
Abstract
Objective:
Antipsychotic drug treatment alters status on key risk factors for cardiovascular disease. The aim of this study was to test whether cardiovascular risk factor associations differ in adults with psychosis and adults from the general community.
Method:
Data were analysed for those aged 25–64 years from a nationally representative psychosis sample (n = 1,457) and a national comparator sample (n = 8,866). The Pearson correlation coefficient was used to estimate the association among tobacco use, body mass index, waist circumference, diastolic and systolic blood pressure and fasting total-, LDL- and HDL-cholesterol, triglycerides and plasma glucose. The robust Levene test was used to test for sample differences in variance.
Results:
Correlations among cardiovascular risk indicators and between cardiovascular risk indicators and age were often significantly weaker in those with psychosis than in those from the national comparator sample. This was not due to a reduction in variance within the psychosis sample.
Conclusions:
Risk prediction that synthesizes multivariate risk indicator data needs to be connected to verified cardiovascular morbidity and mortality in those with psychosis to determine if standard risk calculators adequately discriminate those at high, medium and low future risk of cardiovascular morbidity and mortality. Until then the clinical implications of low or absent correlations among cardiovascular risk indicators and their low or absent association with increasing age is unclear but may indicate that risk equations commonly used in the general population may not be applicable for those with treated psychosis.
Introduction
Adults with psychosis are twice as likely to die from cardiovascular disease as adults in the general population (Saha et al., 2007) and often develop coronary heart disease at a relatively early age (Hennekens et al., 2005; Lawrence et al., 2001). Exposure to some cardiovascular risk factors, such as cigarette smoking (Myles et al., 2012), typically precedes the diagnosis of psychosis while others, such as obesity, dyslipidemia and diabetes, are worsened by its pharmacological treatment (Foley and Morley, 2011; Nielsen et al., 2010). Whether or not antipsychotic drug effects alter the individual and combined effects of cardiovascular risk factors is unknown but, in the general population, these risk factors are substantially interrelated and have much stronger effects on cardiovascular outcomes in combination than they do individually (Mendis, 2010; Yusuf et al., 2004).
The association between clusters of risk indicators and cardiovascular morbidity and mortality in the general population has been used to develop risk calculators to predict risk. Prediction of future risk is important clinically because many individuals experience no symptoms prior to potentially fatal cardiovascular events and a combination of several modestly raised risk factors may result in a higher total risk than one very substantially raised risk factor (Cooney et al., 2009). The universal recommendation of cardiovascular disease prevention guidelines is that all asymptomatic individuals should undergo a global risk assessment (Deedwania, 2001; Greenland et al., 2010). Risk calculators are used not only to estimate future risk but also to trigger the implementation of lifestyle or pharmacological interventions designed to lower risk in those whose estimated global risk exceeds pre-specified risk thresholds (Goff et al., 2014; Rosenzweig et al., 2008). Wide deployment of uniform methods for estimating cardiovascular risk means that increases and decreases in predicted risk can be tracked across time and across populations and uniform thresholds for primary prevention strategies can be implemented. The trade-off is that one method for calculating risk may not be equally sensitive across all populations or population sub-groups (e.g. the elderly; Cooney et al., 2009).
The aim of this study was to compare the pattern of association among 10 key risk indicators for cardiovascular disease in large representative samples of adults with psychosis and adults from the general community to inform future work on cardiovascular disease risk prediction in those with psychosis.
Methods
Subjects
The Australian National Survey of Psychosis is a population-based prevalence survey with a target population defined by psychosis, place of residence, age range of 18–64 years and contact with public mental health services or relevant non-government organizations (Morgan et al., 2012; Morgan et al., 2014). The study was conducted in 2010 at seven sites across the five mainland Australian states. Sample weights were devised based on age and site and were derived from a census of those in contact with services at each site. Data analysed here are for the 1,457 participants aged 25–64 years with an ICD-10 psychotic disorder. Diagnoses comprised schizophrenia (51.3%, n = 748), bipolar disorder with psychotic features (20.4%, n = 297), schizoaffective disorder (17.8%, n = 260), depressive psychosis (4.9%, n = 71) and delusional disorders or other non-organic psychoses (5.6%, n = 81).
The Australian Diabetes, Obesity and Lifestyle study is a national prevalence survey of diabetes and cardiometabolic risk factors (Dunstan et al., 2002). The target population was defined by place of residence and age 25+. The baseline survey for the study was conducted in 1999/2000 at six clusters within each of the six states and the Northern Territory of Australia. Sample weights were devised based on response rates and coverage of the population within the sampling frame to obtain nationally representative estimates. Data analysed here are for the 8,866 participants aged 25–64 years who completed the baseline survey. This sample serves as our community comparison group. People with known cardiovascular disease were not excluded from either study.
