
Abstract
Objective:
Mental health service use by individuals without a diagnosed mental disorder is sometimes termed ‘met un-need’. However, provision of services for this group may be necessary to provide appropriate assessment, referral and early intervention. This study quantified child and adolescent use of, and perceived need for, mental health services to inform population-level service planning.
Methods:
Young people in Australia’s Young Minds Matter survey (n = 5837, 5–17 years), were categorised into four ‘need’ groups: (1) 12-month mental disorder diagnosis; (2) remitted for more than 12 months (or experiencing a condition not surveyed); (3) 12-month subthreshold mental health problem; and (4) no indication of need for help (i.e. did not meet the requirements of the first three categories). Service demand (use of, or perceived need for, a mental health service) and number of sessions received were estimated for each, separately for children (5–11 years) and adolescents (12–17 years).
Results:
Some 20.1% (95% CI: [18.6, 21.7]) of children and 32.3% (95% CI: [30.5, 34.2]) of adolescents expressed a demand for mental health services in the past year. Service demand decreased across the need groups. Perceived need without service use was higher among those with a 12-month subthreshold mental health problem (13.8/20.2%) than those who had experienced a mental health problem that had remitted for more than 12 months (or were experiencing a condition not surveyed) (9.3/12.6%). In addition, 23.6% of children and 24.6% of adolescents with a demand for mental health services were classified as experiencing no indication of need for help.
Conclusions:
This study quantified the number of children and adolescents in Australia who are likely to require mental health services. Findings suggest that not everyone in this group who has an expressed service demand meets diagnostic thresholds, but among those who do, service demand is higher.
Introduction
Epidemiological surveys suggest that only a proportion of people with a diagnosed mental disorder receive help, while some services are used by people who do not have a diagnosed mental disorder. Some have interpreted the latter as over-servicing, labelling the treatment of persons without a mental disorder as ‘met un-need’ (Andrews, 2000; Jorm, 2006). Others, however, suggest that ‘met un-need’ is overestimated as there are other indicators of need that may lead to service use aside from a diagnosis (Alonso et al., 2007; Druss et al., 2007; Sareen et al., 2005). Indeed, the spectrum of mental health interventions proposed by Mrazek and Haggerty (1994) highlights the need for services for persons who also experience either (1) symptoms of mental illness that do not meet diagnostic thresholds or (2) a lifetime but not a 12-month mental disorder diagnosis. This is important as waiting for symptoms to progress to a diagnosis before accessing care may contribute to high prevalence rates of mental illness. In addition, a lack of services for persons with a lifetime mental disorder may result in relapses that require more intensive treatment and resourcing (Bobevski et al., 2017). Thus, while evidence-based mental health service planning is generally informed by estimates of service demand (i.e. the use of, and perceived need for, care; Harris et al., 2014) for populations with diagnosed mental disorders, there is support for quantifying service demand across a spectrum of ‘need groups’ to meet population-level service needs.
In Australia, the National Mental Health Service Planning Framework (NMHSPF) is a needs-based mental health service planning model that was developed with input from over 250 experts across Australia with clinical, operational, lived experience and/or academic expertise in the area of mental health (The University of Queensland, 2019). It provides mental health service resource estimates for optimal service delivery and is a recommended tool for supporting integrated, regional mental health service planning. To date, the NMHSPF has not produced optimal service resource estimates for children and adolescents who have remitted for more than 12 months but may require, for example, ongoing review and management. In addition, the resource estimates produced for young people with symptoms that do not meet diagnostic thresholds relied on population need data that is over 20 years old (Sawyer et al., 2001). There was therefore a need to quantify these need groups, and their associated levels of service demand, using up-to-date information.
Previous studies have quantified service demand across a spectrum of need groups among young people in Australia. The second iteration of Australia’s Child and Adolescent Survey of Mental Health and Wellbeing (2013–2014) found that, of young people (4–17 years) who used a mental health service in the last 12 months, 50% had a 12-month mental disorder diagnosis, 40% were subthreshold for a disorder diagnosis or experienced some other indicator of need (i.e. an ‘abnormal’ score on the Strengths and Difficulties Questionnaire, a ‘very high’ distress score on the Kessler 10 Scale Psychological Distress Scale, and/or lifetime suicide attempt) and 10% had no diagnosis nor elevated symptoms of mental illness or psychological distress suggesting no indication of need (Johnson et al., 2016). Using the same data (Johnson et al., 2018), it was found that one-fifth of parents/carers of young people with a mental disorder diagnosis did not identify a need for help for their child; another one-fifth identified a need but did not seek help. A more recent analysis (Schnyder et al., 2020) also found that, of young people (13–17 years) with self- or parent-reported emotional or behavioural problems, 46.5% indicated a perceived need for help, but needs were only fully met in one-third of cases.
Despite these findings, there remain gaps in our understanding of service demand among young people. In Australia, use of, and perceived need for, mental health services in this group have not been examined concurrently. A concurrent analysis of these concepts would provide a more complete picture of service demand and may increase our understanding of barriers to service use. In addition, research suggests that demand for school-based services for children and adolescents, although not part of the mental health system, should also be quantified as schools are often the gatekeepers to further specialised care (Johnson et al., 2016).
There also remain research gaps in self-reported demand for mental health services in this group. The inclusion of this concept of self-reported demand is important due to increased individuation through adolescence which may result in service demand without the parent’s knowledge. Research does suggest that levels of agreement between adolescents and parents on perceived need for mental health care are low (Schnyder et al., 2020).
In addition, there has been no prior research that has estimated service demand for a ‘relapse prevention’ group, separate to an ‘indicated prevention’ group, in Australia’s young people. It is important to quantify demand separately across well-defined need groups as each group requires different care approaches (Bobevski et al., 2017). Similarly, there has been no separate analysis of service demand, across a spectrum of need groups, for primary school-aged children (i.e. 5–11 year olds) versus adolescents (i.e. 12–17 year olds), despite the differences in mental health care required for these two age groups.
The current study aims to fill these gaps by quantifying demand for mental health services across a spectrum of four need groups (i.e. 12-month mental disorder diagnosis, relapse prevention, indicated prevention and no indication of need) separately for Australia’s children (5–11 years) and adolescents (12–17 years). Indicated prevention and relapse prevention estimates can inform estimates of national population mental health service need, such as in the NMHSPF, to support population-level mental health service planning.
