
Abstract
Objective:
This study aimed to investigate the factors associated with parricide in patients with schizophrenia who committed homicide.
Method:
Among patients with schizophrenia who were in the National Institute of Forensic Psychiatry between November and December 2007, 88 patients who committed homicides were enrolled; 59 had committed parricide, and 29 had killed strangers. Medical charts, written expert opinions, written records of police or prosecutors, and court decisions were reviewed. Direct interviews with patients were also conducted.
Results:
Significant factors associated with parricide among homicidal patients with schizophrenia were living with the victim, female sex of the victim, and offense-provoking events including scolding, threatening forced hospitalisation, and forcing medication on the patient before the homicide. Capgras syndrome was present at a significantly higher rate in the parricide group than in the stranger group. Drug compliance at the time of the offence was low in both groups.
Conclusions:
Untreated psychotic symptoms such as Capgras syndrome, living with elderly parents, especially mothers, and conflicts caused by victims’ scolding, threatening forced hospitalisation, and forcing medication on the patients are associated with parricide among homicide offenders with schizophrenia.
Introduction
Parricide, the crime of murdering a parent, is extremely serious. Especially in a society such as Korea, in which traditional Confucian ideas are deeply rooted, parricide is a shocking event that shakes filial piety, an important Confucian precept. Reflecting this, parricide is subject to an especially onerous penalty in Korean criminal law.
Parricide constitutes 2% of all murders in the USA (Heide, 1989), 1–2% in the UK (Green, 1981), and 2.8% in France (Devaux et al., 1974). During the last 10 years, the average rate of parricide in Korea was 5.3% of all homicides (Figure 1).
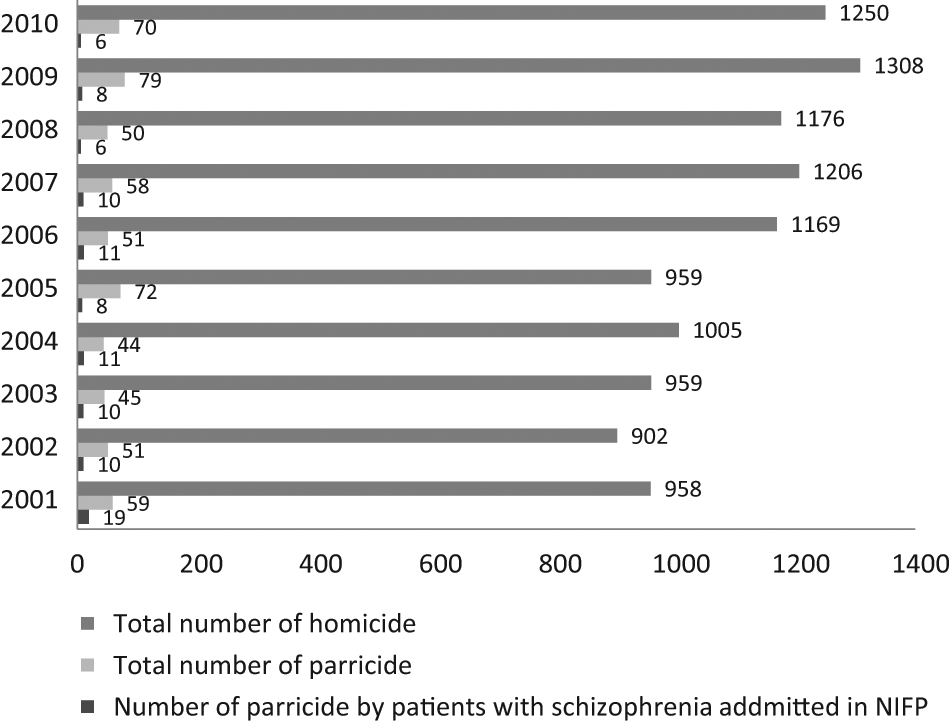
Statistical data regarding the incidence of homicide by patients with schizophrenia admitted to the National Institute of Forensic Psychiatry and the incidence of total parricide in comparison to all homicides committed from 2001 to 2010 in Korea (statistics by the Supreme Public Prosecutor’s Office and the National Institute of Forensic Psychiatry, 2011).
The most notable characteristic of parricide is that a high proportion of assailants suffer from major mental disorders. In studies on parricide, 47–60% of parricidal offenders suffer from psychosis (Devaux et al., 1974; Young et al., 1998). Although adolescent parricides tend to be committed as a means to escape from long-term severe physical or sexual abuse, most adult parricidal offenders have severe and prolonged mental illness (Hillbrand et al., 1999). In a Korean study, parricides caused by perpetrators’ mental disorders accounted for 43.1% of all cases (Jung et al., 2009). Among psychiatric diagnoses, schizophrenia is the most common diagnosis in parricidal patients. More than 50% of patients with mental disorders who committed parricide suffered from schizophrenia (Baxter et al., 2001; Marleau et al., 2003).
