
Abstract
Objective:
Common mental disorders are strong risk factors for suicide attempt. We compared common mental disorder patients with and without suicide attempt regarding health care utilization and psychiatric medication, assessed gender differences and identified how psychotropic medication of attempters is associated with subsequent rehospitalization.
Methods:
We used administrative claims data of 22,276 common mental disorder patients with inpatient care in Lower Austria between 1 January 2006 and 31 December 2011. Suicide attempters (cases, n = 615) and non-attempters (controls, n = 21,661) were compared regarding specific healthcare utilization by calculating mean differences of time-dependent contact probabilities and psychiatric medication (i.e. prescribed defined daily doses) ± 0.5 years around their suicide attempt (cases)/common mental disorder diagnosis (controls). Cluster analysis was used to group suicide attempters according to their psychiatric medication. The risk of rehospitalization 0.5–3 years after the attempt was calculated with regression analysis controlling for sex, age and morbidity-related factors.
Results:
Contacts with general practitioners were lower for attempters than non-attempters (mean difference of contact probabilities over observation period, males = −0.05, 95% confidence interval = [−0.07, −0.03]; females: mean difference = −0.04, 95% confidence interval = [−0.05, −0.03]). Regarding psychiatrists, female attempters had markedly higher contact probabilities after the attempt compared to female non-attempters (mean difference = 0.02, 95% confidence interval = [0.007, 0.04]); male attempters had lower contact probabilities before the attempt compared to male non-attempters (mean difference = −0.01, 95% confidence interval = [−0.004, −0.02]). Attempters had higher dosages of psychiatric medication across the entire period. Antidepressant and antipsychotic medication peaked at the time of common mental disorder diagnosis/attempt. Benzodiazepine prescriptions were considerably higher for male attempters than their female counterparts and were constantly elevated for male attempters across the observation period. A cluster of attempters with long-term benzodiazepine prescriptions had an increased risk of rehospitalization (adjusted odds ratio = 2.4, 95% confidence interval = [1.1, 5.5]).
Conclusion:
Despite lower contact probabilities, common mental disorder patients with suicide attempt are prescribed more psychiatric medication, particularly benzodiazepines, with an elevated risk of rehospitalization. Strong sex differences were found.
Keywords
Introduction
Common mental disorders (CMDs), including depressive and anxiety disorders, have a very high prevalence globally and in Western countries (National Institute for Health and Care Excellence, 2011; Vollebergh et al., 2001; World Health Organization, 2003). These chronic disorders result in large disease burdens in terms of disability and economic loss (Weich, 1997). They are also important risk factors for suicidal behaviour (Cavanagh et al., 2003).
Suicide attempters are a group of high relevance in mental healthcare but their behaviours and treatment patterns are not fully understood. More than 70% of suicide decedents were shown to be in contact with the healthcare system in the month before their suicides (Luoma et al., 2002), and these individuals typically saw their general practitioner (GP) rather than seeking specialized care (Chang et al., 2009; Chock et al., 2015; Pirkis and Burgess, 1998; Stark et al., 2012). However, a Finnish study showed that healthcare contacts briefly before non-fatal attempts were infrequent (Suominen et al., 2002), particularly for young attempters (Suominen et al., 2004). Furthermore, a national survey in the United States found that only 56% of adults who had a suicide attempt within the last 12 months received mental health treatment (Han et al., 2014).
Even less is known about patterns in prescribed psychiatric medication of suicide attempters with CMD diagnosis around their attempt. Due to known gender disparities in suicidal behaviour, help-seeking and mental health treatment (Manteuffel et al., 2014; Oliver et al., 2005), gender effects are extremely relevant. Male CMD patients show less help-seeking for mental health problems than women (Oliver et al., 2005). Female suicide attempters are more likely to have psychiatric consultations before their attempt as compared to male attempters (Harada et al., 2014), and females receive more psychiatric medication (Astbury, 2001). There is also a so-called gender paradox in suicidal behaviour, meaning that females typically have more non-fatal suicide attempts than males, who more frequently die from suicide (Canetto and Sakinofsky, 1998).
Patterns in healthcare contacts and pharmacological treatments received might also predict long-term prognosis such as rehospitalization. Long-term rehospitalization is an established marker of the severity of the disease or medical consequences of a suicide attempt, reflecting poor prognosis (Durbin et al., 2007). Short hospital stay length has been discussed as a predictor of early rehospitalization (Durbin et al., 2007), but a 2014 Cochrane review found no evidence that hospital stays below 28 days for severe mental disorders were linked to rehospitalization at 1 or 2 years. The review also highlighted potentially positive effects of short hospital stays on the prognosis (Babalola et al., 2014).
Information on both the timing of healthcare contacts and psychiatric treatment received by suicide attempters with a CMD diagnosis might reveal important new insight to understand their care-seeking and treatment patterns and to identify possible treatment gaps.
The aims of this study were to (1) investigate how healthcare utilization and psychiatric medication of CMD patients with suicide attempt differ from non-attempters, (2) to investigate gender differences and (3) to define how treatment clusters based on received medication in suicide attempters are related to subsequent rehospitalization for mental disorders.
Methods
We used a pseudonymized medical claims dataset from a public social insurance covering the Austrian state of Lower Austria (NÖGKK) (Klimek et al., 2015). The dataset contains 1,284,303 individuals living in Lower Austria who consulted a health care provider (HCP) between 1 January 2006 and 31 December 2011. Overall, 1,600,000 people lived in Lower Austria in 2006, most of them with universal health coverage. Insurance generally covers care by contracted physicians, and a regional health fund pays for inpatient care. Patients in the dataset can be considered as mainly rural dwellers. People who died/were born during that period were not included in the dataset.
Healthcare utilization and psychiatric medication of CMD patients with suicide attempt compared to non-attempters
Study population
The study base consisted of 22,276 patients hospitalized with CMD diagnoses (International Classification of Diseases, version 10 [ICD-10]) codes F32 (major depressive disorder, single episode), F33 (major depressive disorder, recurrent), F40–F43 (F40–F41, anxiety disorders; F42, obsessive-compulsive disorders; F43, stress- and adjustment-related disorders) as a main or side diagnosis. In Austria, data on diagnoses are only available from hospital stays; therefore, all patients in the study population were hospitalized at least once in the observation window. From the study base, 615 patients were hospitalized for suicide attempts (cases). The remaining 21,661 CMD patients had no attempt (controls). Age and sex were available for 545 attempters (88.6%) and 19,469 non-attempters (89.9%) (Figure 1). For each patient, we assessed healthcare contacts and psychiatric medication in the period from ±0.5 years around the first suicide attempt (cases) or first CMD diagnosis (controls).
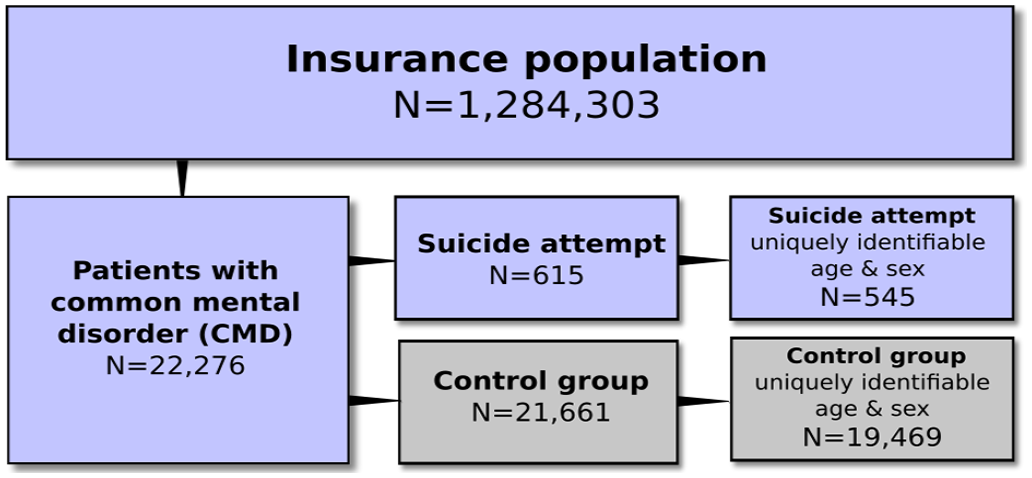
Study flowchart.