Methods
Sampling participants
The study used data from Young Minds Matter: the second Australian Child and Adolescent Survey of Mental Health and Wellbeing (2013–2014). The survey methodology is described elsewhere (Hafekost et al., 2015). Briefly, a multi-stage, area-based sample selection procedure was employed: geographic areas were selected; households were then randomly selected; young people (4–17 years) within those households were then identified. Where there was more than one young person in a family, one was selected at random. Families of children aged 16–17 years were oversampled due to the high-risk nature of this group. Data were collected via face-to-face interviews with the primary carer of each selected young person; young people aged 11–17 years also completed a self-report questionnaire on a tablet. The survey collected information from 6310 families and 2967 young people (aged 11–17 years); the household response rate was 55%. A comparison of the survey sample with 2011 Census data found that it was broadly representative of the Australian population in terms of key demographic characteristics. However, a higher proportion of young people aged 4–7 years (34.1% vs 28.8%), and a lower proportion of families with only one eligible child (37.7% vs 45.8%), were included in the survey sample than expected. This was adjusted for by weighting the survey data. The current analysis was approved by the Office of Research Ethics at The University of Queensland.
Measures
Sociodemographic characteristics
The survey asked about a range of sociodemographic characteristics. For the purposes of the current analysis, only the young person’s age and sex were of interest. The age variable was aggregated, and young people were categorised into one of two age groups: 5–11 years and 12–17 years.
Hierarchical classification of need
Young people were categorised into one of four need groups based on responses to questions pertaining to the experience of mental disorder diagnosis, symptoms and associated impairment. These groups were as follows: (1) 12-month mental disorder diagnosis; (2) remitted for more than 12 months (or experiencing a condition not surveyed); (3) 12-month subthreshold mental health problem; and (4) no indication of need for help (i.e. young people who did not meet the requirements of the first three categories). This terminology was chosen for convenience and it is acknowledged that not all young people in each need group would fit the group’s description (Figure 1).
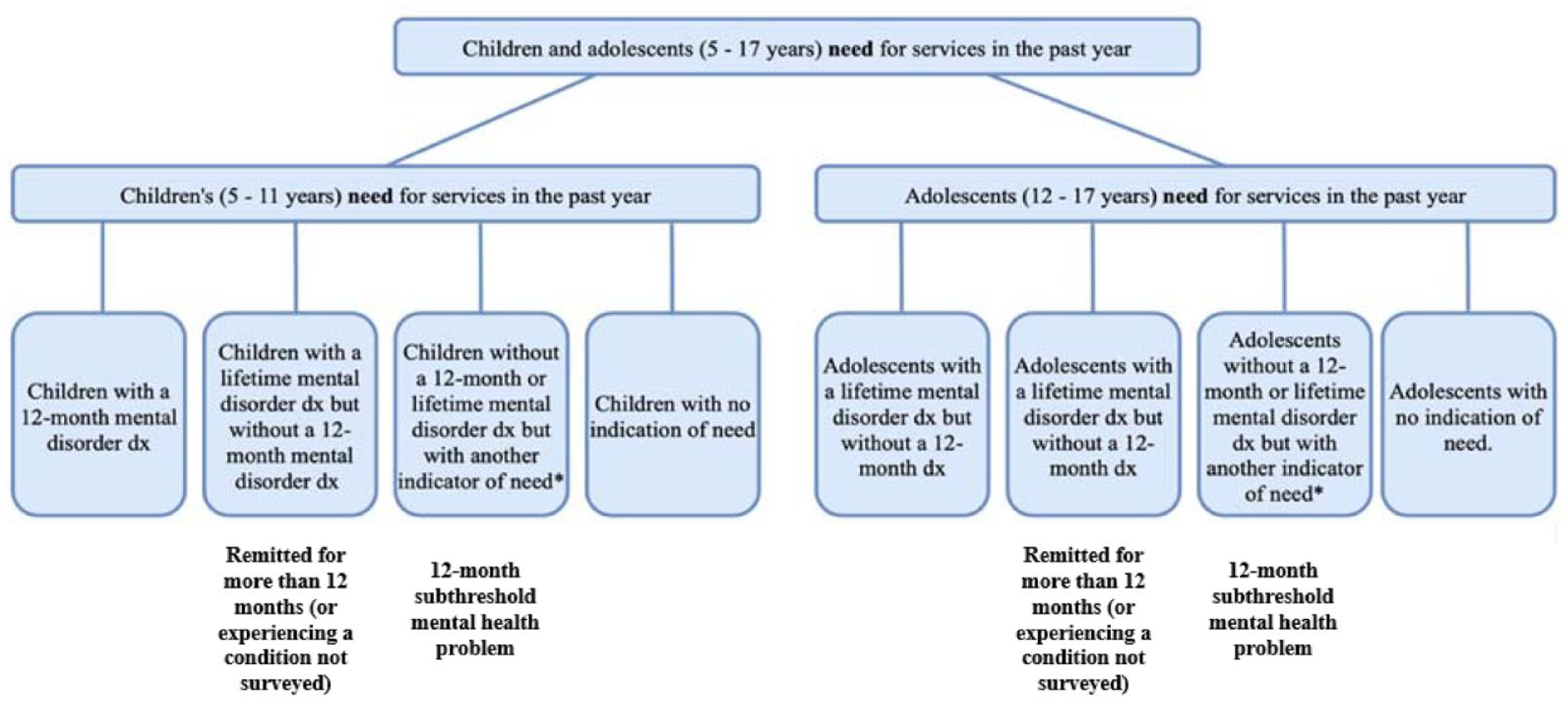
Child and adolescent need groups.
12-month mental disorder diagnosis
Presence of 12-month mental disorder diagnosis was determined using the parent-report Diagnostic Interview Schedule for Children – version 4 (DISC-IV; Fisher et al., 1993). The survey included seven DISC-IV modules – social phobia, separation anxiety disorder, generalised anxiety disorder, obsessive compulsive disorder, major depressive disorder (MDD), attention-deficit/hyperactivity disorder and conduct disorder. The oppositional defiant disorder module was also included; however, it was not possible to operationalise the criterion that ‘problem behaviours occur more frequently than expected based on age and developmental stage’, which requires clinical judgement. Young people who met all other diagnostic criteria for oppositional defiant disorder were therefore referred to as having oppositional problem behaviours. The self-report DISC-IV module for MDD was also completed by young people aged 11–17 years. The other self-report DISC-IV modules were not included in the self-report youth survey to reduce costs and minimise participant burden. The MDD module was chosen as MDD has the highest burden of illness and differences in reported symptoms between young people and their parents are most evident in the context of depression/depressive symptoms (Hafekost et al., 2015).