Several studies have attempted to identify risk factors for parricide in patients with schizophrenia. A majority of parricides committed by patients with schizophrenia are committed by sons (Green, 1981), with a tendency toward matricide (McKnight et al., 1966). The murders typically occur when the victims are alone at home with the offender (Green, 1981). Patient offenders rarely have previous criminal histories, but previous violent tendencies toward their victims are often evident (Baxter et al., 2001; Young et al., 1998). The mental disorder occurs early and tends to be serious for parricidal patients (Nordström and Kullgren, 2003). Medication compliance was often low when the incident occurred (Millaud et al., 1996). With regard to the psychopathologic aspects, some of the patient offenders experienced auditory hallucinations commanding them to harm their parents, and some had Capgras syndrome (CS), which made them believe their parents were replaced with other people or agents (Green, 1981; Young et al., 1998). The presence of threat/control override (TCO), a delusion that causes a person to feel personally threatened or involves the intrusion of thoughts that can override self-control, is recognised as another risk factor of parricide in patients with schizophrenia (Link et al., 1998). Parental victims could be rated high on constructs of ‘expressed emotion’ and engaged in hostile-dependent relationships with the patients (Newhill, 1991). Young et al. (1998) reported that verbal or psychological abuse of the patient by the victim occurred before parricide in 40% of cases.
Existing studies are limited by small sample sizes and retrospective methodologies because prospective study designs to research parricide have distinct ethical and practical limitations. In Korea, the National Institute of Forensic Psychiatry (NIFP) is the only forensic psychiatric hospital that treats the offenders with mental illness who are sentenced to mandatory psychiatric treatment. All sentenced parricidal patients with schizophrenia are admitted to the NIFP with all the documents related to the offence. With this unique system, we could determine the factors that could be associated with parricide among schizophrenic patients who committed homicide with a relatively large sample and various information resources, including direct interviews.
Materials and methods
Subjects
The NIFP, operated by the Ministry of Justice in Korea, provides conditions of special security for patients from throughout Korea and currently has a capacity of about 1000 beds. Most offenders whose crimes are regarded as related to mental illness are initially referred to the NIFP for an expert opinion on their criminal responsibility. If they are demonstrated to be guilty but mentally ill or not guilty by reason of insanity, they are sentenced to compulsory psychiatric treatment at the NIFP until they are believed to be safe from recidivism.
From the computerised case registry system of the NIFP, all patients diagnosed with schizophrenia by DSM-III-R or DSM-IV in the hospital between November and December 2007 were screened. Parricide refers to the crime established by murdering lineal ascendants of one’s own or one’s spouse, but in this study, only parricides committed toward the patient’s parents were included. Among 385 hospitalised patients with schizophrenia, 65 had killed a parent and 31 had killed a stranger. The stranger was defined as any case in which the victim had personally known the offender for fewer than 24 hours (Nielssen et al., 2011). The subjects were admitted between May 1997 and October 2007. Eight patients refused to participate in the study, leaving a total of 88 patients (59 parricidal offenders, 29 stranger-killing offenders) who gave informed consent and were enrolled.
Assessments
The subjects were divided into two groups: the parricide group, who murdered parents; and the stranger group, who murdered strangers. Demographic and clinical characteristics of the patients in these two groups were compared by reviewing medical records and written expert opinions regarding the offenders’ mental status; these reports were highly detailed because their diagnoses were an important basis for determining the offenders’ criminal responsibility. More detailed information, when needed, was obtained through direct interviews with the patients. Criminal characteristics were assessed by reviewing the written records of police or prosecutors and the court decisions.
Information was gathered by two psychiatrists with a structured case registry form. Medical records in the NIFP, written expert opinions regarding the offenders’ mental status, and written records of police or prosecutors use common forms. Data collection and analyses were performed in an anonymous manner. This study was conducted with the approval of the Ministry of Justice. The authors followed the guidelines of the Declaration of Helsinki.
Statistical analysis
The χ2 test or Fisher’s exact test was used for categorical data. The t-test was used for the analysis of continuous data between the two groups.
To assess which variables were significantly associated with parricide, a generalized estimating equation (GEE) (Liang and Zeger, 1986) method was used. Because the GEE method is widely used to account for the correlations among the observations from the same individual, the multiple homicides could be considered by five cases in the parricide group and one case in the stranger group, respectively.
With a candidate set of potential factors that showed significant differences in the χ2 test or t-test, the model with the least quasi-likelihood under the independence model criterion (QIC) for GEE (Pan, 2001) was accepted as the best fitting model. The significance level was set at p< 0.05. The statistical process was conducted using SAS, version 9.2 (SAS Institute, Cary, NC, USA).
Results
Demographic and clinical characteristics of the patients
Table 1 provides data on patient demographics and characteristics. No statistically significant difference in age or sex was found between the two groups. The age at onset of schizophrenic symptoms was significantly earlier for the parricide group (23.1 ± 5.3 years) than for the stranger group (26.1 ± 5.2 years; p< 0.05).