Variables
Age (range: 10–99 years) and sex (male/female) were measured at the time of suicide attempt or first CMD diagnosis for cases and controls, respectively. The occurrence of a hospital stay with specific mental comorbidities as main or side diagnosis, specifically substance dependence (ICD-10: F10–F19), schizophrenia/psychotic disorders (F20–F29), manic/bipolar disorders (F30–F31), and personality disorders (F60–F69), was also measured to characterize the patient groups. The hospital stay length for each patient was defined as the total number of days spent in a hospital (independent of specific diagnoses) during the observation window.
We focused on types of HCP that typically treat patients with CMD, namely, GPs, psychiatrists, psychotherapists, and clinical psychologists, while categorizing the rest as other HCPs. We used two different types of probabilities to describe how often patients encountered these HCPs. First, we defined the treatment probability for attempters and non-attempters, respectively, as the fraction of patients who had at least one contact with the respective HCP. Second, we considered time-dependent contact probabilities with (A) GPs and (B) psychiatrists. Contact probabilities describe the expected number of contacts of each patient with the corresponding HCP. The contact probabilities were computed as a function of time in steps of 36 days within ±0.5 years around the suicide attempt (cases) or CMD diagnosis (controls). Days during hospitalizations were excluded. Three groups of prescribed psychiatric medications according to the Anatomical Therapeutic Chemical Classification (ATC) comprised antidepressants (ATC-code N06A), antipsychotics (N05A, except Lithium), and benzodiazepines (N05BA, N05CD, N05CF, N03AE01). For 91% of dispensations, the defined daily doses (DDD), that is, an average daily maintenance dose in adults (WHO Collaborating Centre for Drug Statistics [WHOCC], 2016), was extracted. We computed the time-dependent medication exposures for cases and controls who received the respective medication. Mean medication exposure was defined as the sum of all dispensed medications (DDD) divided by the total number of days. Days during hospitalizations were excluded.
Statistics
We assessed differences in comorbid diagnoses by means of contingency tables. When comparing continuous variables between two groups, we used a two-sided t-test. Normality of the continuous data was checked with a Jarque–Bera test. For comparisons between more groups, a one-way analysis of variance (ANOVA) test was used. To test whether age of the patients in the case and control group was from the same continuous distribution, we performed a two-sample Kolmogorov–Smirnov test. Furthermore, the difference of average values of contact probabilities between cases and controls was defined as mean difference (MD). The observation period was segmented into intervals of 36 days and the MDs were measured in each interval. Significance of the mean- and time-dependent differences of contact probabilities and probabilities of medication exposures between cases/controls within a single time interval was assessed with unpooled two-proportion z-tests. MDs for the entire observation period, and for before and after the attempt, respectively, were computed as means over the respective intervals; the confidence intervals (CIs) and p-values were again obtained from two-sided t-tests.
Sensitivity analyses/robustness tests
We performed a subsampling procedure in which we removed all patients with a specific group of mental comorbidities from the cases and control group. This approach was taken to evaluate if the results were confounded by the corresponding diagnoses: if differences between cases and controls disappear after the removal of patients with a specific diagnose, differences can be attributed to the excluded comorbidity rather than the suicide attempt. If, however, the differences prevail, they cannot be explained by the confounding influence. Furthermore, we repeated the analysis (1) including only patients with CMD as a main diagnosis (11,680 CMD patients including N = 473 patients with suicide attempt) and (2) including only patients with a diagnosis of depression (ICD-10 codes F32 and F33) instead of CMD (15,152 patients with depression, N = 457 with a suicide attempt). Further tests assessed the influence of patient age and hospital stay length. Therefore, we stratified patients into younger versus older patients and shorter versus longer hospital stays based on the sample mean age and mean hospital stay length, respectively.
We performed a robustness test for an alternative definition of controls to avoid the problem that controls could be biased towards more recent diagnoses. Instead of taking the time of first occurrence of a CMD diagnosis as the ‘index diagnosis’ in the control group, we randomly selected the first or any of the following CMD diagnoses as the index diagnosis.
Finally, we changed the window of healthcare contacts and psychiatric medication in the period from ±0.5 years around the first suicide attempt (cases) or first CMD diagnosis (controls) to ±1 year to assess if findings depended on the definition of that time window.
Clusters of suicide attempters based on prescribed psychiatric medication and risk of rehospitalization
Patients with suicide attempts were grouped into clusters according to their time-dependent psychiatric medication exposures from 180 days before until 180 days after the attempt. This was to capture the heterogeneity of their temporal prescription patterns. For each type of medication (antidepressants, antipsychotics, benzodiazepines), each patient’s exposure was described by a time-series of cumulative exposures with time being measured relative to the patient’s first suicide attempt. Similarity of patients in terms of prescriptions was expressed by the cross-correlation coefficient (Pearson’s correlation) of these time-series. Each pair of patients gave a three-dimensional vector of similarities, where each component corresponded to a different type of medication. This vector was collapsed into a single number by taking its length (Euclidean norm). The clusters of mutually similar patients were extracted from the so-obtained similarity matrix using the Louvain clustering algorithm (Blondel et al., 2008), a greedy network modularity optimization procedure (Newman, 2010) that does not require a pre-specification of the retrieved number of clusters.
Each patient with suicide attempt was described by a set of independent variables that were measured in the time span around ±0.5 years of attempt. These variables included the patient’s cluster assignment based on dispensed medications (patients without medications served as reference group) and binary variables for specific HCP contacts and comorbid CMD diagnoses. For each individual with suicide attempt, we extracted the length of hospital stay directly related to the suicide attempt as a further independent variable.
Regression model
The dependent variable was a binary variable indicating whether a patient was rehospitalized due to a mental disorder (any ICD-10 F-code) in the time span between 180 days and 3 years after the attempt. Here, we included the 489 (163 males, 326 females) patients with suicide attempts before 1 January 2009, that is, where the entire span of 3 years after the attempt was covered in the data.