The DISC-IV implements the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) diagnostic criteria, which specifies that clear evidence of significant impairment in social, academic or occupational functioning is required for diagnosis. There are four different DISC-IV algorithms for assessing impairment; algorithm D was used given its previous use in Australian (Sawyer et al., 2001) and international surveys (Merikangas et al., 2010). Young people were classified as having a 12-month mental disorder diagnosis if it was reported that they met all relevant symptom criteria and experienced severe impairment in one or more of the functional domains, or at least moderate impairment in two or more functional domains, as per the algorithm.
Remitted for 12 months (or experiencing a condition not surveyed)
In the absence of a standardised assessment approach for assessing lifetime disorder diagnosis among young people, the experience of a previous diagnosis that had remitted for more than 12 months was measured by parent responses to the question ‘have you ever been told by a doctor or health professional that your child has: separation anxiety; obsessive compulsive disorder; post-traumatic stress disorder; any phobia; any other anxiety disorder; an eating disorder (e.g. anorexia, bulimia), depression, schizophrenia, psychosis, attention deficit disorder, oppositional defiant disorder, conduct disorder, autism (all forms including Asperger’s); intellectual disability; and/or Down syndrome’. Autism, intellectual disability and Down’s syndrome were excluded from the analysis as they are not the sole responsibility of the Australian mental health system. That is, these disorders are not indicative of ongoing need for mental health services but rather disability services. Nonetheless, it is noted that some young people with these disorders may have dual diagnoses and/or require, for example, review and ongoing management and/or care coordination and liaison, facilitated by the mental health system. Young people were classified as experiencing a mental disorder diagnosis that had remitted more than 12 months if they did not have a 12-month diagnosis as per the DISC-IV but their parents reported that they had previously been told that their child had a mental disorder diagnosis. Using this data, a binary lifetime mental disorder diagnosis variable was created (i.e. ‘yes’ and ‘no’). Because the DISC-IV modules did not measure the presence of all potential 12-month mental disorder diagnoses, this grouping was called ‘remitted for 12 months (or experiencing a condition not surveyed)’.
12-month subthreshold mental health problem
The DISC-IV was also used to determine the number of young people who experienced what we defined as a 12-month subthreshold mental health problem. This was defined as the experience of the required number of symptoms for a DSM-IV disorder, as per the seven parent-reported DISC-IV modules and the self-report MDD module, without the experience of clinically significant impairment and/or the experience of less than the required number of symptoms for a DSM-IV disorder (i.e. at least half but less than that required for diagnosis) with impairment (i.e. mild, moderate or severe); impairment was again defined using the DISC-IV algorithm D.
No indication of need for help
Remaining young people who did not meet the requirements of the first three categories were classified as never meeting the criteria for a 12-month subthreshold mental health problem or 12-month mental disorder diagnosis (i.e. ‘no indication of need for help’).
Health service demand
To understand service demand, we quantified three separate groups: mental health service use, perceived need and their aggregate (i.e. demand). In-scope services included mental health services and school-based mental health services. Survey questions related to service demand were completed by all parents but only a proportion of young people (13–17 years).
Mental health service use
Parents, and young people aged 13–17 years, answered questions about the use of mental health services to address emotional or behavioural problems in the past year. They were told that these problems ‘could mean a number of things, for example, being anxious or stressed, feeling depressed, having problems concentrating, being aggressive or hyperactive’. Both parents and adolescents were asked whether the young person had (1) consulted with a health professional (i.e. general practitioner, paediatrician, psychiatrist, psychologist, nurse, social worker, occupational therapist, counsellor/family therapist, other or unsure about what their profession was); (2) received help from a hospital emergency, outpatient and/or inpatient service; and/or (3) received help from a specialist child and adolescent mental health service, i.e. Child and Adolescent Mental Health Service/Child and Youth Mental Health Service, headspace (a widely available Australian specialist holistic youth service providing primary mental and physical health care and employment support) or another child and youth health service. The data was combined to create a composite, binary ‘mental health service use’ variable (i.e. ‘yes’ and ‘no’).
School-based service use
Parents, and young people aged 13–17 years, also answered questions about the use of school-based services to address emotional or behavioural problems in the past year; these included the following: (1) receiving a referral/engaging in individual and/or group counselling at school; (2) being placed in a special class; (3) making a visit to a school nurse; and (4) using ‘other’ school-based services. The data on these variables was combined to create a composite, binary ‘school-based service use’ variable (i.e. ‘yes’ or ‘no’).
Perceived need
Parents, and adolescents aged 13–17 years, answered questions about perceived need for four ‘types of help’ in the past year – information, medication, counselling and life-skills courses. For the current study, perceived need was defined conservatively as need for medication or counselling as the scope of the research was to determine perceived need for mental health care. A binary ‘perceived need’ variable was created (i.e. ‘yes’ or ‘no’). Young people who had either (1) not accessed a mental health service but perceived a need for care or (2) had not accessed a mental health service but had accessed a school-based service and reported a need for further care, were classified as having a perceived need for mental health care.
Any demand
Demand for mental health services was defined as the aggregate of the following: (1) used a mental health service; (2) did not use a mental health service but perceived a need for help or did not use a mental health service but did use a school-based service and perceived a need for further help; and (3) did not use either service but perceived a need for help. A binary ‘any demand’ variable was created (i.e. ‘yes’ or ‘no’) based on this aggregation (Figure 2).