The research protocols for both studies were approved by relevant institutional ethics committees and all participants gave written informed consent. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Measures
The Diagnostic Interview for Psychosis (Castle et al., 2006) was used to determine ICD-10 diagnoses (World Health Organization, 2008) in the psychosis sample. The physical health assessment in each sample included 1) waist circumference, 2) body mass index, 3) systolic blood pressure, 4) diastolic blood pressure, 5) current smoking and fasting 6) plasma glucose, 7) total cholesterol, 8) low density lipoprotein (LDL) cholesterol, 9) high density lipoprotein (HDL) cholesterol and 10) triglycerides (see online supplementary material in Morgan et al., 2014; AusDiab Report, 2000). These variables were selected because they have been used to define the metabolic syndrome (waist circumference, triglycerides, HDL cholesterol, blood pressure, plasma glucose, Alberti et al., 2009) and to predict future risk for cardiovascular disease (e.g. the Framingham, SCORE, ASSIGN, QRISK, PROCAM, WHO-ISH and Reynolds Risk score use various combinations of sex, age, total, HDL and LDL cholesterol, plasma glucose, blood pressure and cigarette smoking status and other variables; see Cooney et al., 2009 for review). In the psychosis sample, among those who currently smoked tobacco, the number of cigarettes or cigar or pipe equivalents smoked daily during the previous four weeks was recorded. In the general population comparison sample, among those who currently smoked tobacco, the number of cigarettes or cigar or pipe equivalents smoked daily was recorded. Where multiple measurements were taken by the Australian Diabetes, Obesity and Lifestyle study only the first measure was used here to match the single measurements taken by the Australian National Survey of Psychosis. All metabolic assays were carried out using quality assured standard enzymatic methods (Morgan et al., 2014; Galletly et al., 2012; AusDiab Report, 2000).
Current prescribed medication use during the past four weeks was recorded based on participant report, with medication chart review for those from the psychosis sample who were in hospital at the time of interview.
Data analysis
Data analysis was undertaken using Stata v13.1. Pearson correlation coefficients, applying each sample’s sampling weights, were used to estimate associations between risk indicators in each sample. Sex and age are potential confounders of strength of association. Correlations were therefore calculated separately for males and females, and partial correlations between indicators, adjusted for age, were also calculated. All bivariate relationships were examined visually, with a loess plot imposed on the data to rule out any substantial deviation from linearity. The analyses were repeated using log transformed and ranked scores (the latter yielding Spearman correlations). As these yielded comparable results to those obtained with untransformed data they are not reported here. The correlation estimated between current tobacco smoking and other risk factors was with the number of cigarettes or cigar or pipe equivalents smoked daily. Those who did not currently smoke were excluded from these analyses. Any observed differences in the pattern of correlation between samples may arise, at least in part, from differences in the dispersion of variables in each sample. Accordingly the robust Levene test (Conover et al., 1981) was used to test for sample differences in the variance of each of the 10 measures of cardiovascular risk examined here.
Results
Sample characteristics
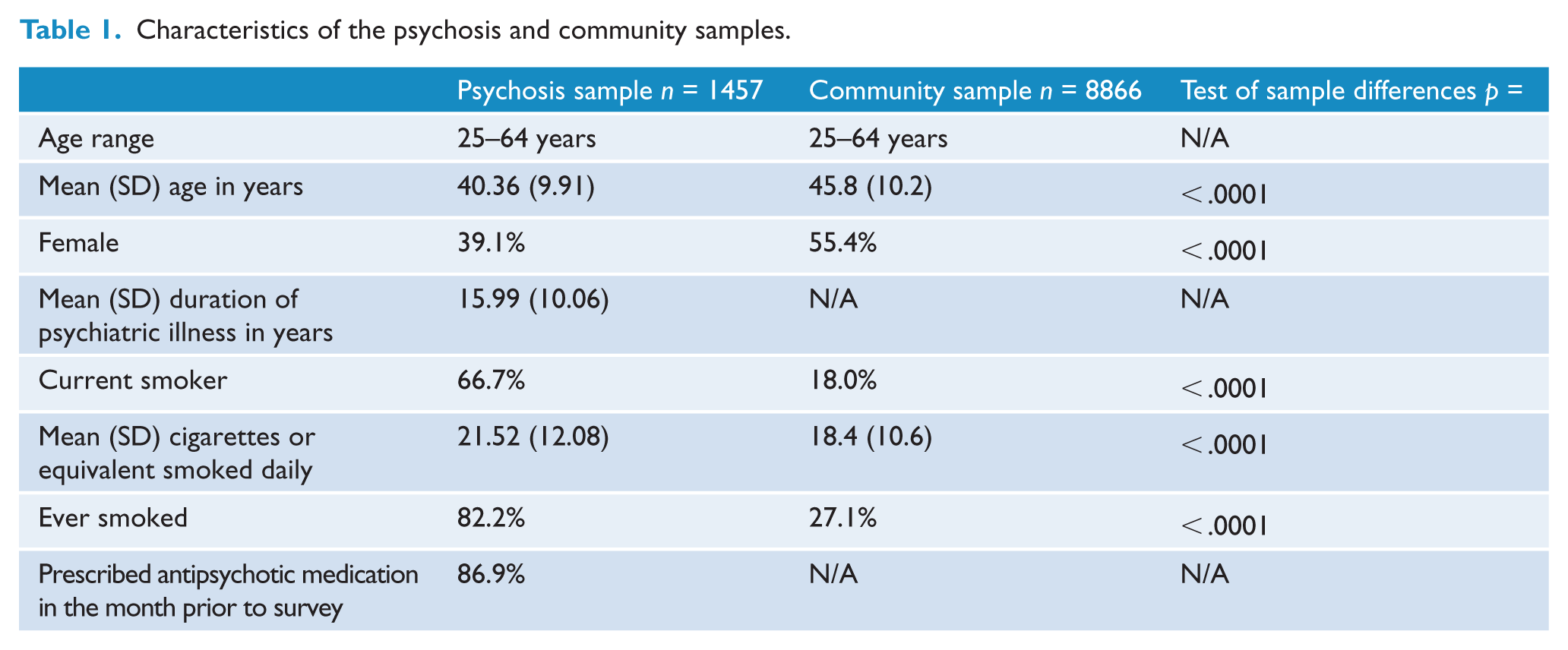
Those in the psychosis sample were more likely to be male and were slightly younger on average than individuals in the community comparison sample (Table 1). Those with psychosis were also 3.7 times more likely to be current smokers and almost nine out of ten had been prescribed antipsychotic medication in the four weeks prior to survey.