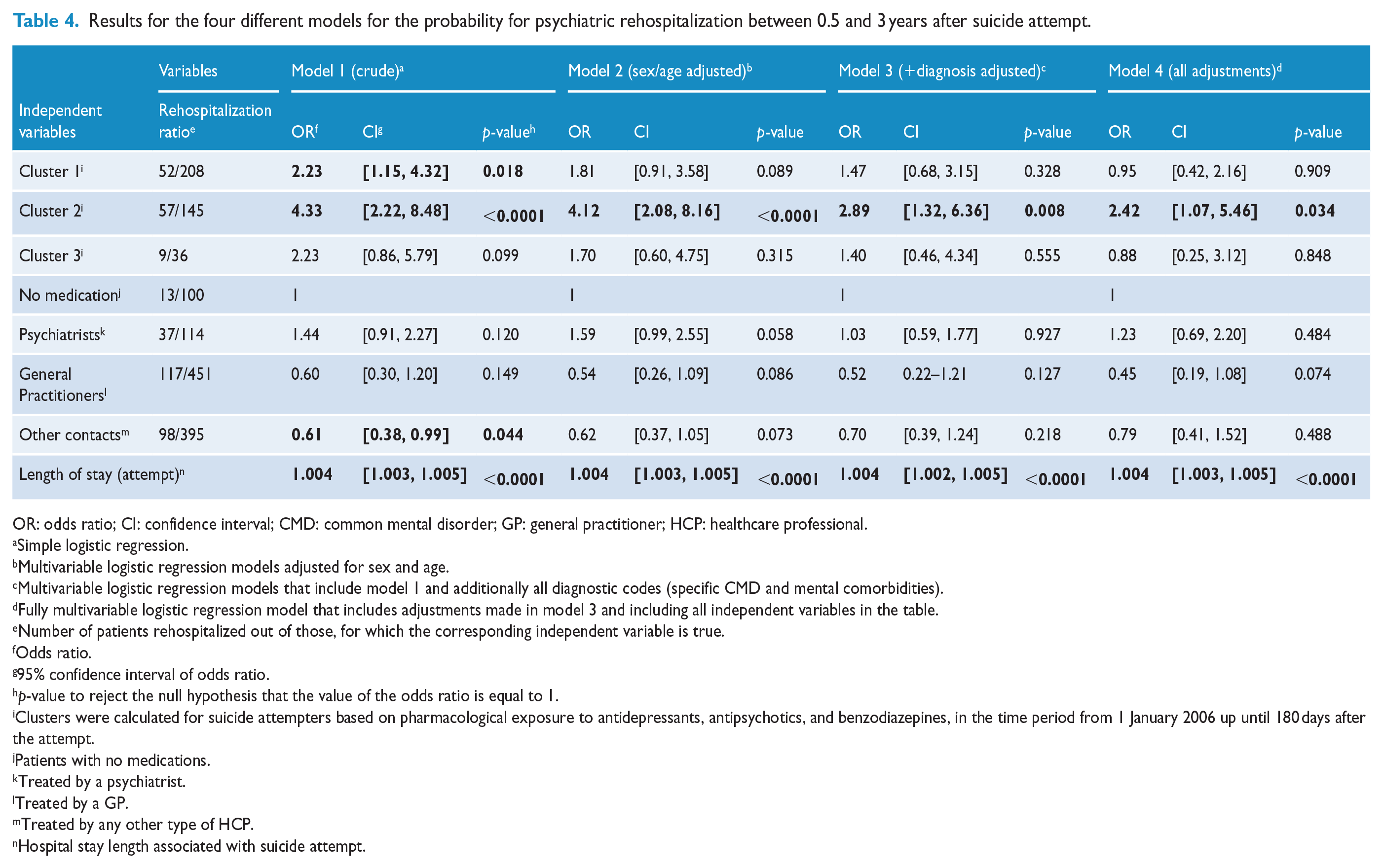
Four different logistic regression models were applied including a crude model and three adjustment steps (see Table 4 for details on adjustments made in each step).
Ethical statement
Under local regulations, the study was considered exempt from ethical approval as it involved the secondary use of an anonymous administrative research database. This was confirmed by the Medical University of Vienna’s legal department. The study was carried out in full compliance with the Declaration of Helsinki and the local applicable Good Scientific Practice.
Results
Characteristics of male and female CMD patients with suicide attempts compared to non-attempters
On average, patients with suicide attempts (cases) had 1.04 attempts (1.02 for males and 1.05 for females); 17 patients had two or more attempts. Controls had on average 1.39 CMD diagnoses, and 76% had only one CMD diagnosis. Attempters had 1.89 CMD diagnoses, with 52% having exactly one. N = 128 attempters had their first CMD diagnosis after the first attempt, 200 had the first CMD diagnosis before their attempt, and for the remaining 287 attempters the diagnoses occurred concurrently.
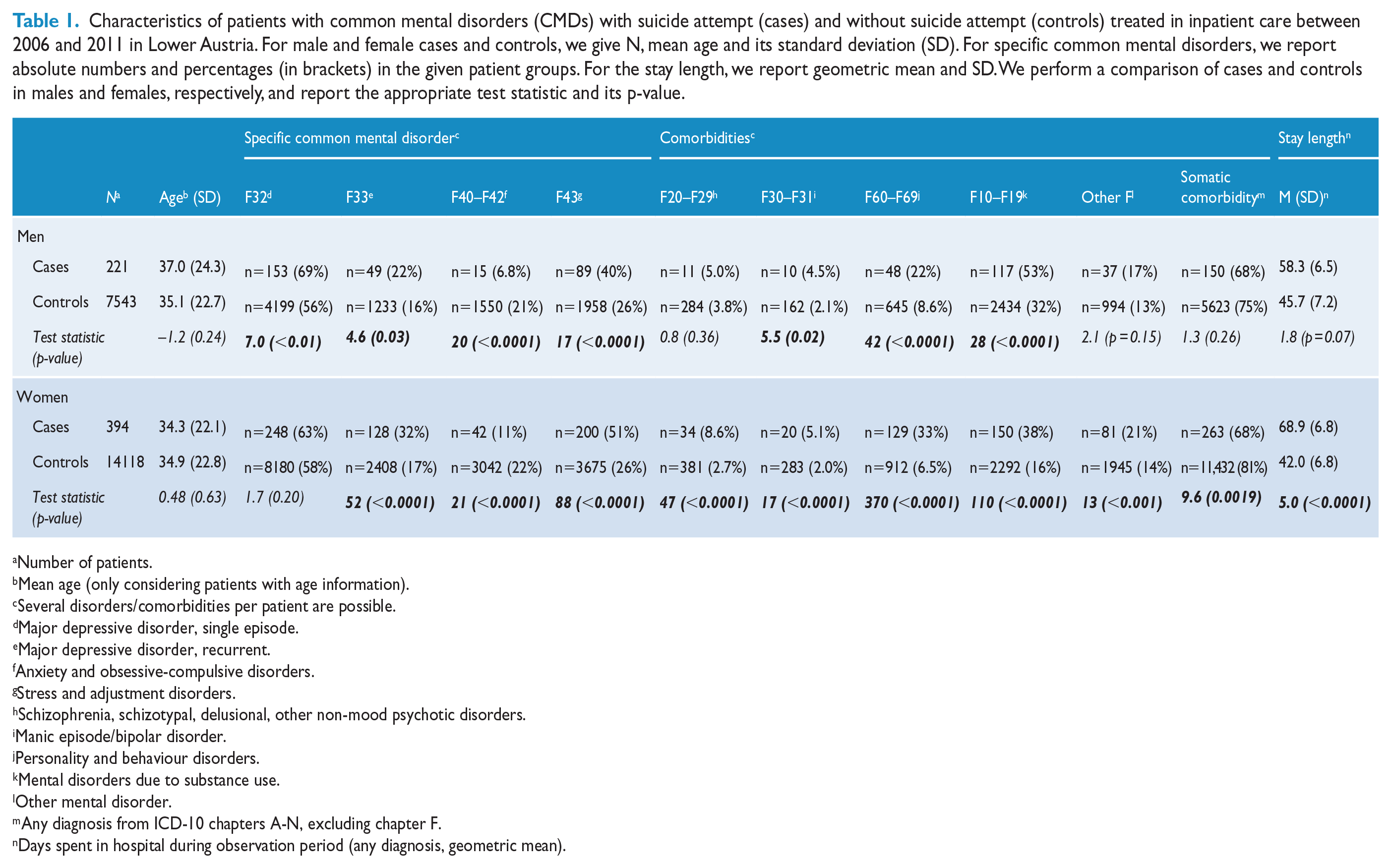
Male cases and controls had similar age distributions (p = 0.24). Compared to their male counterparts without an attempt, male attempters had more often a depressive disorder (69% vs 56% for a diagnosis of a depressive episode and 22% vs 16% for recurrent major depression), had lower proportions of anxiety disorders (7% vs 21%), and higher proportions of stress-related disorders (40% vs 26%). Male attempters were more often comorbid of other psychiatric disorders than male non-attempters, that is, with bipolar disorders (5% vs 2%), personality disorders (22% vs 9%), and with substance abuse disorders (53% vs 32%). For males, there was no difference in the length of hospital stay during the episode of diagnosis of suicide attempt (cases) and CMD diagnosis (controls) (Table 1).