Demographic and clinical characteristics of the 88 patients.
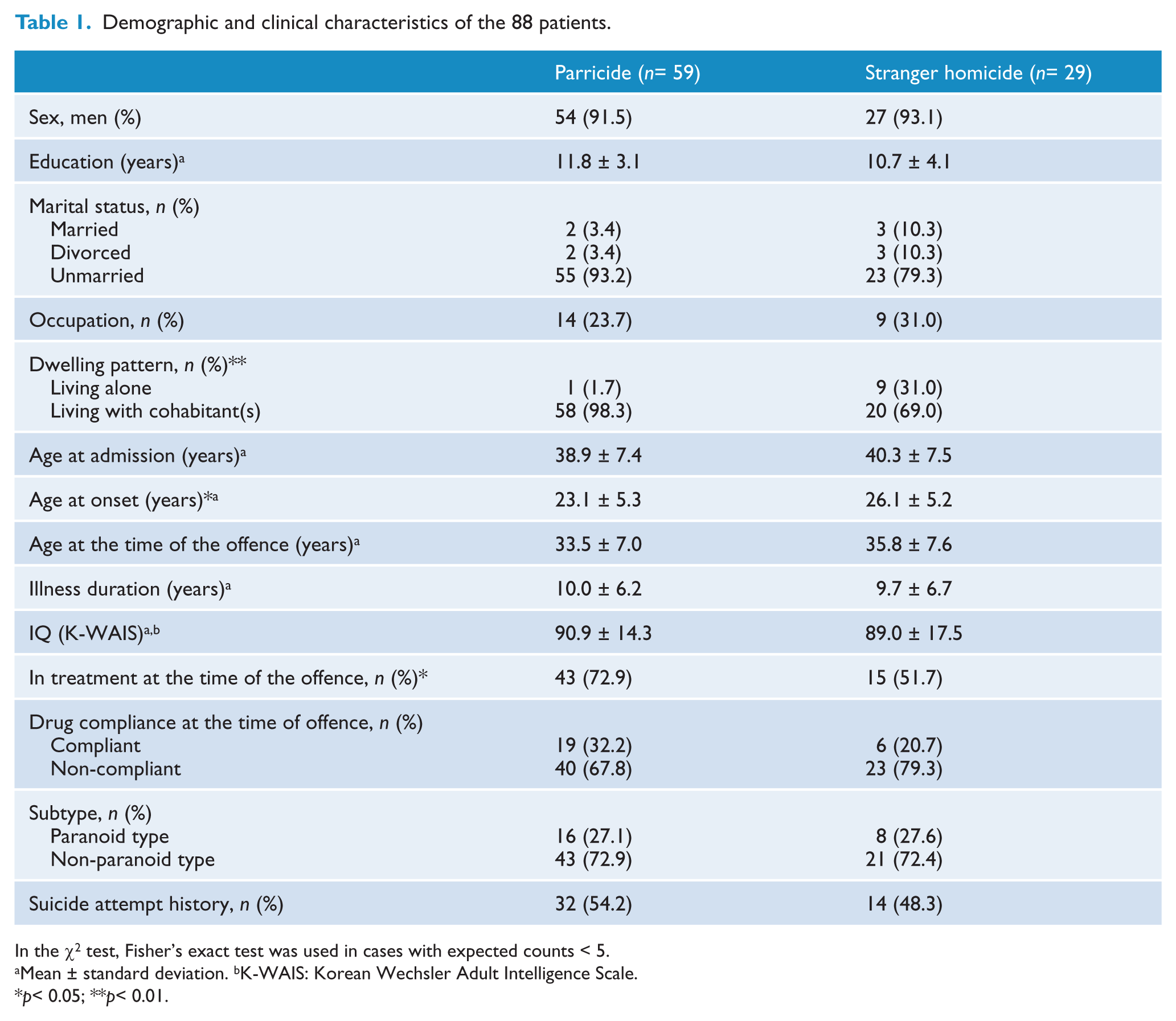
In the χ2 test, Fisher’s exact test was used in cases with expected counts < 5.
Mean ± standard deviation. bK-WAIS: Korean Wechsler Adult Intelligence Scale.
p< 0.05; **p< 0.01.
A significant difference was apparent in dwelling patterns between the groups (p< 0.01). Patients living alone were more common in the stranger group than in the parricide group.
The parricide group had a higher rate of contact with psychiatrists before the murder (n = 43, 72.9%) than the stranger group (n = 15, 51.7%; p< 0.05). However, the rate of actually taking prescribed medications at the time of the murder was low in both groups (n = 19, 32.2%, in the parricide group and n = 6, 20.7%, in the stranger group).