Characteristics of the psychosis and community samples.
Differences in the variance of risk factors between samples
Tests for differences in variance between the psychosis and community samples showed that for 20 comparisons – 10 measures examined separately by gender – 13/20 were significantly different (Table 2). The variance for body mass index, waist circumference, fasting total cholesterol, LDL cholesterol, triglycerides and glucose was greater in the psychosis sample than in the community sample for both males and females. Variance of numbers of cigarettes or equivalents smoked daily was greater only for females. The differences were not large and could not account for the difference in the pattern of correlations between samples.
Variance of measures of cardiovascular risk by sample by sex.
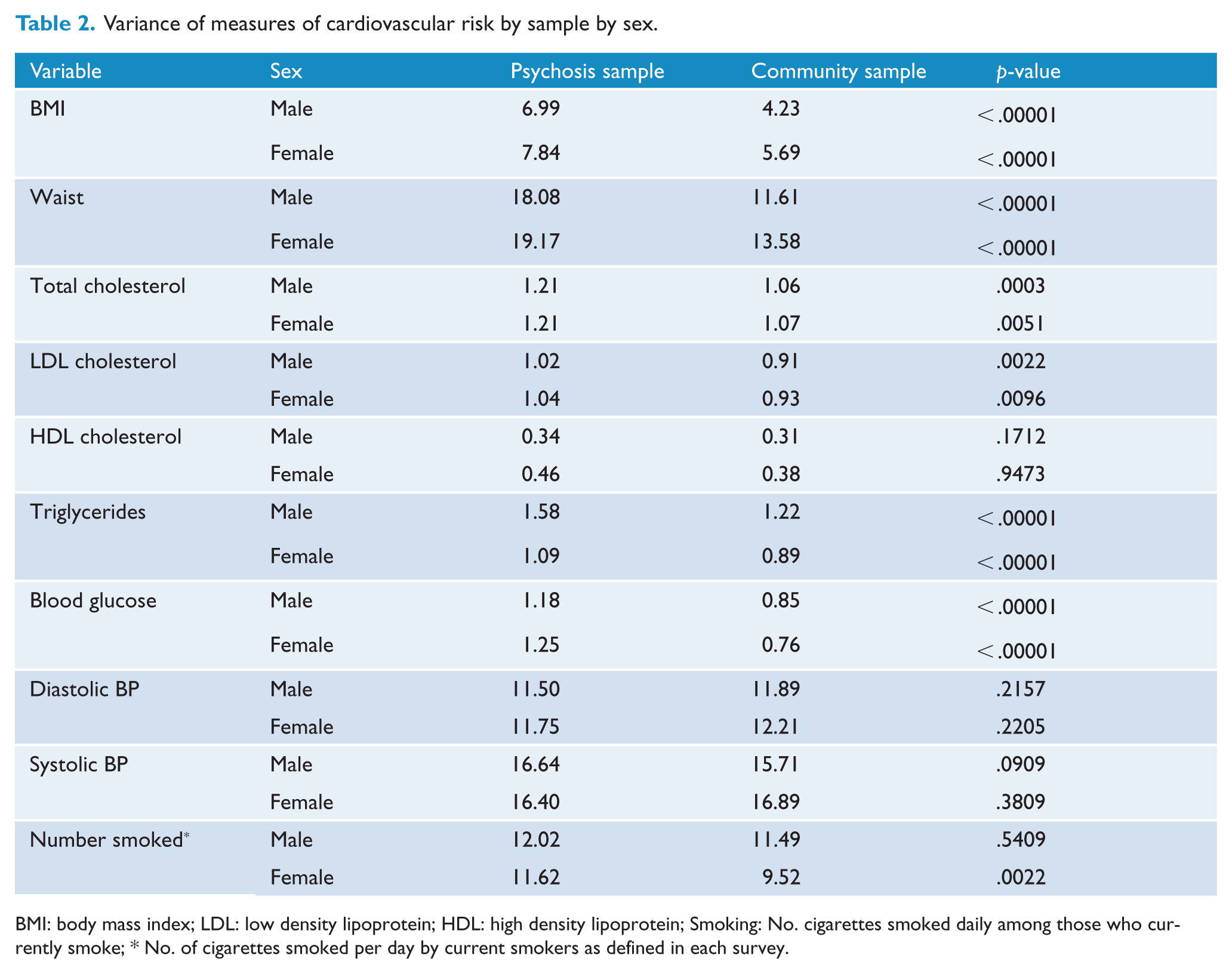
BMI: body mass index; LDL: low density lipoprotein; HDL: high density lipoprotein; Smoking: No. cigarettes smoked daily among those who currently smoke; * No. of cigarettes smoked per day by current smokers as defined in each survey.