Characteristics of patients with common mental disorders (CMDs) with suicide attempt (cases) and without suicide attempt (controls) treated in inpatient care between 2006 and 2011 in Lower Austria. For male and female cases and controls, we give N, mean age and its standard deviation (SD). For specific common mental disorders, we report absolute numbers and percentages (in brackets) in the given patient groups. For the stay length, we report geometric mean and SD. We perform a comparison of cases and controls in males and females, respectively, and report the appropriate test statistic and its p-value.
Number of patients.
Mean age (only considering patients with age information).
Several disorders/comorbidities per patient are possible.
Major depressive disorder, single episode.
Major depressive disorder, recurrent.
Anxiety and obsessive-compulsive disorders.
Stress and adjustment disorders.
Schizophrenia, schizotypal, delusional, other non-mood psychotic disorders.
Manic episode/bipolar disorder.
Personality and behaviour disorders.
Mental disorders due to substance use.
Other mental disorder.
Any diagnosis from ICD-10 chapters A-N, excluding chapter F.
Days spent in hospital during observation period (any diagnosis, geometric mean).
Female cases and controls showed similar age distributions. Similar differences as for males were present for female attempters compared to their female counterparts without an attempt (Table 1). Different from males, female attempters showed significantly longer hospital stays compared to their controls (Table 1).
Treatment probabilities of male and female attempters
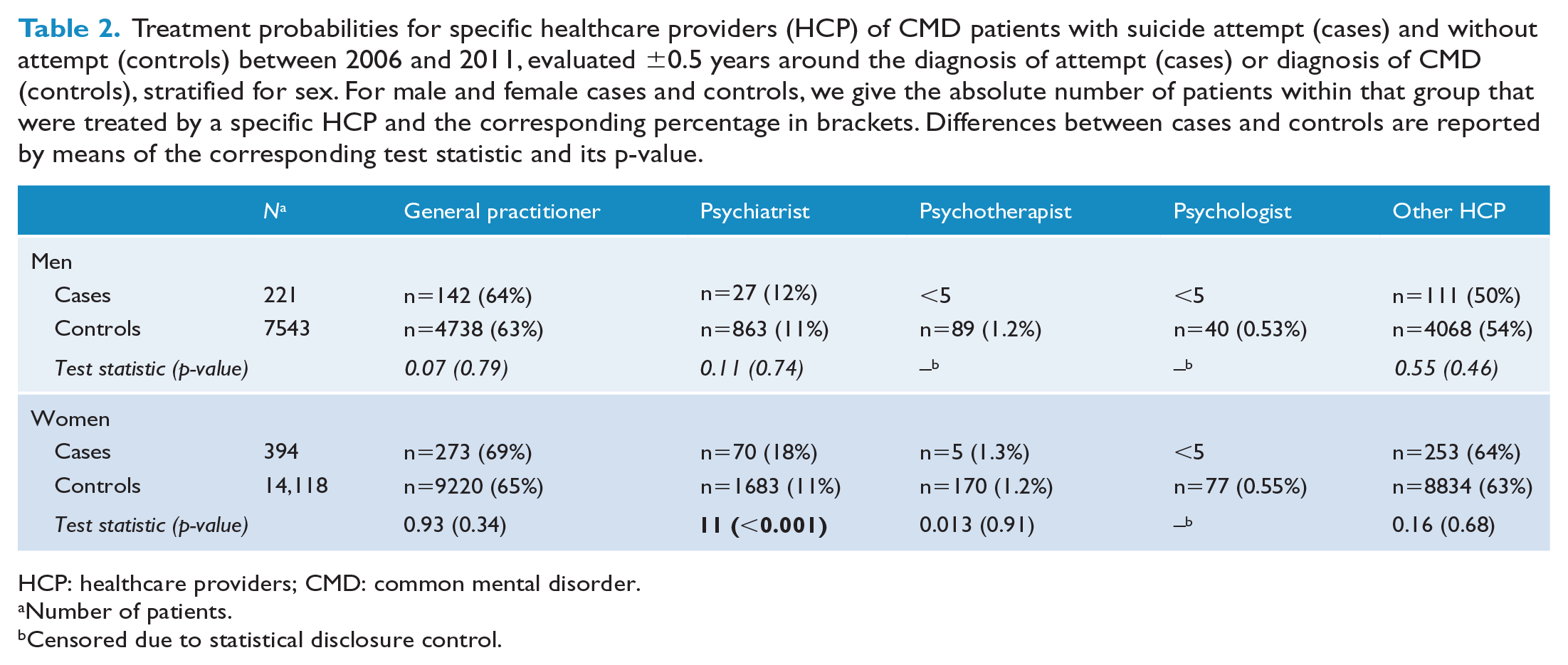
For male and female suicide attempters, seeing a GP was the most frequent type of healthcare contact (64% for males and 69% for females), followed by treatment by a psychiatrist (12% in male attempters vs 18% in female attempters). Treatment by a psychotherapist or psychologist was generally rare.
Male CMD patients with attempts did not differ from their male counterparts without an attempt in terms of the probability of seeing any type of HCP.
Female attempters had a considerably increased treatment probability by psychiatrists as compared to female non-attempters (18% vs 11%) (Table 2).
Treatment probabilities for specific healthcare providers (HCP) of CMD patients with suicide attempt (cases) and without attempt (controls) between 2006 and 2011, evaluated ±0.5 years around the diagnosis of attempt (cases) or diagnosis of CMD (controls), stratified for sex. For male and female cases and controls, we give the absolute number of patients within that group that were treated by a specific HCP and the corresponding percentage in brackets. Differences between cases and controls are reported by means of the corresponding test statistic and its p-value.
HCP: healthcare providers; CMD: common mental disorder.
Number of patients.
Censored due to statistical disclosure control.
Time-dependent contact probabilities with GPs and psychiatrists
Contact probabilities were evaluated for GPs and psychiatrists (Figure 2). Regarding GPs, the overall probabilities differed between cases/controls in males and females (m: MD = −0.051, 95% CI = [−0.072, −0.031], p < 0.0001; f: MD = −0.040, 95% CI = [−0.051, −0.028], p < 0.0001). Male and female attempters had lower contact probabilities compared to their controls; the probabilities peaked around the time of the attempt/first CMD diagnosis.
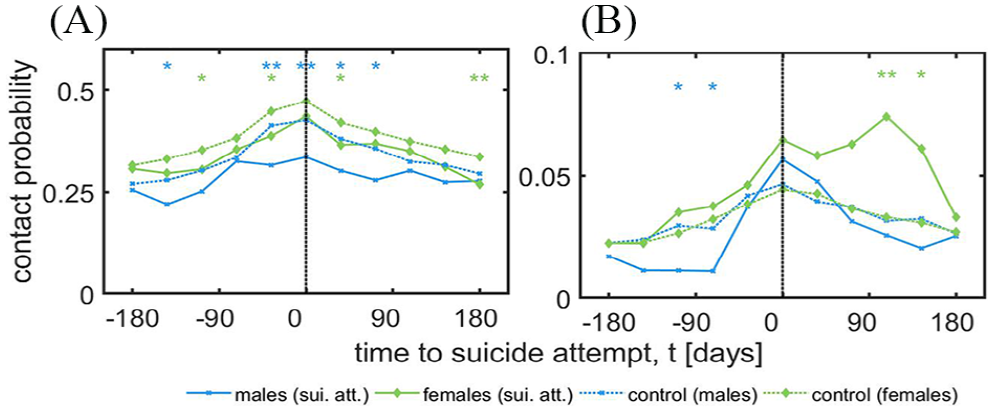
Time-dependent contact probabilities for (A) general practitioners and (B) psychiatrists for male and female suicide attempters and non-attempters.