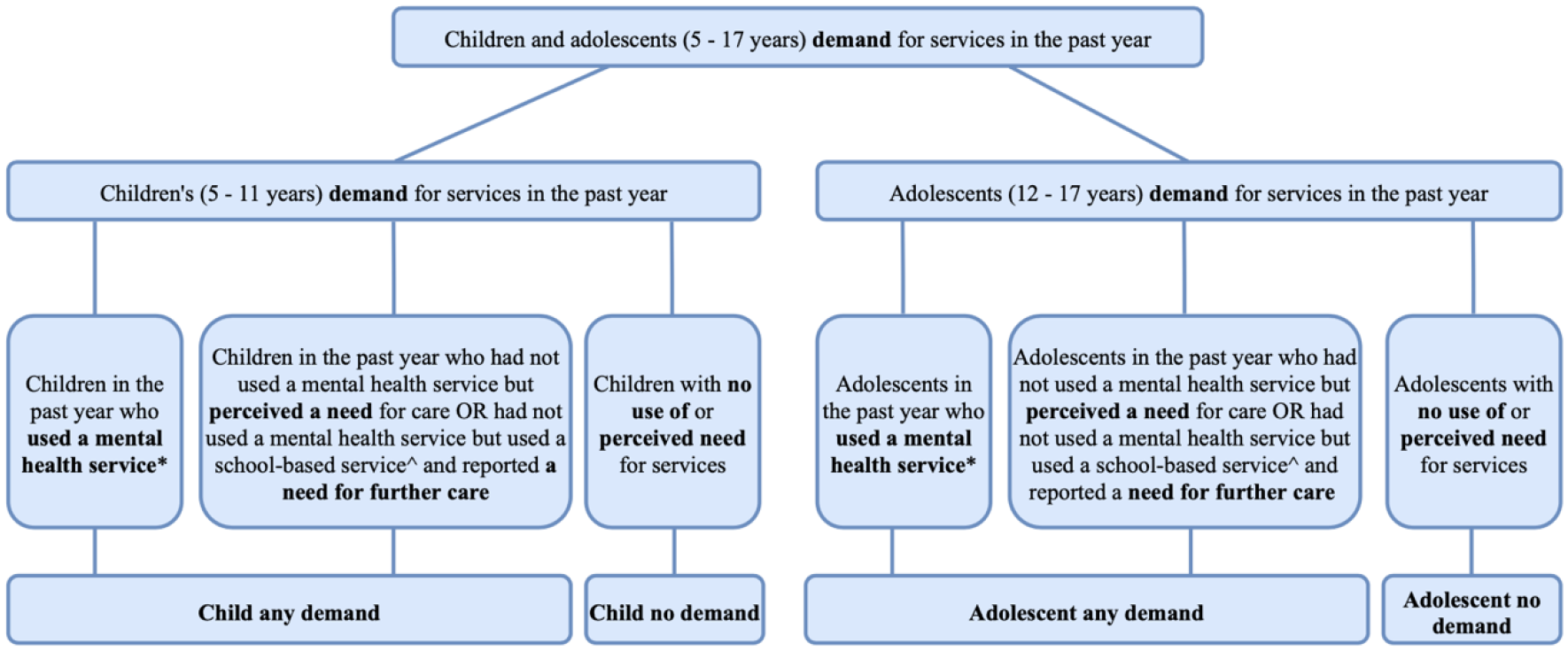
Child and adolescent demand groups.
Sessions of care received
Parents of young people who used a service for emotional or behavioural problems in the past year were also asked about how many times their child had seen each professional that they had previously reported consulting; responses were categorised as follows: once, 2–4 times, 5–9 times, 10 or more times, refuse to answer and ‘don’t know’. Individual variables pertaining to each professional seen were combined into a composite ‘sessions of care’ variable based on the highest number of sessions received from any one professional.
Data analysis
There were no missing data on the measures used in the current analysis. Data were weighted to ensure representativeness of the Australian child and adolescent population. Weights were calculated using the generalised ranking procedure of Deville and Sarndal (1992). Weighting accounts for patterns of non-response, specifically the over-representation of younger children and families with more than one child aged 4–17 years, and the oversampling of 16–17 year olds. Analyses were conducted using STATA 13 software (StataCorp, 2013). Estimates and 95% confidence intervals were calculated using the Jackknife method of estimation (Wolter, 2007). Survey weighted cross-tabulations were produced to determine prevalence rates, rates of health service use, perceived need for care and ‘any demand’ for each need group by age group. For each age group, a cross tabulation of need groups and sessions of care was also conducted to determine the proportion of young people in each need group who received each ‘level’ of sessions of care. In addition, we conducted a cross tabulation of service demand by need group for each age group and sex.
Results
5–11 year olds
The left-hand panel of Table 1 shows the population prevalence for each need group for children aged 5–11 years. Overall, 14.4% of 5–11 year olds experienced a 12-month mental disorder diagnosis, a further 5.2% had experienced a mental disorder diagnosis that had remitted for more than 12 months (or were experiencing a condition not surveyed), 9.8% experienced a 12-month subthreshold mental health problem and 70.7% did not meet the criteria for a 12-month subthreshold mental health problem and had never met the threshold for a mental disorder diagnosis (12-month or otherwise) (i.e. no indication of need for help).
Demand for mental health services among Australian’s aged 5–11 years in each defined need group based on 2013–2014 YMM survey data. a
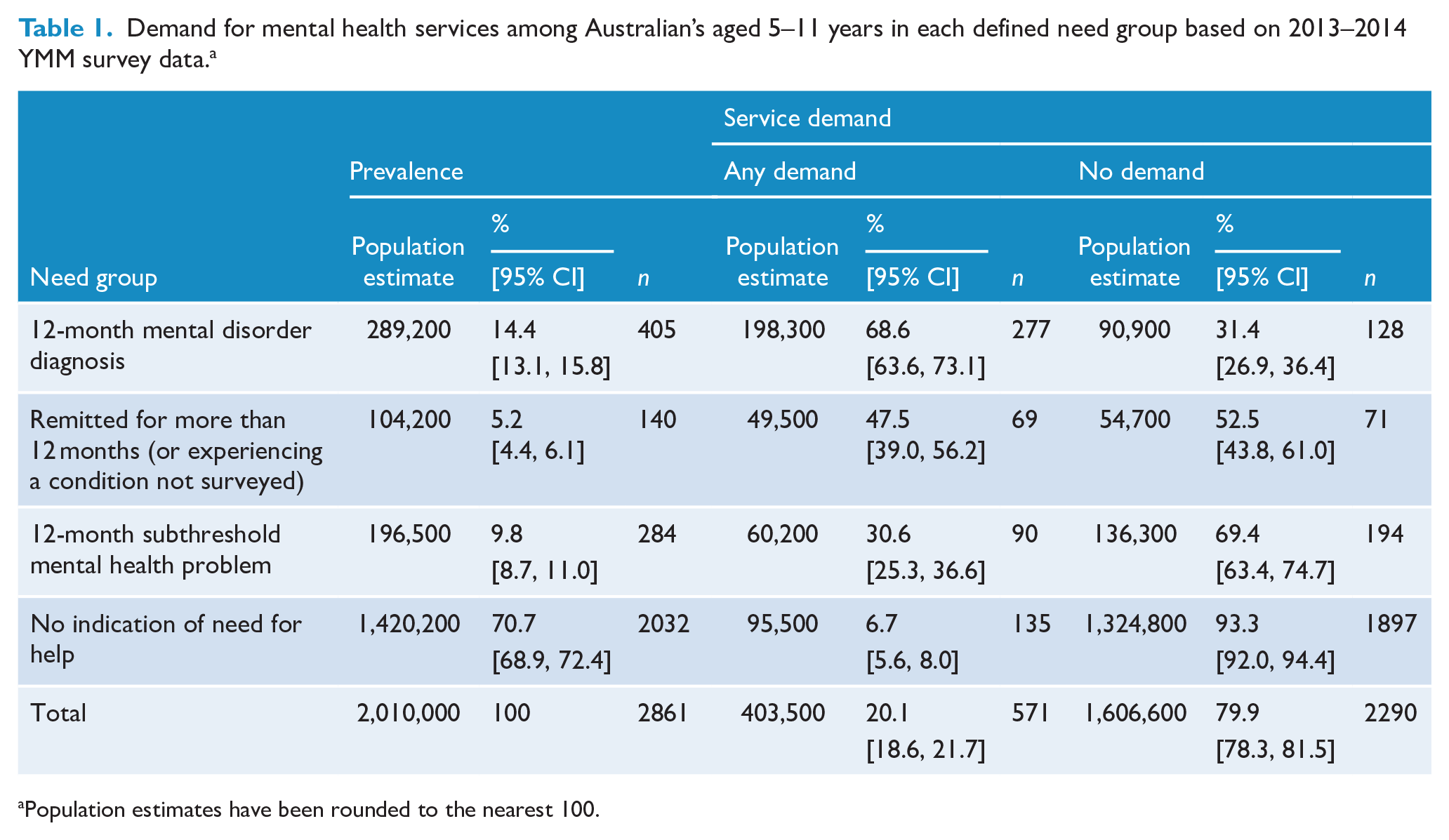
Population estimates have been rounded to the nearest 100.