Correlations among cardiovascular risk indicators
Almost all correlations in those with psychosis were weaker than in those from the community comparison sample (Table 3). Fifty of 90 correlations between cardiovascular risk indicators were significantly different between samples, with an almost even split by gender, 24 in women and 26 in men. This is approximately 10 times the level expected by chance. Most (39/50) differences were in the 0.10–0.25 range which means that the estimated correlation differed by as much as r = 0.25 between samples; the remainder of the differences (11/50) were r < 0.10. Only the correlation of plasma glucose with triglycerides and diastolic blood pressure with daily level of smoking (in women) was significantly stronger in those with psychosis than in those from the community sample. All other correlations were weaker in those with psychosis.
Correlations among cardiovascular risk indicators by sex in the psychosis and community comparison samples.
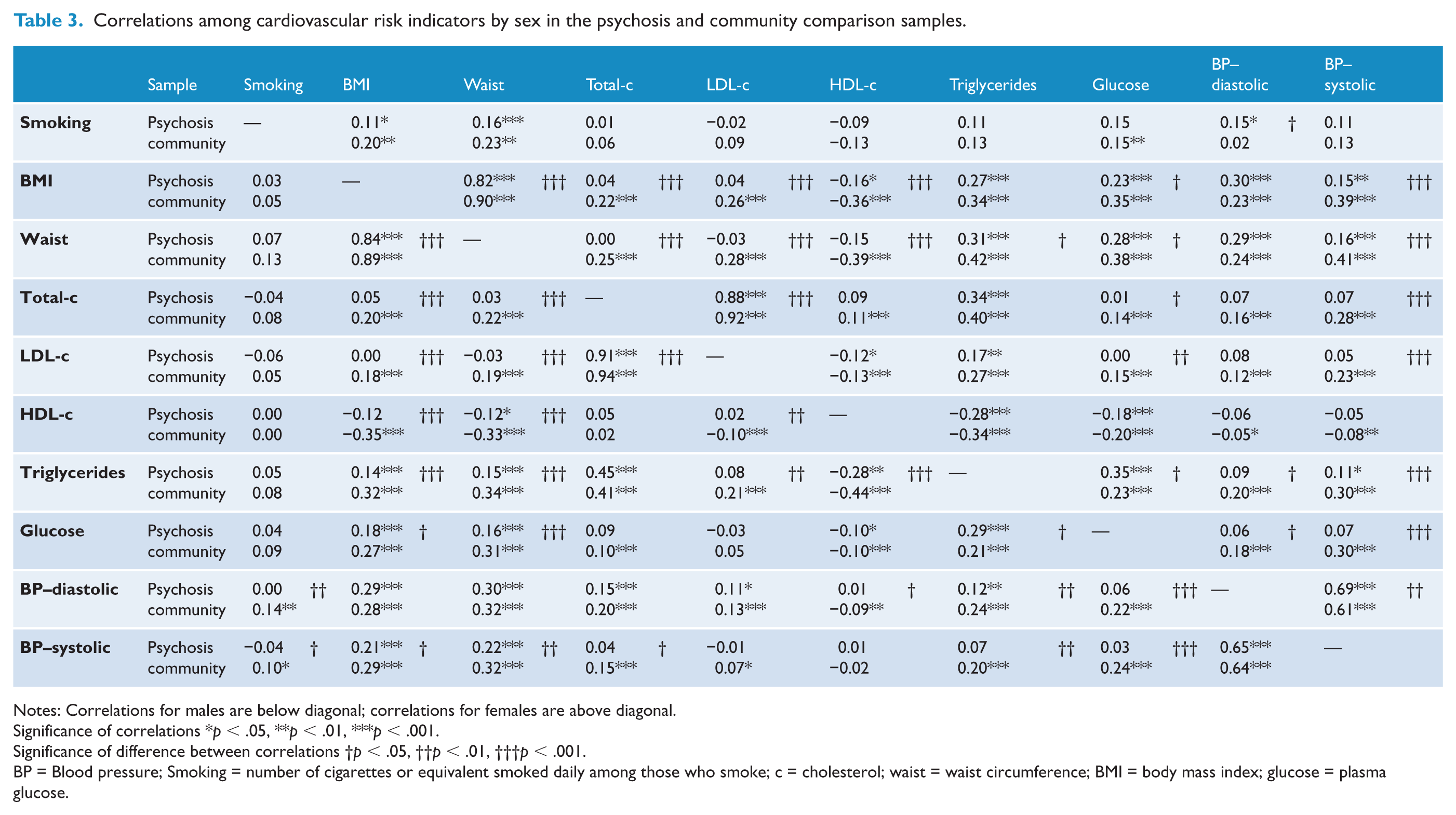
Notes: Correlations for males are below diagonal; correlations for females are above diagonal.
Significance of correlations *p < .05, **p < .01, ***p < .001.
Significance of difference between correlations †p < .05, ††p < .01, †††p < .001.
BP = Blood pressure; Smoking = number of cigarettes or equivalent smoked daily among those who smoke; c = cholesterol; waist = waist circumference; BMI = body mass index; glucose = plasma glucose.
Twenty-eight risk indicator pairs (17/45 in men and 11/45 in women) significantly correlated in the community sample were not correlated in those psychosis. Ten risk indicator pairs were uncorrelated in both men (10/45) and women (10/45) with psychosis: total and LDL cholesterol with BMI, waist circumference, plasma glucose and systolic blood pressure, and plasma glucose with diastolic and systolic blood pressure. Seven risk indicator pairs were uncorrelated only in men with psychosis: the level of daily smoking with systolic and diastolic blood pressure, HDL cholesterol with BMI, LDL cholesterol and diastolic blood pressure, and triglycerides with LDL cholesterol and systolic blood pressure. One risk indicator pair was uncorrelated only in women with psychosis: waist circumference and LDL cholesterol.