Regarding psychiatrists, there were no overall differences in contact probabilities between male cases and controls (MD = −0.0059, 95% CI = [−0.012, 0.00028], p = 0.059), although male attempters had significantly lower contact probabilities before the attempt (MD = −0.012, 95% CI = [−0.020, −0.0037], p = 0.015). In contrast, higher contact probabilities for female cases were present (MD = 0.024, 95% CI = [0.041, 0.007], p = 0.017), peaking around 100 days after the attempt.
Psychiatric medication
Figure 3 shows a Venn diagram for the three types of dispensed medications for (A) attempters and (B) controls. Overall, frequencies of prescriptions of antipsychotics and benzodiazepines were higher in attempters than non-attempters. Measured in DDDs for each medication type, exposure was higher for attempters than non-attempters (antidepressants: MD = 0.048, 95% CI = [0.0043, 0.052], p < 0.0001 for males; and MD = 0.153, 95% CI = [0.150, 0.156], p < 0.0001 for females; antipsychotics: MD = 0.050, 95% CI = [0.0045, 0.055], p < 0.0001 for males and MD = 0.248, 95% CI = [0.244, 0.251], p < 0.0001 for females; benzodiazepines: MD = 0.31, 95% CI = [0.30, 0.32], p < 0.0001 for males and MD = 0.156, 95% CI = [0.152, 0.161], p < 0.0001 for females). The time dependence of medication exposure to (C) antidepressants and (D) antipsychotics peaked around the time of the attempt or CMD diagnosis (t = 0), with higher exposures for attempters than controls. Prescribed dosages showed a steep increase in the month before the suicide attempt/CMD diagnoses, followed by a steep decline in the subsequent month. A similar observation holds for the comparison of (E) benzodiazepines between female attempters and non-attempters. In contrast, male attempters showed constant and considerably higher exposures to benzodiazepines over the whole observation period, amounting to an up to threefold DDD compared to their male counterparts.
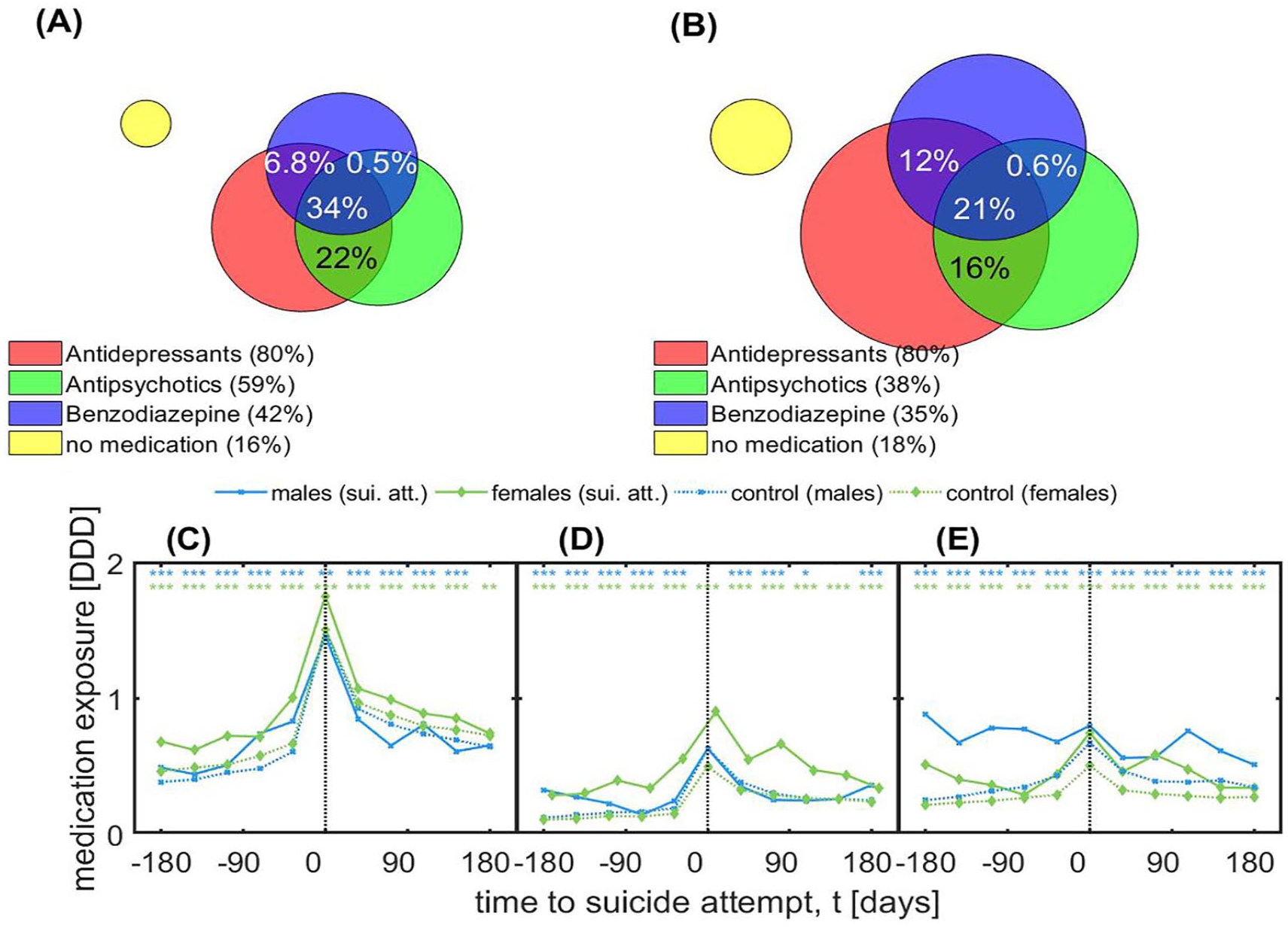
Medications for (A) attempters and (B) non-attempters using Venn diagrams, and time-dependent drug exposures measured in defined daily doses (DDD) are shown for (C) antidepressants, (D) antipsychotics and (E) benzodiazepines for males and females.
Sensitivity analyses/robustness tests
Results of the subsampling robustness tests for specific psychiatric diagnoses are shown in the supplemental information (SI), Figures S1–S3 and discussed in SI Text S1. To summarize these results, we found that most results did not change qualitatively in the different subsamples. This applied also to the robustness test assessing if a random selection of hospitalizations in the observation window (instead of the first hospitalization with CMD diagnoses) qualitatively changed the findings. Regarding the definition of time intervals, our results did not change substantially if we defined the time interval from ±0.5 years to cover a period of ±1 year around the attempt/CMD diagnosis. Exceptions from this general consistency in the robustness tests were that (1) the increased exposure to benzodiazepines in male attempters was mostly driven by younger patients and patients with a diagnosis of substance abuse (F10–F19, which includes mental and behavioural disorders due to use of sedatives or hypnotics [including benzodiazepines]) and that (2) increased contact probabilities with GPs for female attempters appeared to be confounded by diagnoses of depression (F32 and F33).
