
Abstract
Keywords
It is well recognized that following presentation with deliberate self-harm (DSH) there is an increased risk of suicide and/or all-cause death [1–11]. However, it is less well recognized that there is an increased overall mortality for patients following presentation with DSH [1], [2], [4], [12]. In the Hunter Area Toxicology Service (HATS) population we have described a five-fold increase in standardized mortality rate for self-poisoning patients, with a greater increase in males than females, following an initial presentation with deliberate selfpoisoning (DSP) [13].
Part of the increased mortality is explicable through an increased risk of suicide, but there remains an unexplained component, due to non-suicidal mortality. This includes death by disease or natural causes, uncertain or undetermined causes, accident and homicide [1–7]. Some of these categories may include misclassified suicidal deaths [14]. This may explain a previously described increase in mortality from accidents, but not from natural causes, following medically serious suicide attempts [11].
The aim of the present study is to quantify the increased non-suicidal mortality subsequent to presentation with self-poisoning in an Australian hospital treated population, and to identify risk factors for non-suicidal death in this patient group. Secondary aims are to quantify the increased mortality from accidental death and natural-cause death, and to identify risk factors for these outcomes.
Method
A prospective longitudinal cohort design was used, with datalinkage between the Hunter Area Toxicology Service (HATS) patient database, described in more detail elsewhere [15], and the National Death Index (NDI) of the Australian Institute of Health and Welfare (AIHW) [16]. The HATS services the Newcastle and Lake Macquarie regions of New South Wales and provides a co-ordinated toxicological and psychiatric model of patient care [17]. Patient data are entered prospectively into a relational electronic database. The NDI contains mortality data provided from death certificates from the Registrars of Births, Deaths and Marriages in all Australian states and territories. Follow-up was for the duration of the study, a maximum of 10 years. Subjects were consecutive cases of DSP and recreational self poisoning, aged 10 years and over, presenting for hospital treatment to HATS during the time period of the study. All subjects from 1 January 1991 to 31 December 2000 were selected and the first episode in the period was used as the index episode for all analyses. Transgender patients and patients who died in hospital during their index admission were excluded.
Data were obtained from the NDI for case matching, and to determine cause and time of death. Cause of death was recorded from the death certificate according to ICD-9 or ICD-10 [18]. Those patients with cause of death attributed to suicide were excluded from the analysis. The NDI matching process uses a probabilistic method that matches cases by first name, last name, date of birth, maiden name and sex, and has a reported sensitivity of 88.8% and specificity of 98.2% [16]. The data-linkage was performed for deaths occurring on or before 31 December 2000.
We examined three outcome variables: non-suicide death (death from all causes excluding suicide), ‘natural’ cause death (death from all causes excluding suicide, accident and homicide), and accidental death (death as a result of accident or homicide). Age adjusted allcause death, accidental death and suicide death rates were obtained from the AIHW and non-suicide death rates were calculated by subtracting the suicide rates from the corresponding all-cause death rates. Similarly, ‘natural’ cause death rates were determined by subtracting the accidental death rates and the suicide death rates from the all-cause death rates. Age-standardized mortality ratios were calculated for nonsuicide death, accidental death and ‘natural’ death for the male, female and combined patient groups.
The independent variables were: type of self-poisoning (deliberate or recreational, classified by emergency department staff and reviewed by toxicology and psychiatry staff at a weekly review meeting); age; gender; history of lifetime and current substance dependence and/ or abuse, and previous ‘suicide attempt’ (emergency department ratings by resident medical staff); prescribed medications (as indicators of serious medical conditions), psychiatric diagnoses (major DSM-IV categories) [19]; and discharge destination (home, self-discharge/absconding, voluntary public psychiatric hospital, involuntary public psychiatric hospital, private psychiatric hospital, general hospital/nursing home and other). The ‘other’ discharge category included discharge to gaol, police custody, hostel and the street. Psychiatric diagnoses were made according to DSM-IIIR or DSM-IV by psychiatric staff after direct clinical assessment of the patient and these diagnoses were reviewed at a subsequent weekly meeting. Individual disorders were mapped to DSM-IV major diagnostic categories for analyses and reporting. Those cases not seen by the psychiatry service were excluded from the multivariate analysis as ‘missing data’. Absence of psychiatric assessment was examined as an independent variable, but was not included in the multivariate analysis.