Correlation of age with cardiovascular risk indicators
The psychosis and community samples were both aged 25–64 years but the distribution of age within samples was different (Figure 1). Those with psychosis, and especially men with psychosis, were skewed towards the older end of the age range compared with their counterparts from the community comparison sample. An association of age with cardiovascular risk indicators could therefore explain some of the observed differences between samples.
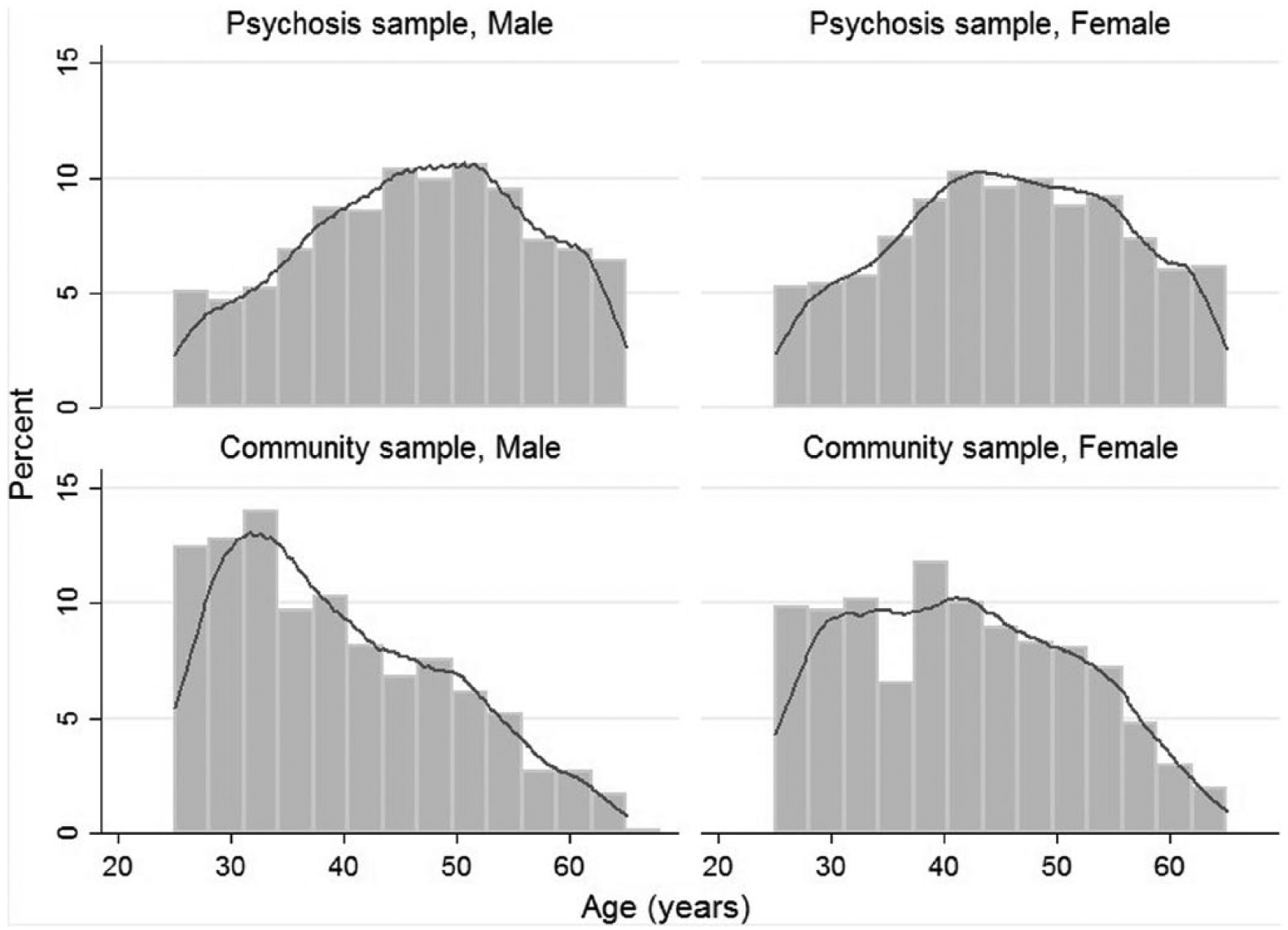
Age distribution by sex of the psychosis and community comparison samples.
HDL-cholesterol was not associated with increasing age in either sample, but all other cardiovascular risk indicators were positively and significantly associated with increasing age in those from the general community (18/20, 9/10 in men and 9/10 in women) (Table 4). Only some cardiovascular risk indicators were positively and significantly associated with increasing age in those with psychosis (11/20, 5/10 in men and 6/10 in women). Fourteen of 20 comparisons between samples were significantly different, 8/10 in men and 5/10 in women. All significant differences between samples were due to a weaker correlation of age with cardiovascular risk indicator in those with psychosis and half of these (7/14) were uncorrelated in those with psychosis. Two risk indicators were uncorrelated with age in both men and women with psychosis, BMI and LDL cholesterol; two were uncorrelated with age only in men, total cholesterol and triglycerides, and one was uncorrelated with age only in women, waist circumference.
Correlation of age with cardiovascular risk indicators by sex in the psychosis and community comparison samples.
