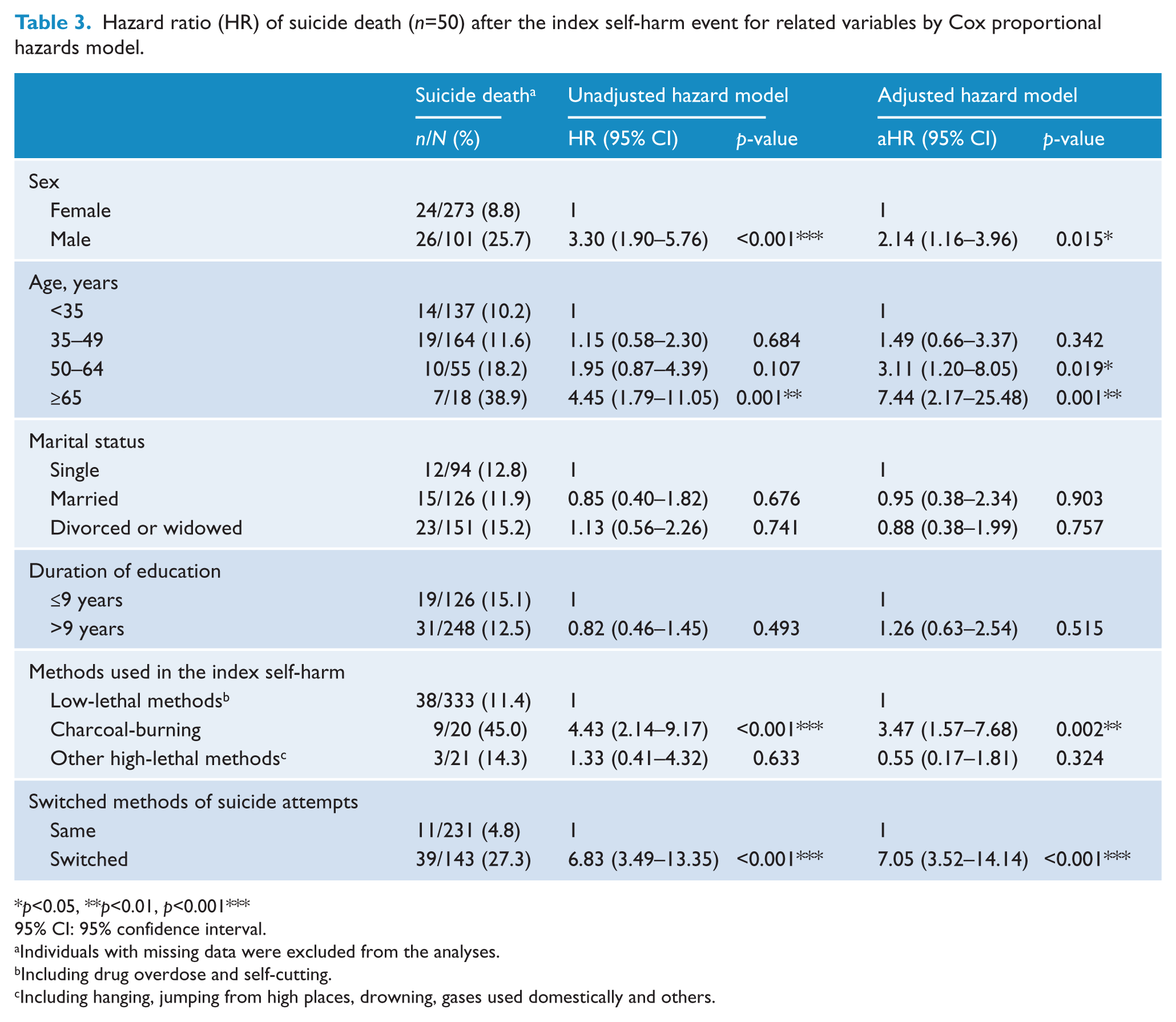
p<0.05, **p<0.01, p<0.001***
95% CI: 95% confidence interval.
Individuals with missing data were excluded from the analyses.
Including drug overdose and self-cutting.
Including hanging, jumping from high places, drowning, gases used domestically and others.