Characteristics related to homicide
As shown in Table 2, 59 patients killed 64 victims in the parricide group, including 19 patricides and 35 matricides, and five cases in which both parents were killed. The victims in the stranger group included neighbours, passers-by, co-workers, hospital colleagues, and others. Regarding the genders of the victims, 67.8% of the victims in the parricide group were women, whereas men accounted for 79.3% of the victims in the stranger group (p < 0.05). The location of the parricide was usually the home in which the victim and the offender lived together, whereas various locations made up the murder sites in the stranger group. The most common method of killing in both groups was the use of a sharp instrument. The rate of intoxication by alcohol or other drugs during the offence was low in both groups, at 5.1% for the parricide group and 10.3% for the stranger group.
Characteristics related to homicide.
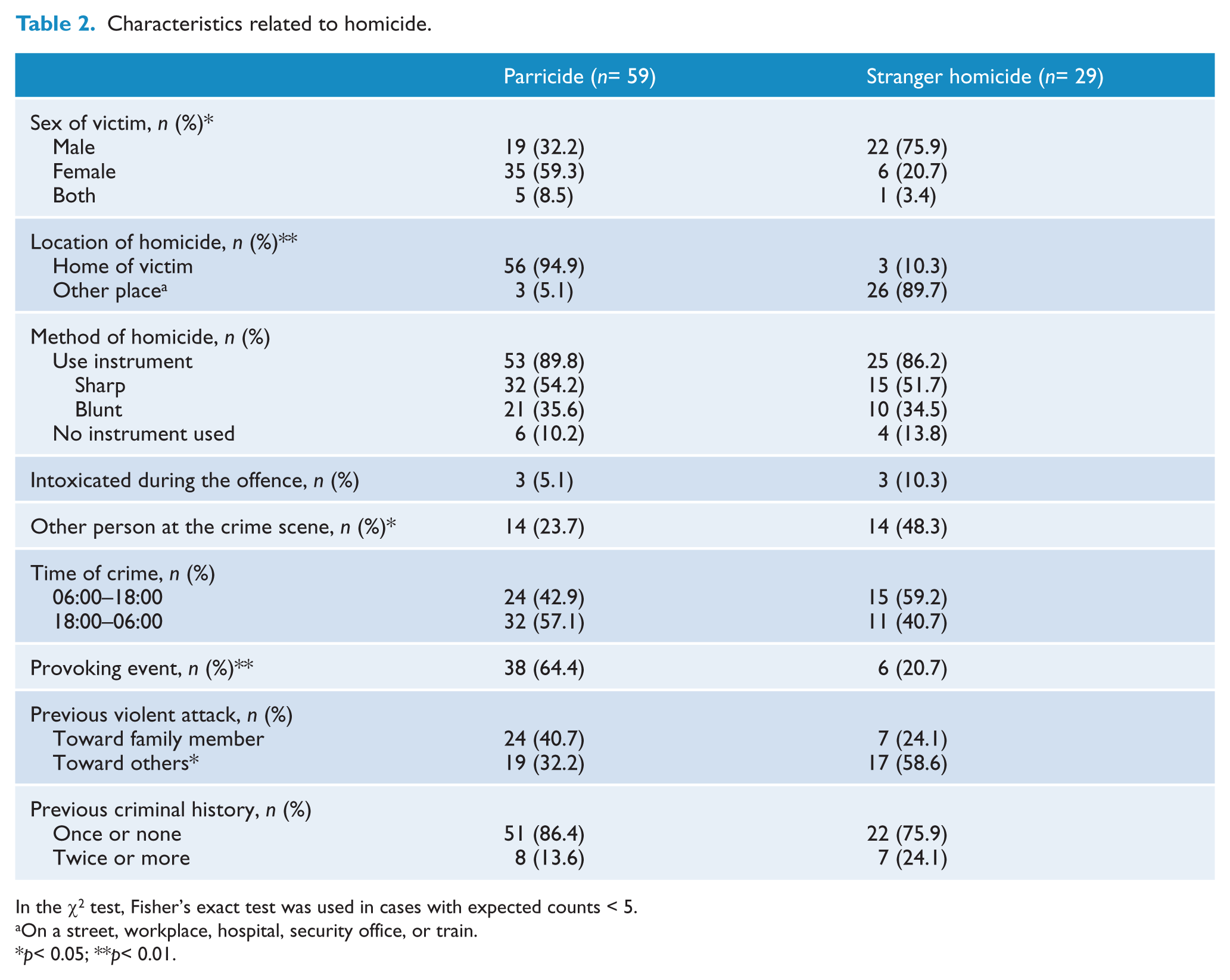
In the χ2 test, Fisher’s exact test was used in cases with expected counts < 5.
On a street, workplace, hospital, security office, or train.
p< 0.05; **p< 0.01.
Regarding the history of violent behaviour, 40.7% of the patients in the parricide group showed violent behaviour toward their victims, but this was not significantly different compared to the stranger group.