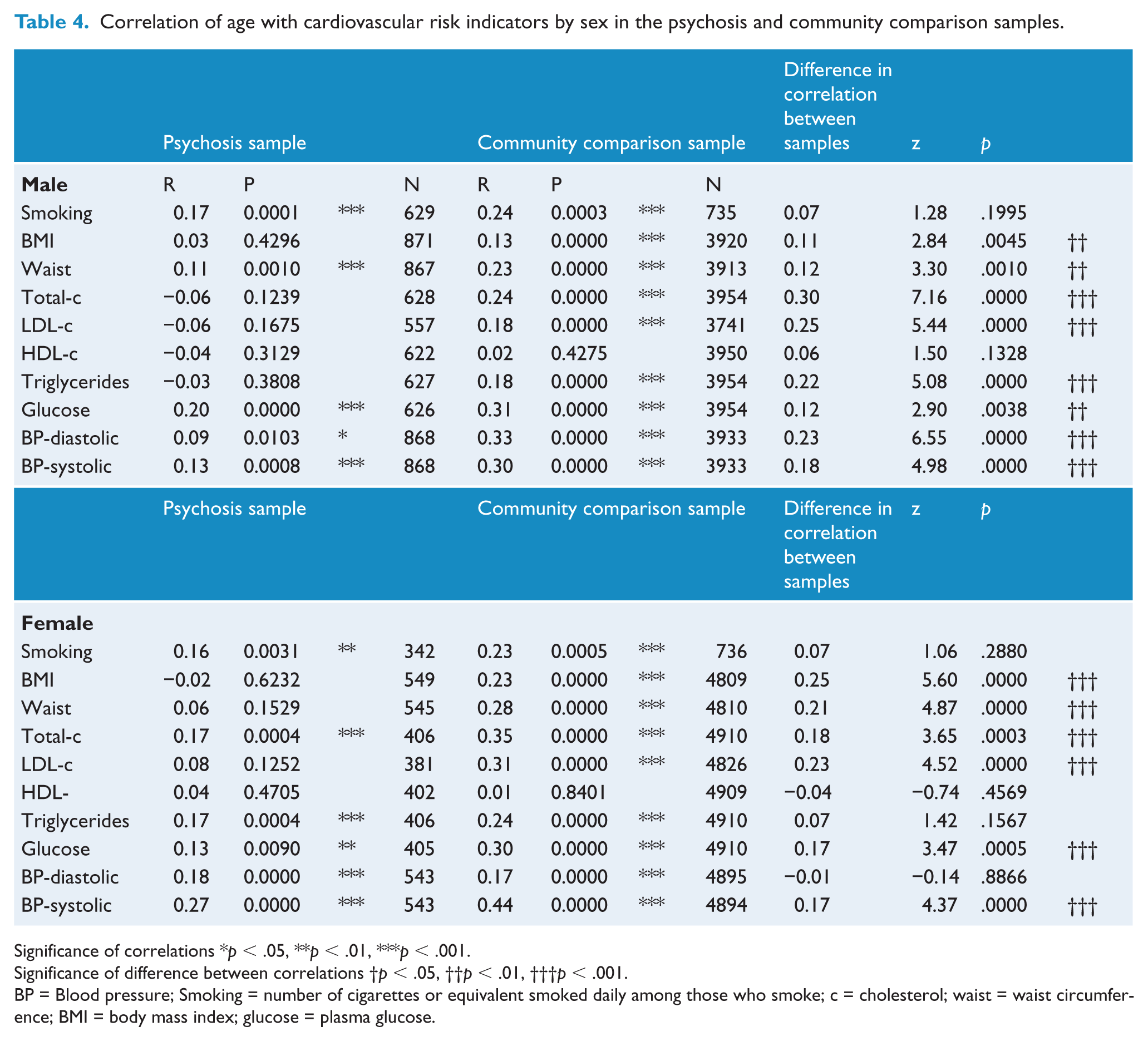
Significance of correlations *p < .05, **p < .01, ***p < .001.
Significance of difference between correlations †p < .05, ††p < .01, †††p < .001.
BP = Blood pressure; Smoking = number of cigarettes or equivalent smoked daily among those who smoke; c = cholesterol; waist = waist circumference; BMI = body mass index; glucose = plasma glucose.
Discussion
Compared with the general population people with schizophrenia are twice as likely to die from cardiovascular disease and their relative mortality risk is increasing because the improvements in health outcomes available to the general population in recent decades are not shared by those with schizophrenia (Saha et al., 2007). The implementation of primary prevention strategies for cardiovascular disease early in the course of psychotic illness is therefore a clinical imperative (see Healthy Active Lives (HeAL) consensus statement, International Physical Health in Youth Stream (iphYs), 2013). To do this effectively we need to know whether methods for predicting future risk and associated primary prevention and treatment strategies for the wider community are applicable for those with psychosis.
We sought in the present study to contribute to that knowledge base by comparing the pattern of association among 10 risk indicators for cardiovascular disease in a nationally representative sample of adults with psychosis to a national comparator sample ascertained to estimate the prevalence of diabetes. The association among risk indicators was often significantly weaker in those with psychosis. Perhaps the most striking finding was the absence of any association between many cardiovascular risk indicators, or between age and cardiovascular risk indicators, that were significantly inter-correlated in our national comparator sample. This could not be explained by statistical artefacts such as restriction of range (variance) in the psychosis sample. One possible explanation is variation in risk factor exposure across samples. To avoid an artefactual difference in duration of exposure to risk factors we restricted our comparisons to the age range that was common to the psychosis and community comparator sample – age 25–64 years. Our previous work has shown that people with psychosis have quite different cross-sectional trajectories of risk factors by age when compared with the community comparator sample (Foley et al., 2013).