Figure 2 shows the survival curves during the follow-up period stratified by suicide methods that have been repeated versus switched, controlling for sex, age, marital status, educational levels, and methods of the index suicide attempt. We further analyzed the effects of switching methods on suicide deaths in different groups categorized by the methods used for the index self-harm. For the low-lethal group, switching methods significantly increased the risk of suicide mortality (aHR=15.68, p<0.001). For the charcoal-burning group (aHR=1.41, p=0.781) and the other high-lethal group (aHR=1.17, p=0.999), switching methods was not significantly associated with suicide mortality.
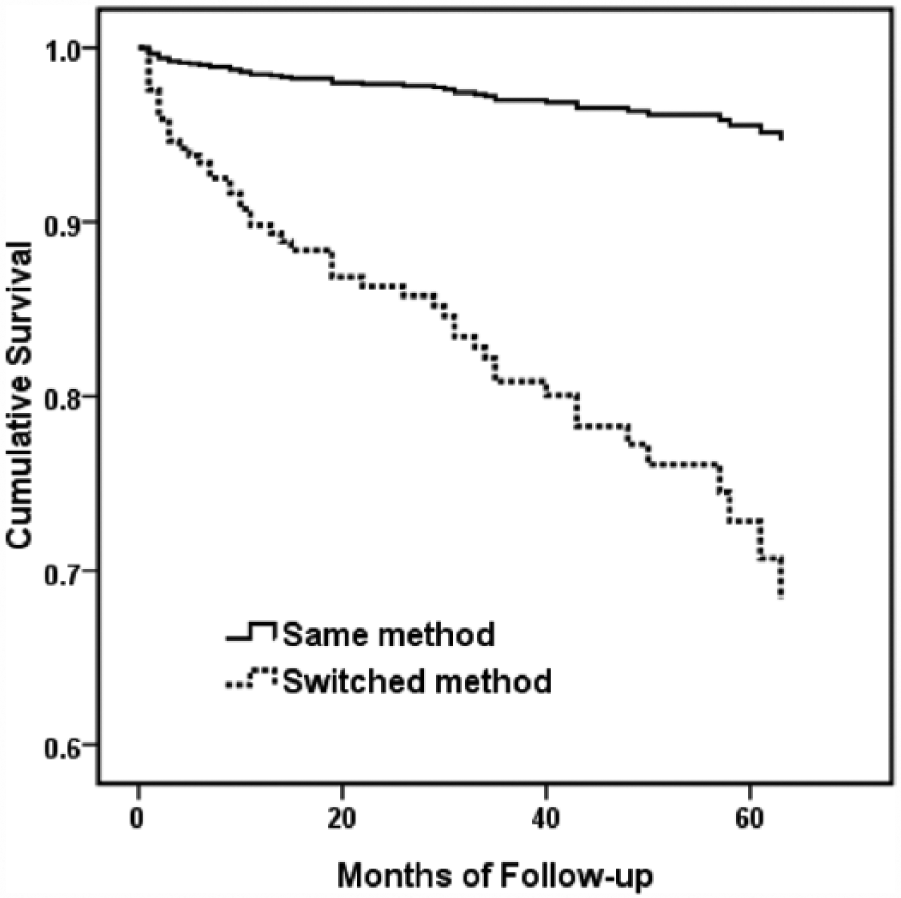
Survival function expressed by Cox regression of suicide mortality in people with suicide repetition from 2006 to 2011 in Keelung City, Taiwan. Stratified by subjects who repeated the method of the index suicide attempt (solid line) and/or switched methods (dashed line) in their second suicide attempt, controlling for sex, age, marital status, educational levels, and methods of the index suicide attempt.
Discussion
Among the subjects who eventually died, those who used a low-lethal method in the last attempt mostly changed methods to complete suicide, and those who used a highly lethal method mostly maintained the same method. Switching methods of suicide attempts is a strong predictor of completed suicide in subjects who previously chose a low-lethal method in the index self-harm. In addition, subjects who used charcoal-burning in the index self-harm had a higher risk of subsequent suicide death.
Switching methods of suicide attempts
In our community-based study of suicide survivors, 18.2% of them had a repeated episode of self-harm. This implies that most people did not switch methods of suicide attempts. There were 50 suicide survivors who eventually died by suicide during the follow-up period. They accounted for 2.4% of the original study sample, and for 13.4% of the repeated suicide attempters. A recent systematic review indicated comparable findings, that the 1-year rate of repeated suicide attempt was 16.3%. The risk of suicide death was 1.6% in the 12 months after an index attempt and 3.9% after 5 years (Carroll et al., 2014). In addition, we found that drug overdose and self-cutting accounted for the greatest number of index self-harm events, and hanging and charcoal-burning comprised the greatest number of suicide mortalities; previous epidemiologic studies in Taiwan revealed findings similar to ours (Chen et al., 2011; Kuo et al., 2012; Thomas et al., 2011).