Psychiatric symptoms and provoking events related to homicide
Provoking events, including scolding patients’ behaviour, threatening forced hospitalisation, or forcing medication, existed at the time of the parricide in 64.4% of parricide cases (Table 3). Homicide of strangers was usually caused by the patients’ own delusions, with no specific triggering factors, which, when they occurred, included the victims’ blaming or cursing at the patients (p< 0.01).
Psychiatric symptoms and provoking events related to homicide.
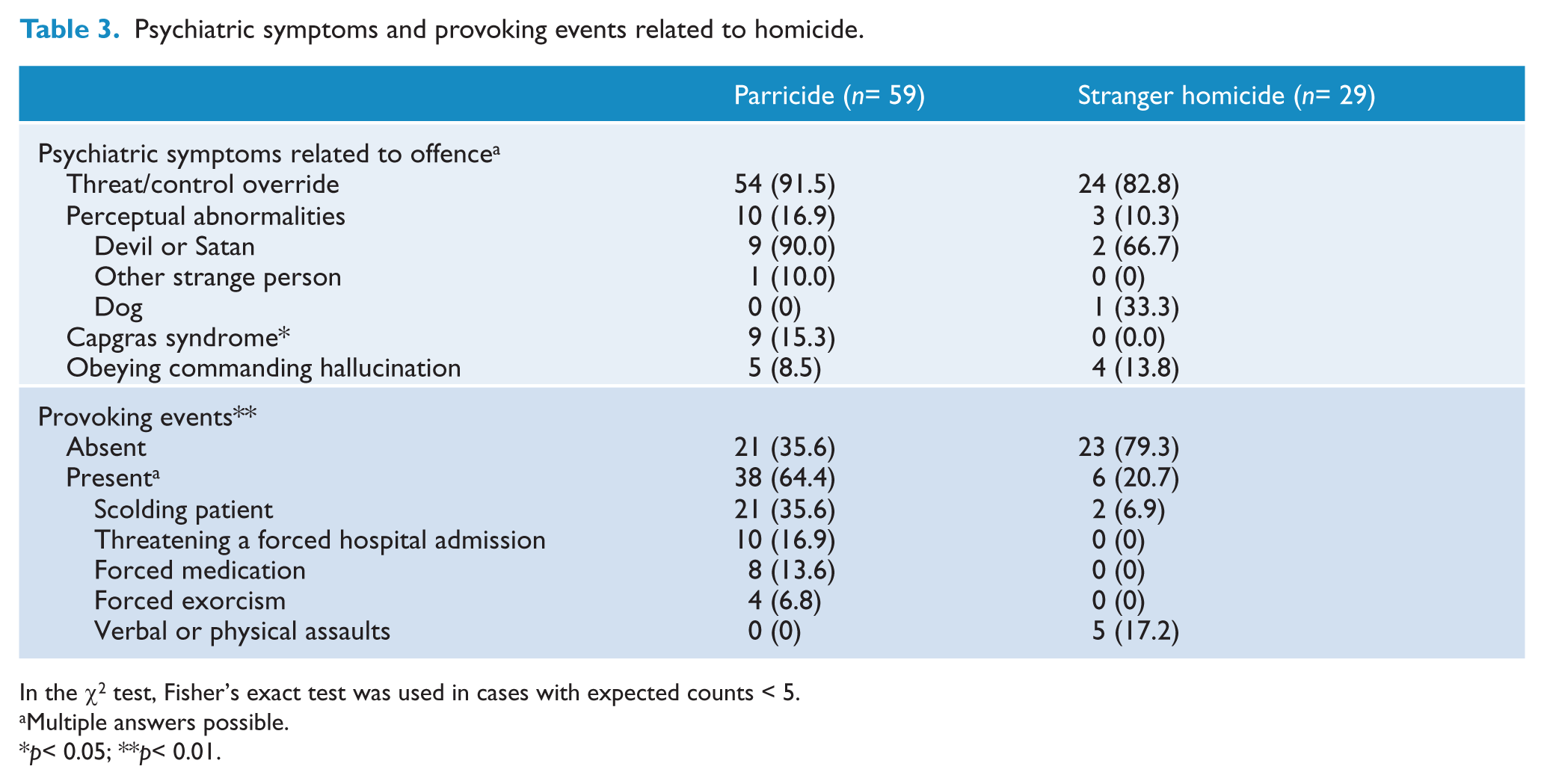
In the χ2 test, Fisher’s exact test was used in cases with expected counts < 5.
Multiple answers possible.
p< 0.05; **p< 0.01.
CS was found in nine patients (15.3%) in the parricide group only. The most common psychiatric symptoms related to homicide in both groups were TCO symptoms, which occurred in 54 patients (91.5%) in the parricide group and 24 patients (82.8%) in the stranger group.