Clusters of suicide attempters based on their prescribed psychiatric medication and risk of rehospitalization
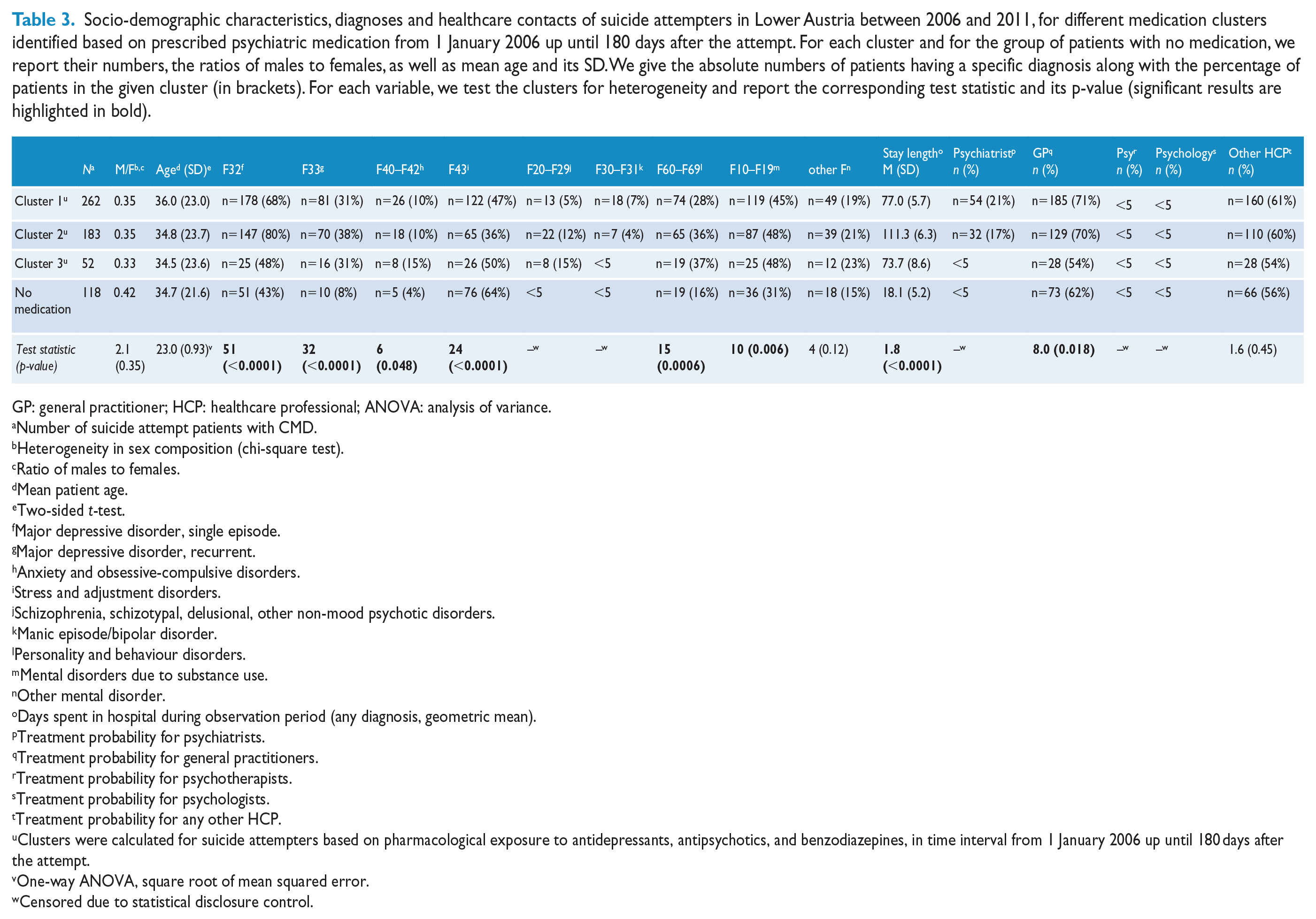
We identified three different clusters of suicide attempt patients based on their time-dependent medication exposures (Figure 4). In the following, all comparisons are made between patients in a given cluster and all patients outside of that cluster. The clusters showed significant heterogeneities in diagnoses, length of hospital stay, and their contact probabilities with GPs and psychiatrists (Table 3). There was a considerable proportion of patients who did not receive any medication (or very small amounts). These patients were more often male, typically had short hospitalizations, were least likely to see a psychiatrist after the attempt and were more often diagnosed with post-traumatic stress disorder (PTSD).
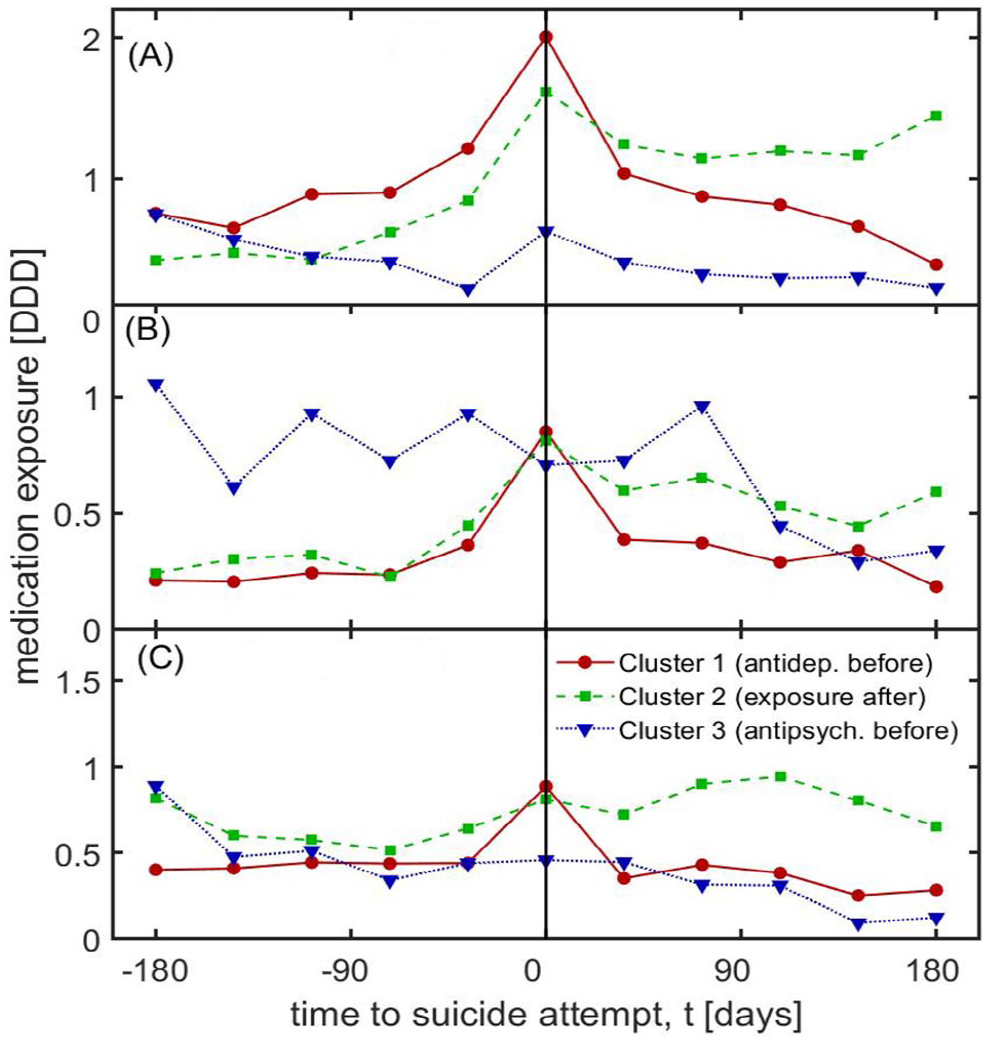
Time-dependent medication exposures in defined daily doses (DDD) for each cluster of suicide attempt patients over a time window of 0.5 years before and after the attempt.