The right-hand panels of Table 1 show the estimates of service demand in the past year. Overall, 20.1% of 5–11 year olds expressed a demand for mental health services. Rates of service demand varied across need groups, being highest for children with a 12-month disorder diagnosis (68.6%) and lowest for those in the ‘no indication of need for help’ group (6.7%). These patterns were somewhat similar for the two components of service demand (Figure 3). However, the proportion of children who did not use a service but perceived a need for help was higher in those with a 12-month subthreshold mental health problem (13.8%) as compared to those who had experienced a mental disorder diagnosis that had remitted for more than 12 months (or were experiencing a condition not surveyed) (9.3%). Notably, of all 5–11 years with any demand for services, 23.6% (95% CI: [20.1, 27.6]) did not meet the criteria for a 12-month subthreshold mental health problem and had never met the threshold for a mental disorder diagnosis (12-month or otherwise) (i.e. no indication of need for help).
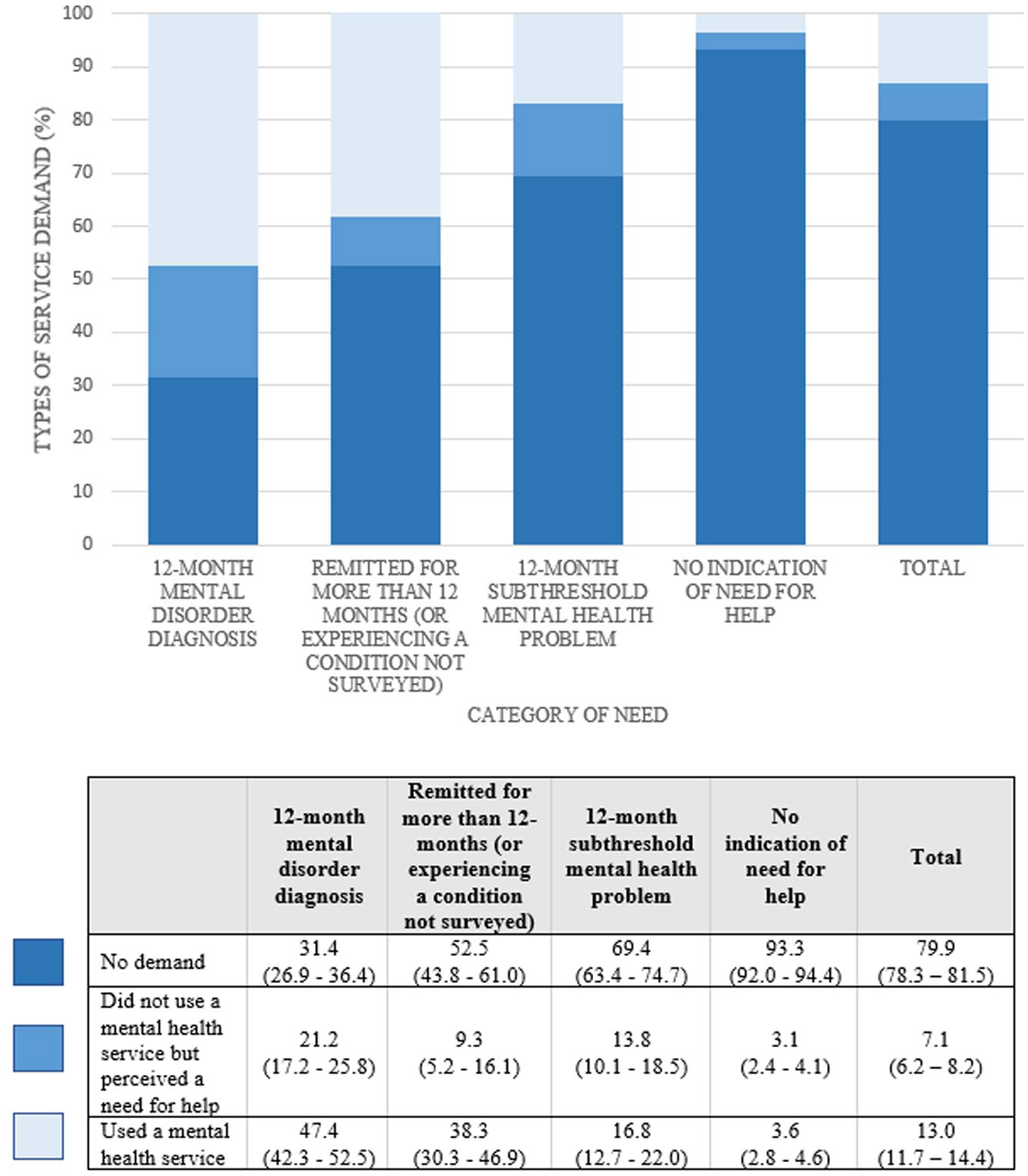
Proportion of young people aged 5–11 years in each need group reporting each type of service demand.
Among 5–11 year olds who used a service in the past year, the proportion in each need group who received the highest number of sessions of care from any one professional was highest among those with a 12-month mental disorder diagnosis (23.8%), followed by those with no indication of need for help (17.2%), those with a 12-month subthreshold mental health problem (13.8%) and those who had experienced a mental disorder diagnosis that had remitted for more than 12 months (or were experiencing a condition not surveyed) (13.6%) (Supplementary Information, Figure S1). Service demand appeared marginally higher for males compared to females in the 5–11 years needs group (Supplementary Information, Table S1).