Cox proportional hazards modelling was used for both univariate and multivariate statistical tests using the ‘stcox’ command of Stata® V.8 [20], [21]. All independent variables were initially tested using univariate analysis and those variables significant at the p < 0.05 level were included in the multivariate analyses, using the ‘sw stcox’ command of Stata® V.8. The multivariate testing employed a backward stepwise technique. Results from the multivariate analysis were expressed as adjusted hazard ratios (HR) with 95% CI. Internal standardization was used to determine the standardized mortality ratios and their 95% CI using Stata® V.8 [20].
The Hunter Area Research Ethics Committee and the AIHW ethics committee approved the research protocol.
Results
Cause of death
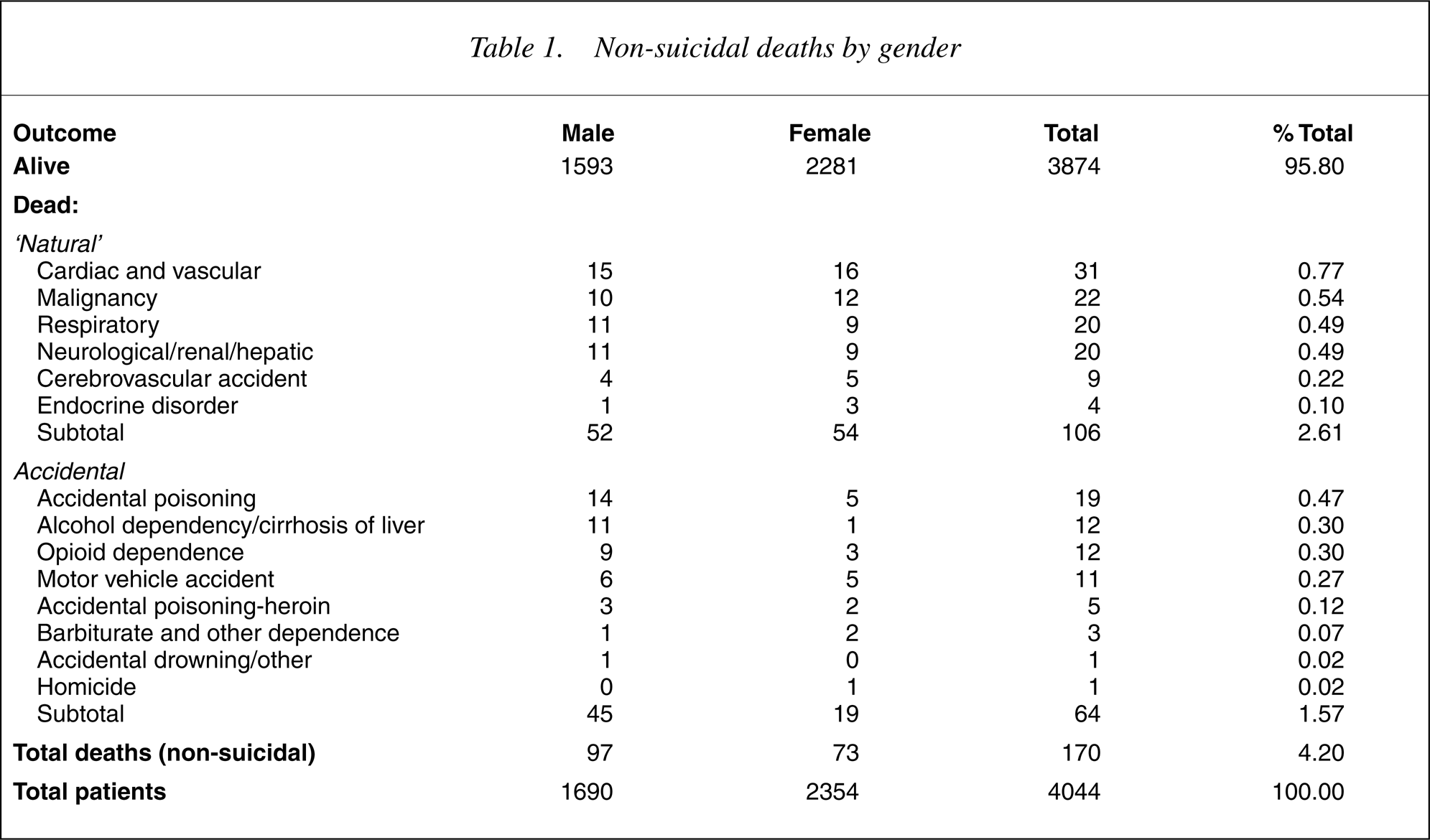
A total of 4044 patients were identified as being eligible for inclusion in the study. One hundred and seventy of these patients subsequently died from causes other than suicide (Table 1). The cause of death was accidental for 64 and ‘natural’ causes for 106. The failure curves (Fig. 1) indicate that at 10 years after presentation, nine percent of the cohort would be expected to die from non-suicide death, with six percent from ‘natural’ causes and three percent from accidental death or homicide.