Socio-demographic characteristics, diagnoses and healthcare contacts of suicide attempters in Lower Austria between 2006 and 2011, for different medication clusters identified based on prescribed psychiatric medication from 1 January 2006 up until 180 days after the attempt. For each cluster and for the group of patients with no medication, we report their numbers, the ratios of males to females, as well as mean age and its SD. We give the absolute numbers of patients having a specific diagnosis along with the percentage of patients in the given cluster (in brackets). For each variable, we test the clusters for heterogeneity and report the corresponding test statistic and its p-value (significant results are highlighted in bold).
GP: general practitioner; HCP: healthcare professional; ANOVA: analysis of variance.
Number of suicide attempt patients with CMD.
Heterogeneity in sex composition (chi-square test).
Ratio of males to females.
Mean patient age.
Two-sided t-test.
Major depressive disorder, single episode.
Major depressive disorder, recurrent.
Anxiety and obsessive-compulsive disorders.
Stress and adjustment disorders.
Schizophrenia, schizotypal, delusional, other non-mood psychotic disorders.
Manic episode/bipolar disorder.
Personality and behaviour disorders.
Mental disorders due to substance use.
Other mental disorder.
Days spent in hospital during observation period (any diagnosis, geometric mean).
Treatment probability for psychiatrists.
Treatment probability for general practitioners.
Treatment probability for psychotherapists.
Treatment probability for psychologists.
Treatment probability for any other HCP.
Clusters were calculated for suicide attempters based on pharmacological exposure to antidepressants, antipsychotics, and benzodiazepines, in time interval from 1 January 2006 up until 180 days after the attempt.
One-way ANOVA, square root of mean squared error.
Censored due to statistical disclosure control.
Cluster 1 comprised suicide-attempting CMD patients who received high dosages of antidepressants at the time of attempt, with concurrent peaks in antipsychotics and benzodiazepines (cluster short name ‘antidep. before’ in Figure 4). The levels declined to base level within 1 month for all substance groups. This cluster was characterized by the lowest prevalence of schizophrenia and higher levels of adjustment disorders (Table 3). Patients in this cluster were seeing GPs and psychiatrists comparably often.
In cluster 2, benzodiazepine exposure was highest. With regard to antidepressants and antipsychotics, exposure increased shortly before and remained stable in the 6 months following the attempt (‘exposure after’ in Figure 4). Patients in this cluster were comparably often seeing a GP and psychiatrist.
Cluster 3 included individuals with high levels of antipsychotic medication and low levels of antidepressants and benzodiazepines (‘antipsych. before’ in Figure 4). These patients showed only small changes in average dosages at the time of the attempt, were least likely to see their GP or psychiatrist, and included the largest proportions of patients with schizophrenia and adjustment disorders.
The results for the regression models for rehospitalizations are shown in Table 4. Length of hospital stay (odds ratio [OR] = 1.004, 95% CI = [1.003, 1.005], p < 0.0001) and assignment to cluster 2 (OR = 2.4, 95% CI = [1.1, 5.5], p = 0.034) showed a significant association with subsequent rehospitalization for mental disorders. Model 4, with all adjustments, had an adjusted generalized R2 of 0.30 and a chi-square statistic for a test against a constant model of 114 (p < 0.0001).
Results for the four different models for the probability for psychiatric rehospitalization between 0.5 and 3 years after suicide attempt.
OR: odds ratio; CI: confidence interval; CMD: common mental disorder; GP: general practitioner; HCP: healthcare professional.
Simple logistic regression.
Multivariable logistic regression models adjusted for sex and age.
Multivariable logistic regression models that include model 1 and additionally all diagnostic codes (specific CMD and mental comorbidities).
Fully multivariable logistic regression model that includes adjustments made in model 3 and including all independent variables in the table.
Number of patients rehospitalized out of those, for which the corresponding independent variable is true.
Odds ratio.
95% confidence interval of odds ratio.
p-value to reject the null hypothesis that the value of the odds ratio is equal to 1.
Clusters were calculated for suicide attempters based on pharmacological exposure to antidepressants, antipsychotics, and benzodiazepines, in the time period from 1 January 2006 up until 180 days after the attempt.
Patients with no medications.
Treated by a psychiatrist.
Treated by a GP.
Treated by any other type of HCP.
Hospital stay length associated with suicide attempt.
Discussion
This is the first study that quantified healthcare utilization and psychiatric medication received by suicide-attempting CMD patients using a comprehensive, large-scale administrative database that linked in- and outpatient data. Specific, repeated healthcare contacts with GPs were generally less common for suicide attempters than non-attempters with similar diagnoses. Only psychiatrists were more frequently seen by some suicide attempters, and this applied only to female attempters after their attempt. Despite their lower contacts with specific HCPs, as compared to non-attempters, attempters received more psychiatric medication, with a peak of antidepressant and antipsychotic prescriptions around the time of the suicide attempt. Regarding benzodiazepines, particularly male attempters had high dosages of benzodiazepines (up to three-fold dosages of their male counterparts). This pattern was present across the whole observation period, particularly in younger male attempters.
The present finding that seeing a GP was much more likely than seeing a psychiatrist around the time of suicide attempt is consistent with previous findings regarding HCP contacts before suicide (Chang et al., 2009; Chock et al., 2015; Luoma et al., 2002; Pirkis and Burgess, 1998; Schaffer et al., 2016; Stark et al., 2012). It reflects that GPs are generally the first contact for health issues but may also signal difficulties in accessing specialist care and stigmatization of mental health services.
Despite the relatively high probability of suicide attempters to see a GP around their suicide attempt, the finding that follow-up visits were much less frequent around the time of diagnoses (as indicated by lower contact probabilities) compared to non-attempting patients reveals an important addition to what is known about healthcare-seeking patterns in suicide attempters. Suicide-attempting CMD patients may have a lower inclination of seeking regular help, with reduced help-seeking particularly around their attempt (Goldsmith et al., 2002). Because suicide risk often remains undetected during healthcare contacts (Deisenhammer et al., 2007; Isometsä et al., 1995), GPs may also underestimate the necessity for follow-up appointments with these patients. Some individuals might be reluctant to seek help once their suicidal development gets worse.
For males, contact probabilities were lower for attempters before the attempt as compared to their male controls. This is concerning and might reflect that particularly suicidal male patients do not keep follow-up appointments with their psychiatrists before their suicide attempt, or their suicidality might not be sufficiently addressed during their visits. Unlike female attempters, male attempters did not get more aftercare from psychiatrists after their suicide attempt, indicating a treatment gap before and after suicide attempts for male attempters. These patterns might reflect known gender differences in help-seeking (Oliver et al., 2005). In general, contact probabilities with psychiatrists were low, and only 18% of attempting CMD patients had contact with a psychiatrist. In a Swedish and Taiwanese sample of suicide attempters, about 40% and 26%, respectively, received some sort of aftercare (Lin et al., 2014; Runeson et al., 2000). Divergences may result from differences in samples, time windows, healthcare systems, and differences in the definition of aftercare.
Treatments by psychologists and psychotherapists, which are considered to be very relevant for state-of-the-art prevention and aftercare (Carrigan and Lynch, 2003), were even more infrequent. At least part of this finding appears to be due to unmet help-seeking behaviours, which has been reflected in long waiting lists for prescribed psychotherapy in Austria (OECD, 2015).