12–17 year olds
The left-hand panel of Table 2 shows the population prevalence for each need group for adolescents aged 12–17 years. Overall, 18.9% of 12–17 year olds experienced a 12-month mental disorder diagnosis, a further 8.2% had experienced a mental disorder diagnosis that had remitted for more than 12 months (or were experiencing a condition not surveyed), 9.7% experienced a 12-month subthreshold mental health problem and 63.2% did not meet the criteria for a 12-month subthreshold mental health problem and had never met the threshold for a mental disorder diagnosis (12-month or otherwise) (i.e. no indication of need for help).
Demand for mental health services among Australian’s aged 12–17 year in each defined need group based on 2013–2014 YMM survey data. a
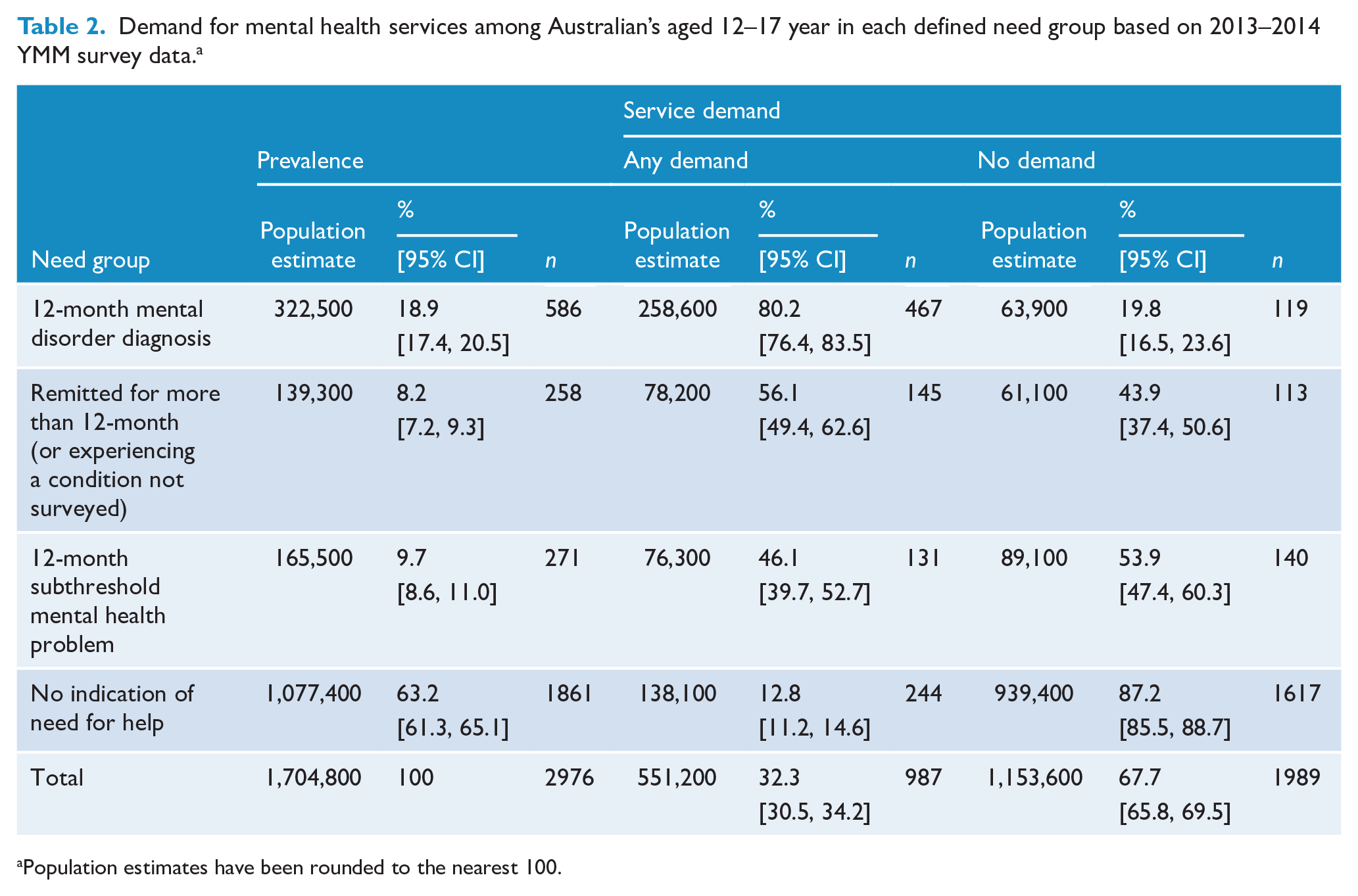
Population estimates have been rounded to the nearest 100.
The right-hand panels of Table 2 shows the percentage of 12–17 year olds in each need group who reported a demand for services. Again, rates of service demand varied as expected across need groups, being highest among adolescents with a 12-month mental disorder diagnosis (80.2%) and lowest among those with no indication of need for help (12.8%). Overall, 32.3% of Australia’s population of 12–17 year olds expressed a demand for mental health services. Similar to the 5–11 year olds, patterns were comparable for the two components of service demand (Figure 4). However, the rate of adolescents who did not use a service but perceived a need for help was higher in the 12-month subthreshold mental health problem group (20.2%) as compared to those who had experienced a mental disorder diagnosis (12.6%). Notably, of all 12–17 years with any demand for services, 24.6% (95% CI: [22.2, 28.1]) did not meet the criteria for a 12-month subthreshold mental health problem and had never met the threshold for a mental disorder diagnosis (12-month or otherwise) (i.e. ‘no indication of need for help’).