Failure curves for non-suicide death.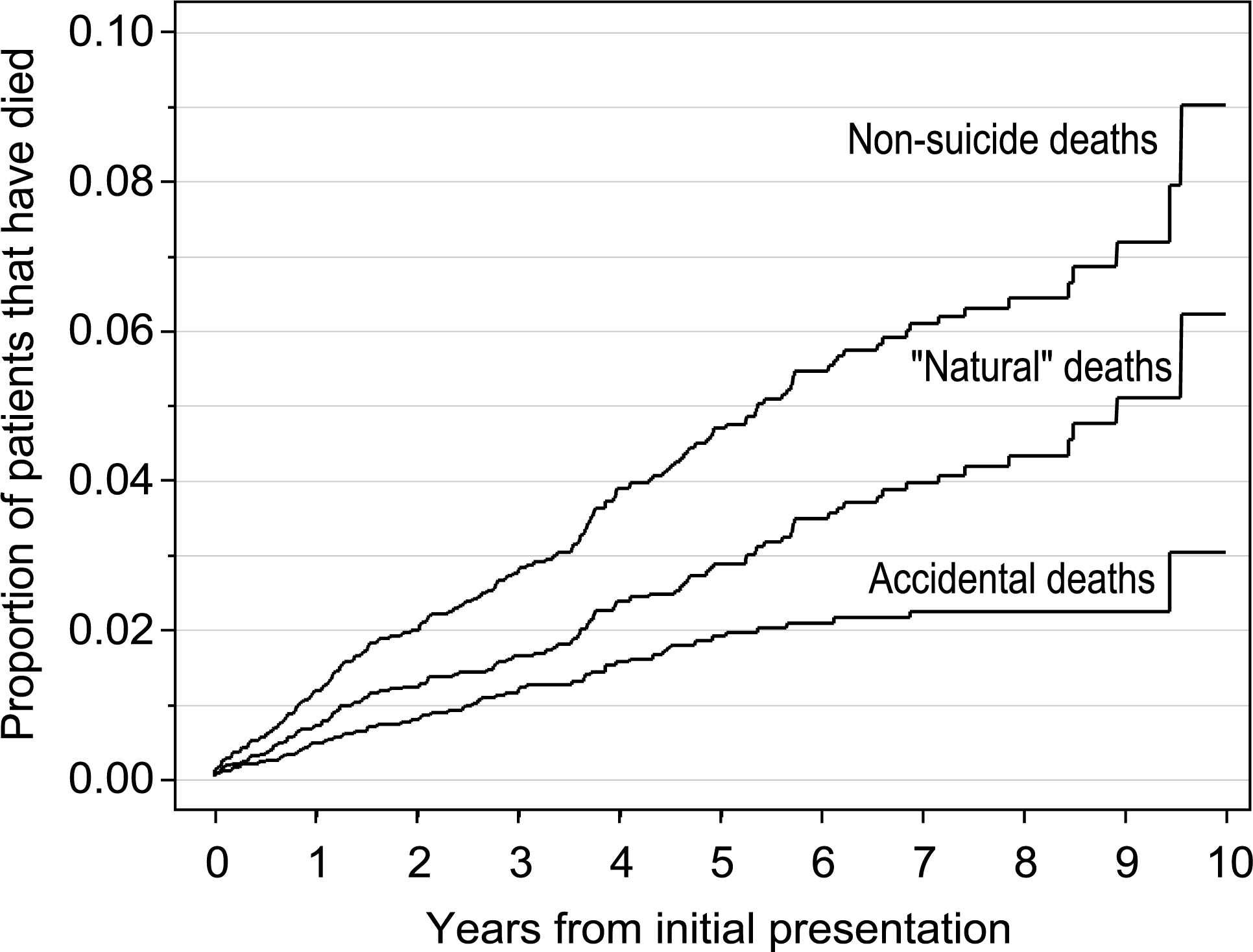
Non-suicidal deaths by gender
The standardized mortality ratios (95% CI) for non-suicidal death for males, females and combined were 4.98 (4.08–6.07), 3.78 (3.0–4.75) and 4.20 (3.62–4.88), respectively. The standardized mortality ratios (95% CI) for accidental death for males, females and combined were 14.16 (10.54–19.04), 12.86 (8.20–20.17) and 12.40 (9.69–15.88), respectively. The standardized mortality ratios (95% CI) for ‘natural’ death for males, females and combined were 3.26 (2.50–4.26), 3.02 (2.32–3.95) and 3.02 (2.50–3.65), respectively.
Univariate analysis of risk factors
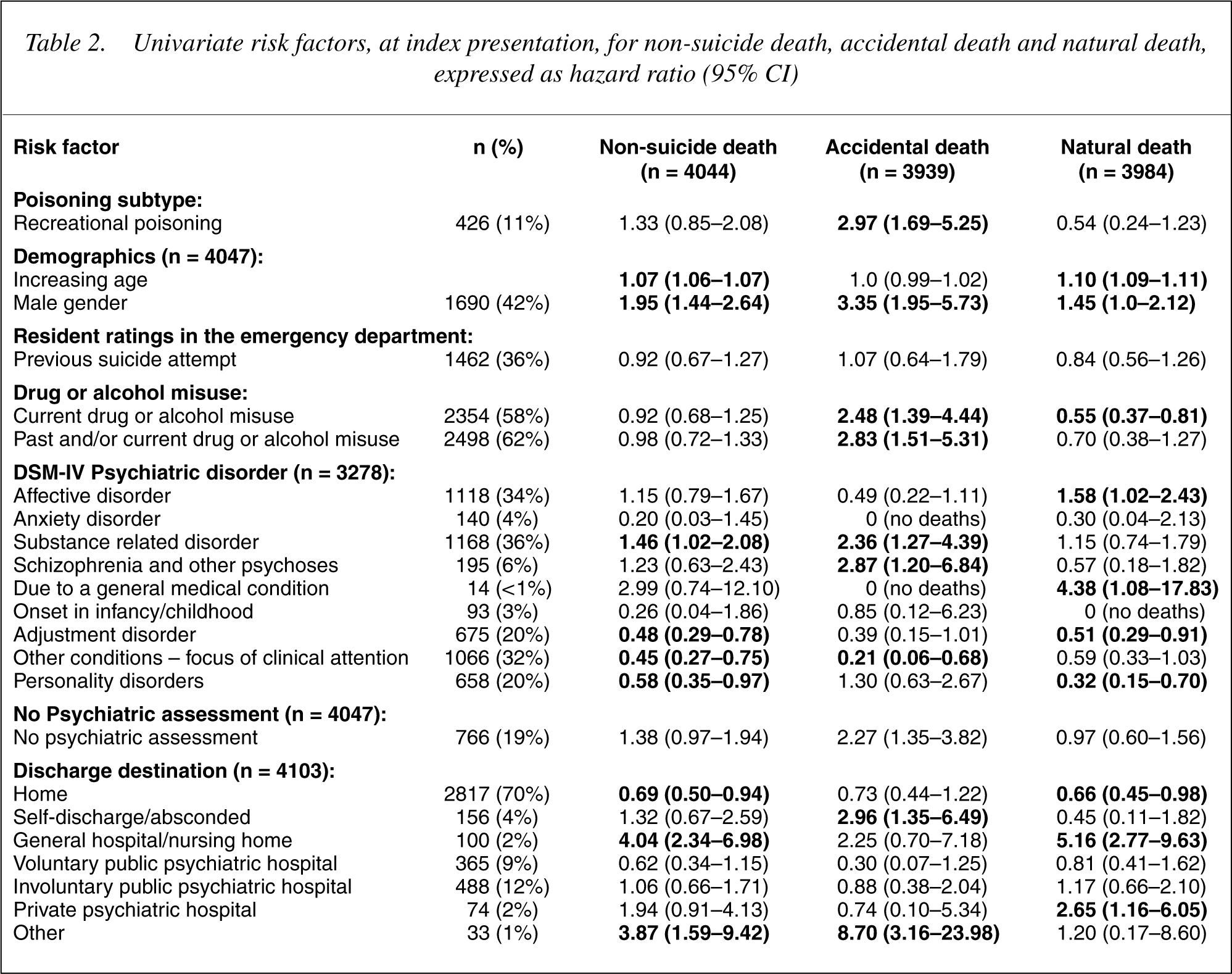
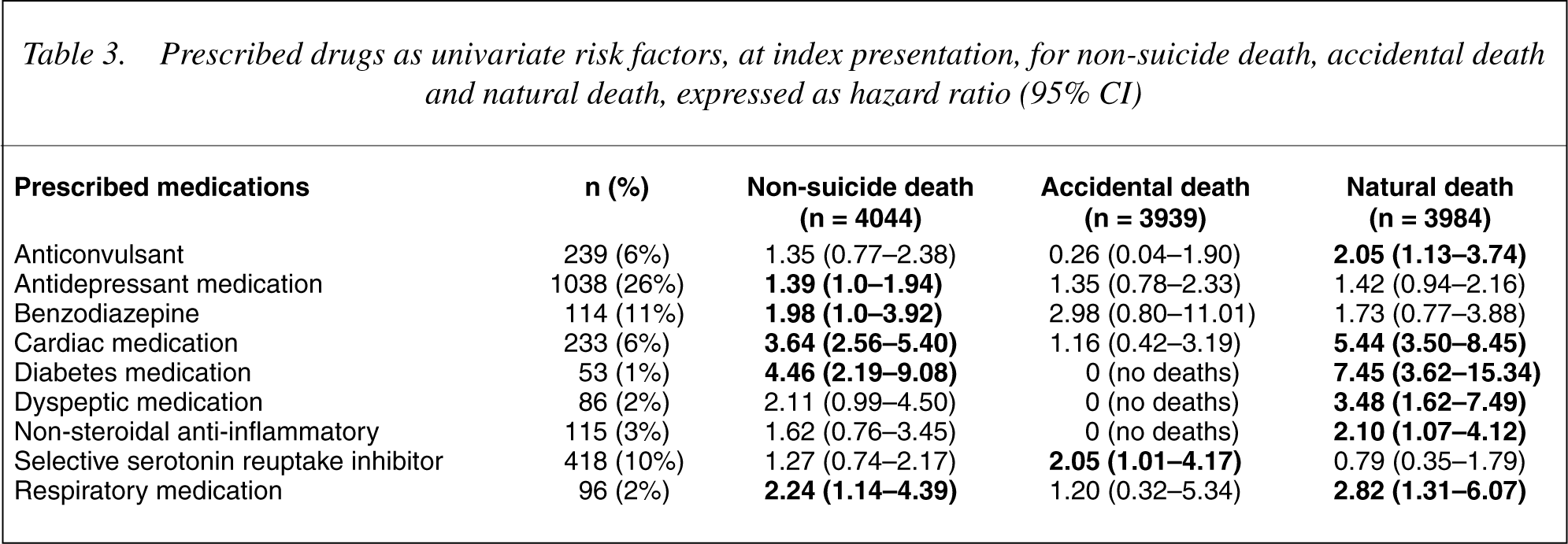
On univariate analysis (Table 2), there was little overlap between the risk factors for accidental death and those for ‘natural’ cause death. Male gender was the only risk factor common to all three outcomes. Increasing age, affective disorder, psychiatric disorders due to general medical conditions, discharge to a general hospital/nursing home and discharge to a private psychiatric hospital were risk factors for natural cause death. Drug or alcohol misuse (current and