Implications for prediction of future risk
The Framingham Heart Study showed that cardiovascular risk factors cluster in the general population and have synergistic effects on the risk for cardiovascular outcomes (Mendis, 2010). Many subsequent studies have validated the Framingham approach to risk prediction (Tzoulaki et al., 2009) but there is no equivalent body of evidence for those with psychosis. The clinical implication of low and absent correlations among cardiovascular risk indicators in those with psychosis is therefore unclear. Weaker associations among risk indicators does not preclude synergist effects on risk for cardiovascular disease but suggests that the weightings for risk indicators in an optimal risk equation for those with psychosis are likely to differ from the weightings derived from general population samples in which these risk indicators are more substantially related. This, in turn, is likely to mean that the rank of importance of targets for intervention may differ substantially for those with psychosis and those in the general population, both at individual and group levels.
Most cardiovascular risk prediction systems include age as an index of exposure time and age is the strongest contributor to the discrimination of virtually all risk calculators (Cooney et al., 2009). The low or absent association of age with multiple cardiovascular risk indicators in those with psychosis compared with those from the general community is therefore noteworthy and consistent with the expression of increased cardiovascular disease risk in those with psychosis from a very early age. In the wider community cardiovascular disease risk indicators worsen with increasing age and associated length of exposure to unhealthy lifestyles, but from at least 25 years of age those with psychosis already have a significantly higher mean BMI, waist circumference, triglycerides, plasma glucose (in women), and diastolic blood pressure and significantly lower HDL-cholesterol than those in the general community (Foley et al., 2013). Those with psychosis are also much more likely to be smoking cigarettes from a very early age (Myles et al., 2012).
A significantly reduced correlation between waist circumference and fasting plasma glucose, triglycerides, HDL-cholesterol and blood pressure in those with psychosis compared with the general population is also relevant for the estimation of the metabolic syndrome. The criteria recommended by the International Diabetes Federation are the presence of an at-risk level of any two of plasma glucose, triglycerides, HDL-cholesterol or blood pressure in those with central obesity. The harmonized criteria are any three of those five risk factors; there is no contingency on central obesity. In our psychosis sample 84% met criteria for central obesity and the prevalence of metabolic syndrome is therefore very similar using either definition. In samples with a lower prevalence of central obesity the prevalence of the metabolic syndrome defined by IDF or harmonized criteria would be more divergent.
Antipsychotic drug treatment
Treatment with antipsychotic drugs is typically instituted early in the course of psychotic illness as part of an active effort to reduce the duration of untreated psychosis (Bhui et al., 2014). It is therefore tempting to attribute the different pattern of inter-correlation among risk indicators for cardiovascular disease in adults with psychosis to the effect of almost ubiquitous antipsychotic drug treatment. However, prospective studies are required to compare the pattern of correlations before and after controlled treatment with antipsychotic drugs. There is a small literature comparing change in predicted cardiovascular disease risk over short time frames stratified by antipsychotic drug received within a randomized controlled trial, but these studies have not assessed participants prior to first exposure to antipsychotic drugs (e.g. Daumit et al., 2008 analysed data from an 18 month randomized control trial of participants with schizophrenia who were randomized to an antipsychotic drug but had already been treated with antipsychotic drugs for an average of 14 years prior to the trial). Outside of short-term randomized controlled trials (Rummel-Kluge et al., 2010), long-term drug treatment of psychosis is often complex and may be altered or discontinued in response to emerging obesity, dyslipidemia, diabetes or client dissatisfaction. A different sampling strategy is therefore required to test the effects of long-term drug treatment for psychosis on risk factor associations. Comparing those with psychosis to age-matched first degree biological relatives who have not been treated with antipsychotic drugs, and who therefore share some of their familial liability for psychosis but not the effects of its pharmacological treatment, would show whether the pattern of correlations observed here is related to risk for psychosis but independent of drug treatment for psychosis. This approach has shown previously that the lower risk for certain cancers in those with schizophrenia is not explained by antipsychotic drug effects (Catts et al., 2008) and an inverse comorbidity with cancer is now known to characterize a range of central nervous system disorders (Ibáñez et al., 2014; Tabarés-Seisdedos et al., 2011; Tabarés-Seisdedos and Rubenstein, 2013). An important caveat is that individuals with psychosis may be exposed to many drugs over their lives, not just antipsychotic drugs, and the totality of drug treatment may also be affecting risk indicator relationships. Those with psychosis here were more likely to be receiving medication for diabetes, hypertension and dyslipidemia than those in the community comparator sample (Foley et al., 2014). Estimating the impact of these medications on the inter-correlations among risk indicators also requires data that has been collected pre- and post-exposure.
Limitations
We compared the inter-correlation among cardiovascular risk indicators in two samples that were surveyed 10 years apart. The last large scale prevalence study of type 2 diabetes in Australia was conducted in 2000, but while the prevalence of certain risk factors has changed over time there is no a priori reason to assume that affects the inter-correlation among predictors. Nonetheless we urge those in other countries with access to large contemporaneous population-based samples of psychosis and the general population that have been screened for type 2 diabetes to attempt to replicate our findings.