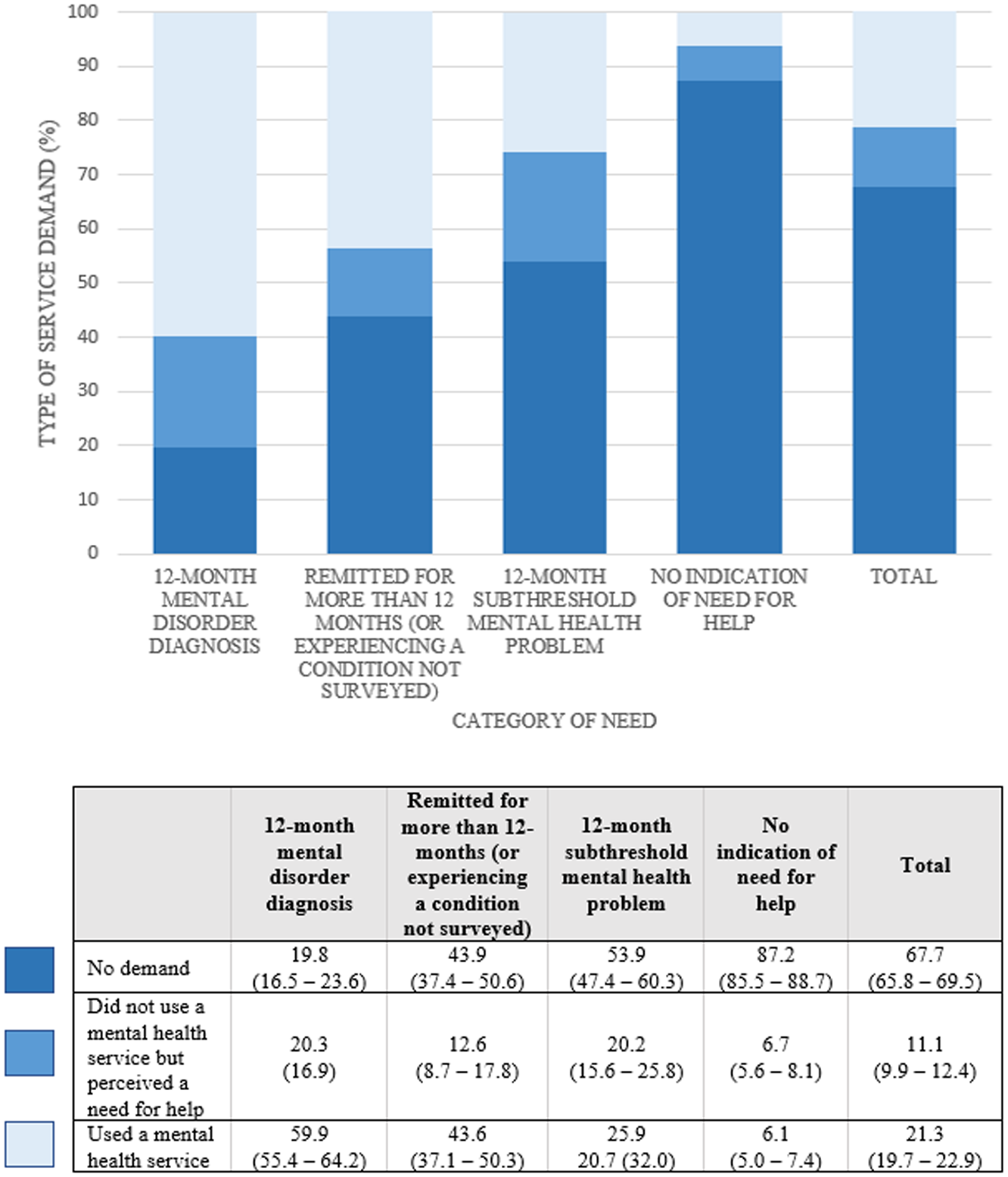
Proportion of young people aged 12–17 years in each need group reporting each type of service demand.
Among 12–17 year olds who used a service in the past year, the proportion in each need group who received the highest number of sessions from any one professional was highest among those with a 12-month mental disorder diagnosis (26.0%), followed by those who had experienced a mental disorder diagnosis but had remitted for more than 12 months (or who were experiencing another condition not surveyed) (24.6%), those with a 12-month subthreshold mental health problem (13.8%) and those with no indication of need (5.1%) (Supplementary Information, Figure S2). Dissimilar to the 5–11 years age group, service demand appeared marginally higher for females aged 12–17 years as compared to males (Supplementary Information, Table S2).
Discussion
This study examined demand for mental health services among Australian children and adolescents according to level of need as per their membership in one of four ‘need groups’. Findings revealed that 20.1% of 5–11 year olds, and 32.3% of 12–17 year olds, experienced a 12-month demand for mental health services in 2013–2014; this equated to 955,000 young people. For both age groups, service demand followed a gradient defined by need group membership. Rates of service demand were highest among young people with a 12-month mental disorder diagnosis, followed by those who had remitted for more than 12 months (or experienced a condition not surveyed), those with a 12-month subthreshold mental health problem and those with ‘no indication of need for help’. For the most part, when examining the individual components of service demand, patterns of service use and perceived need followed the same gradient. However, perceived unmet service needs were higher for those with a 12-month subthreshold mental health problem compared to those who had remitted for more than 12 months (or experienced a condition not surveyed) and young people with no indication of need for help contributed to a quarter of service demand.
Implications
The current paper extends the findings of Johnson et al. (2016) and Johnson et al. (2018) by investigating demand for mental health services across a full spectrum of need groups defined according to previous studies of adult populations (Bobevski et al., 2017; Harris et al., 2014). Specifically, it sheds light on service demand for Australian children and adolescents without a 12-month mental disorder. Although service demand among young people without a 12-month mental disorder diagnosis represents a considerable number of people (10% of Australia’s population of 5–17 year olds), it is probable that these groups have a lower level of service requirements compared to those with a 12-month mental disorder diagnosis. This was supported by our findings which showed that a larger proportion of young people with a 12-month mental disorder diagnosis received 10 or more sessions of care for emotional or behavioural problems from a single professional in the past year as compared to any other need group.
Children who experienced a mental disorder that had remitted for more than 12 months (or were experiencing a condition not surveyed) made up 12% of service demand for their age group; similarly, adolescents made up 14%. Notwithstanding differences in methodology, this is similar to the estimate of 18% in Australia’s adult population (Harris et al., 2014). Previous research suggests that those with a lifetime disorder who experience service demand have had recent relapses and/or require maintenance treatment (Druss et al., 2007; Harris et al., 2014). We hypothesise that there may also be other factors that have influenced ongoing service use, such as comorbid physical health concerns, educational or other government bureaucratic processes such as signing of forms for benefits or school exemptions, or an unsupportive family environment. Future research could examine these to predict the proportion of young people who will need further services beyond the duration of their illness.
Collectively, children and adolescents with a 12-month subthreshold mental health problem made up around 15% of service demand; this is far less than the previously reported 40% (Johnson et al., 2016). However, this variation in findings may be accounted for by differing methodologies. That is, the current study introduced an additional need group (i.e. remitted for more than 12 months [or experiencing a condition not surveyed]) which was not quantified separately in previous research. It is important to examine service demand separately for this need group for the purpose of service planning. As alluded to, those who have remitted for more than 12 months are likely to require different treatment approaches to those with a 12-month subthreshold mental health problem. Quantifying service demand separately for these need groups can help inform the quantity and level of services needed to meet the diverse mental health needs of Australia’s child and adolescent populations.