Factors associated with parricide among patients with schizophrenia who committed homicide
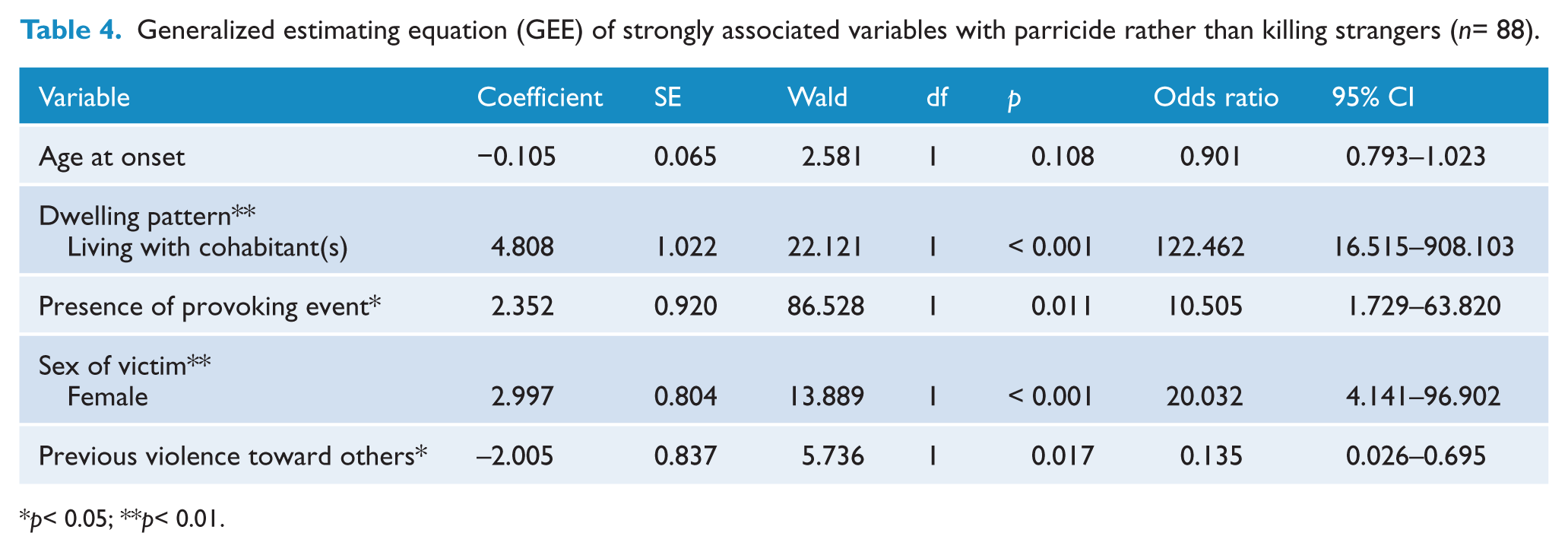
The GEE model-fitting results showed that living with a victim, a provoking event before homicide, and female sex of the victim were significantly associated with parricide among homicidal patients with schizophrenia (Table 4). The odds indicated that patients with schizophrenia who lived with their victims were 122.5 times more likely (95% CI, 16.515 to 908.103), those who experienced provoking events before the homicide were 10.5 times more likely (95% CI, 1.729 to 63.820), and those who killed female victims were 20.0 times more likely (95% CI, 4.141 to 96.902) to commit parricide than other homicidal patients who exhibited none of these factors.
Generalized estimating equation (GEE) of strongly associated variables with parricide rather than killing strangers (n= 88).
p< 0.05; **p< 0.01.
Discussion
The Korean government has tried to change the mental health system into a community-based system (World Health Organization, 2006). Since the enactment of the Mental Health Act in 1995, 151 community mental health centres, 170 rehabilitation centres, and 56 psychiatric nursing homes have been established (Asia Australia Mental Health, 2008). Despite these efforts, Korean families assume the major responsibility of caring for mentally ill patients, including community support and financial burdens (Crowe, 2005). Parents, especially, have an obligation to support their offspring with mental illness in the Korean social and cultural environment. In this study, 98.3% of the parricidal patients lived with their elderly parents. Significantly earlier onset of the psychotic symptoms of the patients in the parricide group, in accordance with the findings of a previous study (Nordström and Kullgren, 2003), may make it difficult for them to be independent from their parents.
In Korea, where Confucian ideas are deeply rooted, any type of deviance from the norm represents a dissonance from the ideal state of harmony (Seeman, 2009). Filial piety, ‘hyo’, is also highly regarded from the Confucian perspective, as seen in the traditional Korean custom that children should live in a mud hut built near their parents’ tomb for at least 3 years after the parents’ deaths (Kim, 2008). This concept shows respect for parents and, in more general terms, engages in good demeanour toward parents and outside the home to foster a good reputation for one’s parents. In this culture, parental expectations for their offspring’s good manners and appropriate behaviours can be high. Thus, discipline for regressed and disturbing behaviour by the patient may be stricter than in Western countries. In our study, parents scolded patients regarding behaviours that were possibly associated with the patient’s mental illness, including demands not to wander at night, not to smoke at night, to clean up their rooms, to have regular mealtimes, to study hard, to take medications, and to be thrifty. Five victims refused to give money to the patients when they demanded it. These limiting actions may have been perceived by the patients as coercive and hostile on the part of the parents (Straznickas et al., 1993).