We have focused here on a subset of cardiovascular risk indicators that define the metabolic syndrome and which are used in cardiovascular risk prediction equations. Other risk indicators may also differ in prevalence and/or in their pattern of multivariate association with cardiovascular outcomes in those with psychosis and those in the general population. One possible candidate is cannabis abuse, which like cigarette smoking is common in those with psychosis and has been associated with cardiovascular risk (Jouanjus et al., 2014). Additional risk indicators can only be evaluated when longitudinal cardiovascular outcome data is available for testing the performance of current risk prediction equations in people with psychosis.
We analysed BMI and waist circumference but not waist to hip ratio because the psychosis survey did not collect hip measurements. In the general population waist to hip ratio is more strongly associated with risk for cardiovascular disease than BMI or waist circumference (Dhaliwal and Welborn, 2009; Welborn et al., 2003; Yusuf et al., 2005). It is not known if that is true for psychosis. We therefore urge those collecting baseline cardiovascular risk data on large samples of people with psychosis to collect BMI, waist and hip measurements to permit estimation of their inter-correlations with other risk factors and their individual and joint associations with risk for future cardiovascular disease.
The clinical significance of the structure of cardiovascular risk indicators in those with psychosis can be resolved only by connecting the multivariate pattern of risk indicators to their cardiovascular outcomes. Such studies are currently lacking for people with psychosis but are needed to understand the structure of risk factors, to guide treatment decisions and to evaluate if those decisions are changing outcomes. Possible causes of altered risk factor associations and altered associations with age include psychosis itself and medication effects on multiple cardiovascular risk factors. There is also emerging evidence of a direct effect of antipsychotic drugs on risk for myocardial infarction (Lin et al., 2014).
Clinical implications
Risk equations developed to estimate future cardiovascular disease risk in the general population may either not be applicable to those with psychosis or may be relatively inaccurate. This does not mean that individual risk factors should not be treated. However, without longitudinal data connecting different patterns of risk factors to cardiovascular outcomes and the impact of associated treatment recommendation monitored, the priorities for intervention programmes and the means by which total risk may be most effectively reduced is necessarily uncertain. If our focus was simply on what is most prevalent a strong case could be made for focusing on tobacco use and obesity. In the psychosis cohort whose data were analysed here 84% had central obesity and 67% were current cigarette smokers (Galletly et al., 2012). A focus on prevalence is simplistic, however, because prevalence does not equate to the impact of the risk factor or the achievable risk reduction associated with current intervention paradigms. Determining that requires longitudinal multivariate risk and outcome data in large samples of people with psychosis.
Footnotes
Acknowledgements
This publication is based on data collected by the Second Australian National Survey of Psychosis and the Australian Diabetes, Obesity and Lifestyle study. The members of the Australian National Survey of Psychosis Survey are: V. Morgan (National Project Director), A. Jablensky (Chief Scientific Advisor), A. Waterreus (National Project Coordinator), R. Bush, V. Carr, D. Castle, M. Cohen, C. Galletly, C. Harvey, B. Hocking, A. Mackinnon, P. McGorry, J. McGrath, A. Neil, S. Saw, H. Stain. We acknowledge, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication. For their invaluable contribution to the set up and field activities of the Australian Diabetes, Obesity and Lifestyle study we are grateful to A. Allman, B. Atkins, S. Bennett, S. Chadban, S. Colagiuri, M. de Courten, M. Dalton, M. D’Emden, D. Dunstan, T. Dwyer, D. Jolley, I. Kemp, P. Magnus, J. Mathews, D. McCarty, A. Meehan, K. O’Dea, P. Phillips, P. Popplewell, C. Reid, A. Stewart, R. Tapp, H. Taylor, T. Welborn, F. Wilson and P. Zimmet. Finally, our thanks go to the local collaborating centres, including Sir Charles Gairdner Hospital (WA), the Prince of Wales Hospital (NSW), the Menzies Centre for Population Health Research (TAS), the Queen Elizabeth Hospital (SA), the Menzies School of Health Research (NT), Queensland Health, the Monash Medical Centre Department of Nephrology (VIC), and the Centre for Eye Research Australia (VIC).
Funding
The Second Australian National Survey of Psychosis study was funded by the Australian Government Department of Health and Ageing. The Australian Diabetes, Obesity and Lifestyle study was funded by the then Commonwealth Department of Health and Aged Care, Eli Lilly (Aust) Pty Ltd, Janssen-Cilag (Aust) Pty Ltd, Abbott Australasia Pty Ltd, Merck-Lipha s.a., Alphapharm Pty Ltd, Merck Sharp & Dohme (Aust), Roche Diagnostics, Servier Laboratories (Aust) Pty Ltd, SmithKline Beecham International, Pharmacia and Upjohn Pty Ltd, BioRad Laboratories Pty Ltd, HITECH Pathology Pty Ltd, the Australian Kidney Foundation, Diabetes Australia (NT), Queensland Health, South Australian Department of Human Services, Tasmanian Department of Health and Human Services, Territory Health Services, Victorian Department of Human Services and the Health Department of Western Australia. The work is supported in part by the Victorian OIS scheme. John McGrath has received support from the National Health and Medical Research Council John Cade Fellowship APP1056929. Jonathan Shaw is supported by a National Health and Medical Research Council Senior Research Fellowship (APP526609). Debra Foley acknowledges the support of the Colonial Foundation (Australia) to the Orygen Youth Health Research Centre.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.