Among individuals with repeated suicide attempts in this study, 79.1% used the same method in the first two episodes of self-harm. The proportion of those using the same method was higher among subjects who chose low-lethal methods in the index attempt (83.2%) compared to the charcoal-burning group or the other high-lethal group. Individuals with low-lethal methods exhibited a greater degree of help-seeking behavior and had a history of more low-lethal methods of suicide attempts (Horesh et al., 2012). People who attempted suicide using low-lethal methods might have a higher probability of para-suicide and suicide communication, and thus a greater probability of keeping the same method in a reiteration of self-harm (Chesin et al., 2010). However, we found that 76% of those who eventually completed suicide actually chose a low-lethal method in the last attempt (Table 2). In the adjusted Cox regression model, switching methods of suicide attempts carried a sevenfold increased risk of suicide deaths among subjects with repeated self-harm and an over 15-fold increased risk in subjects who chose a low-lethal method in the index self-harm. Similar to our findings, Bergen et al. (2012) reported that 60% of repeated suicide attempters who eventually died by suicide had switched methods from self-poisoning. This suggests that people who repeatedly chose the same low-lethal method for self-harm might have a low probability of subsequent suicide death. Nevertheless, if people who initially used a low-lethal method for self-harm changed methods in the next attempt, this may indicate that they have a stronger intent to die and that they are searching for another method to increase the likelihood of suicide completion.
Subjects who used charcoal-burning (50%) or other high-lethal methods (57.1%) in the index self-harm event were more likely to change methods in the second suicide attempt compared to subjects who chose low-lethal methods (16.8%). However, switching methods of suicide attempts did not significantly predict suicide death in the charcoal-burning group and the other high-lethality group. Among the subjects who eventually died, those who used highly lethal methods in the penultimate attempt mostly maintained the same method in the final attempt. In general, choosing a high-lethal method in the index self-harm event may indicate that the person has a strong will and great intent to implement of the suicide act. These subjects may have a higher probability of trying another method after the previous non-fatal suicide attempt. Nevertheless, the mortality rate did not significantly increase with the use of another method, perhaps because the subjects were not familiar with the new method. Nishimura et al. (1999) reported a significant difference in the choice of methods between last attempted suicide (the most common method was injury to themselves) and the completed suicide (hanging was the most common method). If suicide attempters changed their method of suicide, they tended to choose a more lethal one. However, if suicide victims chose the same method as in their last attempt, they tended to use a more lethal and more violent way to increase the likelihood of death.
‘The Gateway Theory’ suggests that non-suicidal self-injury (NSSI) and suicidal behavior exist along a spectrum of self-harm behaviors, with NSSI at one extreme and completed suicide at the other extreme (Whitlock et al., 2013). The theory assumes that NSSI may be a gateway form of self-injury that leads to more extreme forms of self-injury with similar experiential qualities (i.e. suicidal attempts) and eventually increases the rate of suicide death (Hamza et al., 2012). Based on this theory, a continuum of self-harm behaviors contains a shift from a less lethal non-fatal method to a more lethal method for suicide (from poisoning or self-cutting to high-lethal methods) by the individuals involved. By contrast, if the individuals have already attempted suicide using high-lethal methods, this may indicate that they are close to the extreme of completed suicide. The risk of death, therefore, is not significantly altered by whether they changed a method or not in the next suicide attempt. This gives us some insight into implications for clinical practice. In addition to identifying those few individuals with a relatively high risk of suicide (i.e. those using high-lethal methods), clinicians should still pay attention to those individuals who used low-lethal methods in their last episode, but will switch to high-lethal methods in the next attempt. Suicide risk cannot be predicted on the basis of non-fatal methods alone; rather, a comprehensive assessment of the underlying reasons for suicide and intent to switch methods of suicide attempt are important in clinical settings. Although directly asking a distressed patient how they would attempt suicide next time might be awkward, it is an inevitable approach to predict and prevent further lethal suicide attempts. Clinicians should attempt to be mindful to identify intention to re-attempt suicide in suicide survivors, and to clarify potential suicide methods as part of their clinical risk assessments.