lifetime), ‘recreational’ overdose, substance related disorder (DSM), schizophrenia, absence of psychiatric assessment, prescription of a selective serotonin reuptake inhibitor (SSRI), self discharge/absconded and ‘other’ discharge destination were risk factors for accidental death. Prescribed drugs for medical (non-psychiatric) conditions were predominantly risk factors for non-suicidal and ‘natural’ cause death rather than accidental death (Table 3).
Univariate risk factors, at index presentation, for non-suicide death, accidental death and natural death, expressed as hazard ratio (95% CI)
Prescribed drugs as univariate risk factors, at index presentation, for non-suicide death, accidental death and natural death, expressed as hazard ratio (95% CI)
Multivariate analysis
The exposure variables that were statistically significant on univariate analysis, excepting individual drugs, were included in the multivariate analyses for each of the three outcome variables. For nonsuicidal death the exposure variables that contributed to the final model with increased risk, expressed as adjusted HR (95% CI), were: increasing age 1.07 (1.06–1.08) per year, male gender 1.77 (1.24–2.52), psychiatric diagnosis of substance related disorder 1.49 (1.03–2.16), prescription of one or more respiratory drug 2.69 (1.31–5.55), and prescription of one or more antidiabetic drug 1.95 (0.93–4.07), while psychiatric diagnosis of adjustment disorder 0.64 (0.38–1.05) was associated with decreased risk.
For accidental death the exposure variables that contributed to the final model with increased risk, adjusted HR (95% CI), were: male gender 3.0 (1.49–6.03), recreational overdose 1.64 (1.02–2.63), discharge to ‘other’ destination 4.94 (1.15–21.18), prescription of a selective serotonin reuptake inhibitor 2.58 (1.06–6.27), and current or lifetime drug or alcohol misuse 2.0 (0.90–4.44), while psychiatric diagnosis of ‘other conditions as a focus of clinical attention’ 0.23 (0.07–0.77) was associated with decreased risk.
For ‘natural’ cause death the exposure variables that contributed to the final model with increased risk, adjusted HR (95% CI), were: increasing age 1.10 (1.08–1.11) per year, prescription of one or more respiratory drug 3.22 (1.40–7.42), and prescription of one or more antidiabetic drug 2.06 (0.99–4.31).
Discussion
Study limitations
The main disadvantage of the methodology used in the present study is that some of the patients who died may have been missed by the matching process [16]. However, this problem is common to all studies that utilize death registries, and cohort studies in turn are often unable to track a significant proportion of patients. The advantage of the methodology of the present study is the ability to determine death and cause of death from an entire country for a cohort of patients originating in one geographical region. Patients who present with selfharm or self-poisoning may be difficult to follow up over such a long period of time and the use of data-linkage between databases overcomes the problem of losing patients to follow-up. Some of the accidental deaths, and to a lesser extent the ‘natural-cause’ deaths, may represent misclassified suicide deaths. This problem is common to all epidemiological studies of suicide as it is often difficult to demonstrate prior intent. The use of an elimination technique (backward stepwise) in the multivariate analyses may produce a pattern of risk factors that is difficult to exactly replicate in validation cohorts. The exclusion of suicide attempts by methods other than self-poisoning may have resulted in an under-representation of patients with serious suicide attempts. Hence the generalisability of the study is limited to patients presenting with self-poisoning rather than self-harm in general.