Mothers, particularly, are the group with the highest risk of becoming victims of homicide by patients with schizophrenia (Devaux et al., 1974; Estroff et al., 1998; McKnight et al., 1966). In this study, the rate of matricide was also higher than the rate of patricide, and female sex of the victim was a significant factor that raised the risk of parricide 20-fold. Raising a child is primarily the mother’s responsibility and they are the caregivers who spend the most time with the patients. Thus, they play major roles in forcing medications, forcing hospitalisations, and providing discipline. In this process, long-term conflicts between mothers and patients can occur, and mothers can be direct targets of longstanding delusional ideas of persecution or paranoid ideation or both. One mother in this study even included ground antipsychotic drugs in the patient’s food. After becoming aware of this action, the patient, who had poor insights regarding his mental illness, developed a persecutory delusion that his mother wanted to poison him.
The patient’s usual hostility toward the victim tended to appear as violent behaviours before the homicide. Among parricidal patients, 40.7% had past histories of violent behaviours toward their victims. Studies reported that 15% of parricidal patients threatened their victims and 26% directly attacked their victims several weeks or months before the parricide (Green, 1981; Young et al., 1998). However, the victims might have considered this violence as an unavoidable effect of mental illness and tolerated it in cases of domestic violence (Humphreys et al., 1992), whereas in cases of violence toward others outside their family, offenders are subject to legal punishment. Cultural barriers including social stigma against mental illness and a strong attitude of ‘not in my backyard’ by many Koreans, often make it difficult for parents to expose the domestic violence perpetrated by offspring with mental illness and to reintegrate patients into the community (World Health Organization, 2006). Families with a mentally ill member live in silence, secrecy and shame, lest an illness like schizophrenia interfere with marriage, jobs and community respect, not only for the ill patient but also for the family (Seeman, 2009). In these cases, the caregivers seem to lose their sense of judgement about their own safety. In many studies, a past history of violence has received attention as the most important predictive factor for future violence (Klassen and O’Connor, 1988; Tardiff et al., 1997). Thus, it is especially important to be vigilant about the existence of domestic violence when elderly parents are taking care of patients, because such awareness may prevent a family tragedy. In addition, clinicians treating individuals with schizophrenia should counsel and educate significant family members regarding the nature of schizophrenia; these family members may sometimes be perceived negatively because they try to be helpful and promote treatment for the patient. Clinicians should also provide guidance on how family members can learn to cope with the illness over time, including ways to avoid inappropriate expectations (Anderson et al., 1986; Bourget et al., 2007). In these aspects, community care and mental health services must be available and approachable and actively support family members (Nordström et al., 2006).
Everyone that has psychotic symptoms and conflicts with parents does not pose a risk of parricide. Young et al. (1998) insisted that treatment non-adherence plays a crucial role in parricide. In this study, more patients in the parricide group periodically contacted mental health professionals than did those in the stranger group. The reason for this finding is probably that the victims who lived with the patients forced them to receive psychiatric care. However, many patients in both groups denied their mental illness and were angry that they were stigmatised as ‘patients with mental illnesses’. The finding that a high percentage of patients did not take their medications at the time of the offence (67.8% in the parricide group and 79.3% in the stranger group) supports this opinion. In previous studies on matricide, only 17% of patients were receiving active psychiatric treatment when they committed the homicide, despite a long duration of illness (Green, 1981). It has been suggested that inviting their psychotically ill child who refused treatment to live with them despite extremely contentious relationships that involved threat of harm to the parent is a warning sign for parricide (Hillbrand and Cipriano, 2007). A lack of insight and lack of medication compliance are part of a set of situations that could lead to parricide (Bourget et al., 2007).
An outpatient treatment order system was introduced in Korea by the amendment to the Mental Health Act in 2008. However, with some limitations, it is difficult to expect the practical effect of this order (Seo, 2010). First, it is applied only when the patients are discharged after forced admission. Thus, it cannot be an alternative to forced admission. Second, it is applied only to those who can afford the cost of outpatient treatment. Third, it does not demand a detailed treatment plan. Thus, the treatment can be limited only to control of psychotic symptoms by compulsory pharmacotherapy, although integrated community mental health services including rehabilitation are needed. Fourth, it also has no regulations that require continuous monitoring of the patient who has the outpatient treatment order and no specific guidelines for follow-up measures when the patient is non-compliant with the order. Currently in Korea, residential facilities for patients with mental illness are insufficient, with only 1.7 beds per 100,000 individuals. Moreover, 56% of those facilities are concentrated in Seoul and the suburbs (Gyeonggi area) (Seo, 2007). This also acts as a limitation of outpatient treatment orders.