Method used in the index suicide attempt as a predictor
We found that the risk of subsequent suicide mortality was significantly higher in subjects who used charcoal-burning in the index self-harm event. This result was consistent with those of previous epidemiologic studies in Taiwan (Kuo et al., 2008, 2012). The demographic characteristics of individuals who choose charcoal-burning as a method of suicide attempt and those using other methods might differ (Lee et al., 2014; Tsai et al., 2011). Suicide by burning charcoal requires a well-organized plan and complicated process (i.e. buying barbecue charcoals, properly sealing the door and windows). Therefore, choosing charcoal-burning as the method of suicide attempt is more likely to be deliberate self-harm and less likely to be impulsive suicide or para-suicide. Previous studies have revealed that a past history of deliberate self-harm is a strong predictor of suicide repetition (Haw et al., 2007). These factors may be possible explanations for the especially high risk of subsequent suicide death among people who initially chose charcoal-burning as a method of suicide attempt, no matter whether they changed methods.
In general, people who used highly lethal methods may have a higher probability of re-attempting a fatal suicide after the previous non-fatal attempt. International studies have indicated that the use of more lethal methods in the index episode, particularly the use of hanging, was associated with higher mortality (Kuo et al., 2012; Runeson et al., 2010). However, we found that other highly lethal methods used in the index self-harm were not significantly associated with subsequent suicide mortality. The findings of some studies were comparable with ours, after controlling for socio-demographic factors (Chen et al., 2011; Christiansen and Jensen, 2007). Differences in socio-cultural circumstances and in classification of methods of suicide attempts might account for the discrepant results of these studies. For example, some researchers analyzed suicide methods individually (Kuo et al., 2012; Runeson et al., 2010), but we regarded high-lethal methods, except charcoal-burning, as a single group. Therefore, the effect of the individual method of suicide attempt is unclear in our study. In addition, the sample size of the other high-lethal group was relatively small, so the results of this study should be confirmed using a larger sample size. Furthermore, we found that older adults (≥50 years) with a repeated suicide attempt were more likely to die by suicide than younger adults (<35 years). Possible explanations are that the elderly might re-attempt suicide by utilizing highly lethal methods, and their vulnerable health conditions were more intolerable to the impact of suicide re-attempts (Lee et al., 2014).
Limitations
There are several limitations in this study. First, the surveillance database in this study lacks comprehensive information about other potential determinants of suicide, including the circumstance and intent of the attempt, psychiatric diagnoses and physical condition, thus limiting the analysis of the association among these parameters and the methods of suicide attempts. In addition, subjects who moved after the index attempt might have been missed by this surveillance system. Second, the index suicide attempt represents the first suicide act detected during the study period, but is not necessarily the first attempt in that individual’s lifetime. If a subject had attempted suicide prior to registration in the surveillance database, changes in suicide methods may have already happened and remain undetectable in this study. Therefore, the effect of method-switching on suicide deaths might be over-estimated, and caution should be taken in applying these results to clinical practice. A longer follow-up is warranted to clarify whether the method of the first suicide attempt and/or the switched method in a person’s life predicts the pattern of subsequent suicide mortalities. Third, the sample size of those who completed suicide was small; therefore, the statistical power of analyses in this study is limited. Moreover, we did not examine whether the proportional hazards assumption was met for the data in the current study. It was undetermined whether the effect sizes remained constant across time, or differed as more time passed after index suicide attempts. Finally, we assumed that the use of the high-lethality method indicates high suicide intent. However, the associations between suicide intent and the choice and lethality of method are complex. They may not be related if the attempters have inaccurate knowledge of the lethality of the method. Moreover, people with high suicide intent may use the means that is immediately available but not necessarily the most lethal one.
Conclusions
The findings in this study give us some insight into patterns by which individuals switch methods to those that are more likely to end in suicide. Although low-lethal methods of self-harm rarely contribute to suicide mortality, switching to a more lethal method in the next suicide attempt is a strong predictor of completed suicide in subjects who chose a low-lethal method in the index self-harm. This may provide a clue to clinicians that the intent of switching methods should be considered as an important item in clinical assessment of the seriousness of suicidal behavior, particularly in those who initially choose a low-lethal method. Further investigation with a larger sample size and longer follow-up is warranted to elucidate the effect of individual patterns of switching the method of suicide attempt on subsequent mortality.
Footnotes
Acknowledgements
The authors wish to express their deepest gratitude to the Department of Health, Keelung City Government for providing the suicide data.
Funding
This study was supported by the Chang Gung Memorial Hospital Research Project (CZRPG290021).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.