Robustness analyses indicated that female but not male under-representation of attempters in GP contacts was explainable by their higher prevalence of single-episode major depression (F32) as compared to female non-attempters (i.e. difference in contact probabilities for females became non-significant once these patients were removed). This finding indicates that female cases and controls without depression had similar contact probabilities with GPs, whereas male cases visited their GPs less often independent of comorbid depression. In contrast, the over-representation of female attempters seeing a psychiatrist after the attempt was explainable by a diagnosis of recurrent major depression, indicating that particularly females with recurrent depression received more aftercare from psychiatrists. In total, this finding gives a mixed picture regarding the treatment of female depression: female suicide attempters with a single-episode diagnosis of depression do not seem to see their GPs as frequently as other female attempters (with respect to their controls), which might be due to the perceived lower necessity for frequent follow-ups than for other female attempters, or due to an inclination of these patients not to seek follow-up treatments. On the other hand, female attempters with recurrent depression appear to get more aftercare from psychiatrists as compared to other female attempters, which might suggest that this patient group is more prone to seeking and/or receiving referral to specialist aftercare.
The lower probability of healthcare contacts in suicide attempters was not reflected in lower psychiatric medication in this group. Antidepressant prescriptions (DDDs) typically showed a steep increase in the month before the attempt and CMD diagnosis, followed by a quick decline. Suicide attempters received higher dosages compared to non-attempters. According to the World Health Organization (WHO) definition, antidepressant treatment in adults with depressive disorders should normally not be stopped before 9–12 months after recovery (WHO, 2012). The decline in DDDs therefore appeared relatively quick and might reflect non-compliance with treatment recommendations, a lowering of dosage or an early stop of treatment. The higher dosages obtained by females compared to males is consistent with gender differences in psychiatric prescription patterns (Regitz-Zagrosek, 2012; WHO, 2002). Regarding antipsychotics, time and gender patterns were similar to those seen for antidepressants. The observed decline within a month after the attempt also appeared quick as compared with current treatment recommendations (Rothschild and Duval, 2003).
Suicide attempters received considerably more benzodiazepines than non-attempters. Male attempters had the overall highest dosage. Their average dosage remained fairly stable in the months before and following the suicide attempt. Robustness analyses indicated that this was only true for younger male patients, whereas patients with age above the sample mean experienced a reduction of benzodiazepine prescriptions after their suicide attempt. Ongoing use of benzodiazepines has been linked to a high risk of abuse (Huerta et al., 2016) and to an increased overall mortality, mortality from cardiovascular disease, and suicide, even at moderate levels (Tiihonen et al., 2016). Furthermore, a dose–response relationship between the risk of recurrent overdosing and benzodiazepine prescriptions after the first overdose was found in a Japanese study (Okumura and Nishi, 2017). For suicide attempters, German depression treatment guidelines on post-suicidal crisis intervention recommend benzodiazepine use for no longer than 14 days after the attempt (Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde [DGPPN], 2009). The observed higher dosages for males compared to females is different from earlier studies in non-CMD specific samples (Huerta et al., 2016; Regitz-Zagrosek, 2012) and may reflect a higher symptom severity of anxiety in male patients (Chang et al., 2009; WHO, 2002). It is concerning that male attempters were often comorbid with drug abuse and stress/adjustment disorders, whereas the proportion of anxiety disorders was low in attempters compared to non-attempters, who had considerably lower dosages of benzodiazepines. Particularly substance abusers often misuse benzodiazepines (Shaw et al., 1994), and benzodiazepines are relatively contraindicated for patients with PTSD or recent trauma (Guina et al., 2015). As indicated in the robustness analysis, an important part of this over-treatment with benzodiazepines in male attempters was explainable by the over-representation of substance abuse diagnoses in this group.
This concern was also aggravated by the finding that assignment to the cluster with a sustained boost in all medication types after the attempt including consistent high benzodiazepine exposure was related to a poor prognosis, as indicated by an increased risk of subsequent rehospitalization for a psychiatric diagnosis. This cluster typically included patients comorbid with drug abuse problems and stress/adjustment disorders, raising questions about a potential over-treatment with this substance (Guina et al., 2015; Shaw et al., 1994). Continuing benzodiazepine usage in the months before and after a suicide attempt, as well as longer hospital stays for suicide attempt, can be seen as a marker for rehospitalization. A previous Cochrane review (Babalola et al., 2014) accordingly noted some possible benefits of shorter hospital stays on prognosis in terms of rehospitalizations at 1 or 2 years. The present findings support the notion that longer hospital stays may signal greater medical severity and/or lower long-term functioning (Hodgson et al., 2001).
Strengths and limitations
Strengths of this study include its focus on all individuals with inpatient treatment for CMDs in an entire federal state. Due to the use of big claims data, selection bias, which often occurs in clinical settings, is less likely (Hripcsak and Albers, 2013). There are also limitations. No socio-demographic indicators including education, marital or employment status were available. No information on reasons for contacts with GPs or specialist physicians was available. Data on suicide attempts not resulting in hospitalization were not available. Therefore, the findings only apply to more severe cases of suicide attempts (Krug et al., 2002). Further, no information on healthcare contacts privately paid for was available.
Diagnoses derived from claims data typically agree well with patient chart data, although comorbidities tend to be under-reported (Quan et al., 2002). The database used has not been evaluated comprehensively; however, the number of patients receiving antidepressant medications in the dataset compared well with findings from the representative Austrian health survey (Statistik Austria, 2007). It was not possible to control for suicide attempts that occurred before the follow-up period. CMD diagnoses may have occurred at any point during follow-up, introducing some reverse causality bias. CMD-related symptoms, however, often occur long before diagnoses (Ghio et al., 2015). Suicide attempters and non-attempters had a different distribution of specific CMD diagnoses, and attempters were more frequently comorbid of other psychiatric disorders. In a robustness analysis, we removed patients with specific psychiatric comorbidities. For most of these tests, the findings remained qualitatively the same. A further limitation was the heterogeneity of patients in terms of their specific CMD diagnoses, as well as the inclusion of CMD main and side diagnoses. Related sensitivity analyses did not qualitatively change the identified associations. Finally, suicide attempters might have had more time to accumulate illnesses or treatments as compared to controls, who were defined based on their first CMD diagnosis in the observation window. A related robustness test indicated that the present findings remained qualitatively the same when the observation period for the control group centred on a randomly chosen CMD diagnosis.
Conclusion
Suicide-attempting CMD patients seek healthcare contacts less frequently before their attempt than CMD patients without attempt. Contact with a psychiatrist is not a reality for most patients and particularly low for male attempters. In spite of having lower contact probabilities with HCPs, suicide attempters generally have higher dosages of psychiatric prescriptions around their attempt. Constant high levels of benzodiazepine prescriptions in younger male attempters warrant further investigation regarding possible over-treatment with this substance class and were associated with subsequent rehospitalization. The present findings highlight the need of gatekeeper trainings of GPs and other mental health professionals to improve assessment and follow-up with suicidal patients and improved accessibility of psychological counselling and psychotherapy (World Health Organization, 2014).
Supplemental Material
Text_S1 – Supplemental material for Healthcare utilization, psychiatric medication and risk of rehospitalization in suicide-attempting patients with common mental disorders
Supplemental material, Text_S1 for Healthcare utilization, psychiatric medication and risk of rehospitalization in suicide-attempting patients with common mental disorders by Thomas Niederkrotenthaler, Ellenor Mittendorfer-Rutz, Stefan Thurner, Gottfried Endel and Peter Klimek in Australian & New Zealand Journal of Psychiatry
Footnotes
Author Contributions
P.K., T.N., E.M.-R. and S.T. designed the study; G.E. provided data; P.K. performed the statistical analysis; T.N. and P.K. drafted the manuscript. All authors revised the manuscript critically regarding important intellectual content and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was funded by a grant from the Vienna Science and Technology Fund, grant number WWTF MA16-045, ‘Optimal gender-specific treatment paths on healthcare multiplex networks’, awarded to P.K. The funder did not have any influence on the design of the study and collection, analysis and interpretation of data and in writing the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.