There are concerns, however, about whether it is appropriate to medicalise subthreshold mental health problems and hence provide unnecessary treatment when healthcare resources are limited (Sareen et al., 2013). It should be reiterated, however, that, in the current study, this grouping represents young people with a demand for services and hence, includes young people who are attending a service, or reporting a need for services, regardless of whether there is broader consensus on their need for care. While some research suggests that psychotherapy for young people with subthreshold depression does not reduce the likelihood of developing MDD in the following 12 months (Cuijpers et al., 2021), academic literature and Australian government policy has advocated for the early identification and treatment of mental health problems in childhood and adolescence (Kessler et al., 2005; McGorry et al., 2007; Productivity Commission, 2020). That is, early identification and treatment may have the potential to reduce the severity of future mental illness in some young people who experience subthreshold mental health problems that do not remit. At present, however, there is no way of determining which young people in this group benefit from care, nor what interventions are effective. While psychotherapy may not be the answer, brief assessments, psychoeducation, online interventions and parenting skills training may be appropriate. Further research is required to determine how best to meet the needs of those with a 12-month subthreshold mental health problem without creating health system access problems for those with a mental illness.
Finally, in both age groups, around a quarter of those who experienced service demand (an estimated 234,000 young Australians) were in the ‘no indication of need for help’ group. This is of particular interest given service demand was defined as use of and/or perceived need for mental health services. It could be speculated that important indicators of need were not included when classifying young people into need groups. The inclusion criteria used to define our need groups is based on a diagnostic measure (the DISC-IV); it does not consider the experience of self-harm, lifetime suicide attempt or transient psychological distress. However, findings from the YMM survey revealed that, around 95% of adolescents who reported 12-month self-harm, and 99% of those who experience a 12-month suicide attempt, also experienced parent- or self-reported MDD, or some other parent-reported mental health problem (Lawrence et al., 2015). Similarly, of young people aged 11–17 years who reported high or very high psychological distress as per the Kessler 10 Scale of Psychological Distress, over 90% also experienced parent- or self-reported MDD, or some other parent-reported mental health problem. Majority of young people with these experiences were therefore captured in the 12-month diagnosis group and hence, the inclusion of these other indicators would not have a significant impact on our findings. Some young people in the ‘no indication of need for help’ group, however, may have experienced other problems (e.g. experience of peer or family relational problems) and therefore may have accessed a service in need of information or for an initial assessment that did not require ongoing mental health treatment. This is further supported by our finding that, among young people without an indication of need who used a service for mental health problems in the past year, the highest number of sessions received from any one professional type was ‘one’ for almost one-third of 5–11 year olds, and two-thirds of 12–17 year olds (see Supplementary Information). Future research may examine the sociodemographic (e.g. family structure, parent highest level of education, household income) differences between young people in this group who experienced service demand versus those who did not. It is further speculated that sociodemographic factors may be a significant driver of service demand in this group rather than the experience of mental disorder symptoms or diagnoses alone. Indeed, findings from other analyses of data from the same survey suggest that greater health service use for emotional or behavioural problems may be influenced by family income, parent education, parent employment and family composition (Vu et al., 2018).
Limitations
There are a number of limitations to the current study. First, parents/carers were asked about their child’s experience of a broader range of lifetime disorders as compared to their experience of 12-month disorders. For example, parents/carers were asked whether their child had ever been diagnosed with an eating disorder. However, it could not be determined whether this was a 12-month diagnosis as per the DISC-IV. This means that there may have been some young people in the relapse prevention groups (i.e. lifetime disorder but not a 12-month disorder diagnosis) who had a 12-month mental disorder that was not captured using the DISC-IV. However, we speculate that the misclassification of young people would be small given that most lifetime disorders not assessed using the DISC-IV would likely be comorbid with one or more of those that were assessed with this measure. Second, only adolescents aged 13–17 years were asked questions pertaining to service use and perceived need; responses from those aged 12 years and younger were not captured and their classification therefore relied on parent-report. This was based on the assumption that younger children would be very unlikely to access mental health services without their parent’s knowledge, although this assumption has not been tested. As such, estimates of service demand, particularly for the 5–11 year old age group, may be underestimated. Third, we defined need group membership using subthreshold scores on the DISC-IV but there may be other indicators of need that could be used to define these groups which may result in different findings. However, as discussed above, it is unlikely that the inclusion of other indicators (e.g. 12-month self-harm, 12-month suicide attempt and/or transient psychological distress) would have significantly changed the findings of the analysis given the overlap between these other indicators and the experience of a 12-month mental disorder diagnosis. Fourth, there may be parents/adolescents who have not expressed service demand but may have an objective need for services that has not been identified due to lack of insight or fear of stigma. However, it was not possible to quantify the proportion of those who reported no service demand that had an objective need for services but did not report an expressed need for services.
Conclusion
Finally, this is the first analysis to quantify prevalence and mental health service demand across a spectrum of need groups for Australia’s population of young people. Service demand estimates derived from this analysis can inform estimates of population mental health service need for planning, such as those used in the NMHSPF. This is an important step towards developing an evidence-informed integrated mental health system that meets the needs of the entire population. Planning mental health services for a broad and more inclusive spectrum of need groups than previously estimated may help reduce the long-term burden caused by mental health problems for young people in Australia.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211069874 – Supplemental material for Estimating demand for mental health care among Australian children and adolescents: Findings from the Young Minds Matter survey
Supplemental material, sj-docx-1-anp-10.1177_00048674211069874 for Estimating demand for mental health care among Australian children and adolescents: Findings from the Young Minds Matter survey by Claudia Pagliaro, Madeleine Pearl, David Lawrence, James G Scott and Sandra Diminic in Australian & New Zealand Journal of Psychiatry
Footnotes
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by C.P. The first draft of the manuscript was written by C.P. and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The current analysis was approved by the Office of Research Ethics at The University of Queensland.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This paper builds on an earlier analysis conducted for the National Mental Health Service Planning Framework project funded by the Australian Government Department of Health and all Australian state and territory health departments. This publication reflects the views of the authors and should not be construed to represent the Department of Health’s views or policies. The original funders had no role in the study design, analysis, interpretation or writing of this paper. J.G.S. is supported by funding from Metro North Mental Health Service.
Availability of data and material
Data from the Young Minds Matter survey is available via request from the Australian Data Archives.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.