Increased mortality
The present study confirms a higher death rate from causes other than suicide in patients who present with self-poisoning. In the younger age groups this higher death rate is attributable to deaths from accident and assault, and in the older age groups the higher death rate is attributable to natural causes. Males and females are affected similarly. The increased risk of ‘natural’ cause death is different to a study of medically serious suicide attempts from New Zealand that showed no increased risk of ‘natural’ cause death [11]. This may be because of different inclusion criteria in the two studies, or the smaller sample size and the smaller number of deaths in the New Zealand study.
Accidental death
The risk factors for accidental death in the present study were male gender, drug or alcohol misuse, discharge to ‘other’ destination and the prescription of a SSRI. The first three factors were not surprising, as males are well described as having increased risk of accidental death, as are substance abusers [22–24]. In substance abusers many of the accidental deaths are caused by accidental poisoning, and are associated with polysubstance abuse [23]. Many of these accidental poisoning deaths are attributable to opiates [22]. However, there has also been reported an increase in deaths from accidental trauma associated with substance abuse [25]. Furthermore, risk of trauma death may be reduced in those patients referred to alcohol rehabilitation treatment [26]. Discharge to ‘other’ destination in our study was mostly for homeless patients. Homeless people have been demonstrated to have a greater age and sex standardized mortality than the general population [27], [28]. This includes increased mortality from suicide, natural cause and accidental injury [27].
We are not aware of any previous reports of SSRIs being implicated in increased rates of accidental death or increased rates of accidents. SSRIs have been implicated in increased rates of falls and hip fractures in the elderly [29], [30]. However, SSRIs do not appear to impair driving performance [31]. It has been postulated that there is an association between use of SSRIs and suicidal death but the evidence for such an association is contradictory [32], [33]. While it is possible that some of the accidental deaths in the present study are misclassified suicide, it is unlikely for all of them. SSRIs have been used to treat ‘impulsivity’ and may be preferentially prescribed, compared to more toxic antidepressant medications, for patients thought to be at risk for self-poisoning. Alternatively this may be a Type 1 error as a result of the number of variables examined.
‘Natural’ cause death
The risk factors for natural cause death were, unsurprisingly, medications used to treat serious medical illness and increasing age. Affective illness was associated with ‘natural’ cause death on univariate analysis, but was eliminated from the multivariate analysis. Although there are previous reports of an association between affective illness and increased mortality the literature is conflicting [34–37]. In a general population of patients with depression, the hazard ratio for death compared with patients without a diagnosis of depression, was 1.39 [34]. Depression appears to be associated with increased mortality with neoplasia and following stroke, but not following myocardial infarction [35–37]. Hence the risk may be modified by interactions between affective illness, medical illness and other comorbidity.
The increased accidental and natural cause death rates in a population of patients presenting with self-poisoning, described in the present study, may be due to an increased expression of those risk factors identified in the present study within the study population. Patients presenting with self-poisoning have increased rates of substance, including alcohol, abuse and may also have increased rates of homelessness [38]. Psychiatric illness, and possibly also medical illness, may also be expressed to a greater degree in the population of patients presenting with self-poisoning.
Conclusion
Following self-poisoning there is increased mortality from accidental causes, particularly in the younger age groups, and natural causes, particularly in the older age groups, for both males and females. This increased mortality is in addition to the established increased mortality due to suicidal deaths in the self-poisoning and parasuicidal populations. This means that in addition to the short-term interventions and treatments that are required for self-poisoning patients, it may also be necessary to develop long-term surveillance and intervention strategies that attempt to address the substantial long-term increased non-suicide mortality risk. The different pattern of increased mortality for young (accidental) and old (‘natural’) may require different intervention strategies.