Recently efforts to reduce the recidivism rate related to mental illness have been tried by the Ministry of Justice in Korea. One attempt is to register the offenders at a community mental health centre after discharge from the NIFP and let them receive case management services. The other is to discharge offenders from the NIFP under a probationary state over a specific period. Then a probation officer regularly checks whether the patient is compliant with outpatient treatment or community mental health centre services. When patients fail to comply with these treatments, the law allows for automatic rehospitalisation into the NIFP without legal processes for compulsory psychiatric treatment. The effect of this system on reducing the recidivism rate should be further verified.
Regarding psychiatric symptoms, CS was observed significantly more frequently in the parricide group. CS is an unusual type of delusional belief that someone significant or well known to an individual, usually a close relative or family member, has been replaced by an imposter with a strong physical resemblance (Todd et al., 1981). It is estimated to occur in up to 4% of psychotic patients (Edelstyn and Oyebode, 1999). In this study, CS was observed at a higher rate in the parricide group than has been reported in patients with psychosis. CS increases the risk of violent behaviour toward the targeted person (Rentrop et al., 2002). Attempts to do physical harm to the misidentified person are believed to stem from the individual’s belief that the imagined imposter threatens his or her welfare in some way (Silva et al., 1992). Victims of CS violence are usually misidentified family members living with the patient (Bourget and Whitehurst, 2004). Thus, CS should be included in an assessment of the risk for violent behaviour. Fortunately, patients with CS seem to respond well to antipsychotic agents (Bourget and Whitehurst, 2004).
Other psychotic symptoms related to homicide in both groups are largely TCO symptoms, that is, perceptual abnormalities at the time of the homicide and commanding hallucinations. In both groups, the most common TCO symptom was that the victims would harm the patients. The cases in which the patient murdered the victim by obeying a commanding auditory hallucination were rare. This finding corresponds to the results of previous studies that investigated the association between commanding hallucinations and violence (Cheung et al., 1997). Regarding perceptual abnormalities, most patients reported that the victims were seen as a ‘devil’ or ‘Satan’ who was trying to harm the patient when he or she committed the crime. One patient in the stranger group reported that the victim looked like ‘a dog’.
Although schizophrenia itself independently increases the risk of violence (Brennan et al., 2000), accompanying alcohol or substance abuse increases this risk significantly (Räsänen et al., 1998; Swanson et al., 1990). However, the offenders with schizophrenia who killed members of their biological families were seldom intoxicated (Nordström et al., 2006). Alcohol and other substance use disorders have been reported to be strikingly rare in mentally ill parricidal offenders: 3% (Green, 1981), 4% (Young et al., 1998), and 7.6% (Walsh and Krienert, 2009). In this study, the rate of alcohol or other drug use at the time of the offence was low. This result is in accord with previous studies on parricide, although it is possible that the patient’s psychotic deterioration might have hidden the presence of alcohol or other drugs (Lee et al., 1999) or, related to legal benefit, the patient might have hidden that he was intoxicated when the incident occurred.
This study has some limitations. First, only patients who were sentenced to forced psychiatric treatment were enrolled. Thus, these patients may have more serious psychopathologies than patients who are not referred for forced psychiatric treatment after a mental status evaluation. Second, there was no comparison group of non-homicide offending patients with schizophrenia. Thus, the factors associated with parricide in this study are just associations with parricide among homicidal offenders with schizophrenia compared to non-parricide cases and are not for parricide itself compared to non-homicide. Third, although our sample size is larger than those of other studies, parricide is a rare event, and a small sample size remains a limitation. The estimated confidence intervals of odds ratios were wide due to this small sample size. Fourth, the data were collected retrospectively. An ideal study design would be prospective, but such a design would have distinct ethical and practical limitations, which may be the main reason that studies of predictors and clinical characteristics of parricide have used retrospective designs. Despite these limitations, this study enrolled a relatively large sample, reviewed diverse written information resources in addition to medical records, and attempted direct interviews with patients who are currently hospitalised, suggesting relatively better data quality relative to previous studies.
Victims of extreme and fatal violence by patients with schizophrenia have generally been family members (Nordström and Kullgren, 2003). Nevertheless, domestic violence by patients with schizophrenia has been avoided as a subject of research because of concerns about the possibility that it might increase stigmata for patients with schizophrenia (Solomon et al., 2005). However, without adequate scientific evidence, it is impossible to offer essential family support or to cope with the unnecessary prejudices of the public. Thus, domestic violence by patients with schizophrenia needs to be a primary concern in the mental health field. In addition, psychiatric problems of other family members after a parricide should be investigated in the future. Parricide causes serious psychological trauma to all family members. If the trauma experienced by other family members is not resolved, the patients will not be able to return to the family after treatment. Even if the patient returns to the family after treatment, persisting conflicts and violence are to be expected.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.