
Abstract

Morris et al. recently published data suggesting that more than half of potassium results >6.0 mmol/L in specimens from primary care were due to pseudohyperkalaemia. 1 Furthermore, they found that, for potassium results >6.5 mmol/L, an estimated Glomerular Filtration rate (eGFR) of ≥90 mL/min/1.73 m2 gave a negative predictive value (NPV) of 100%, that is, true hyperkalaemia was not associated with normal renal function. Given the implications these findings for current practice, especially the telephoning of results by laboratory staff to out-of-hours services, we sought to reproduce this study in our own patient population. Potassium and creatinine were measured on an Abbott Architect analyser, with creatinine being measured using an enzymatic assay. Glomerular Filtration rate (GFR) was estimated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.
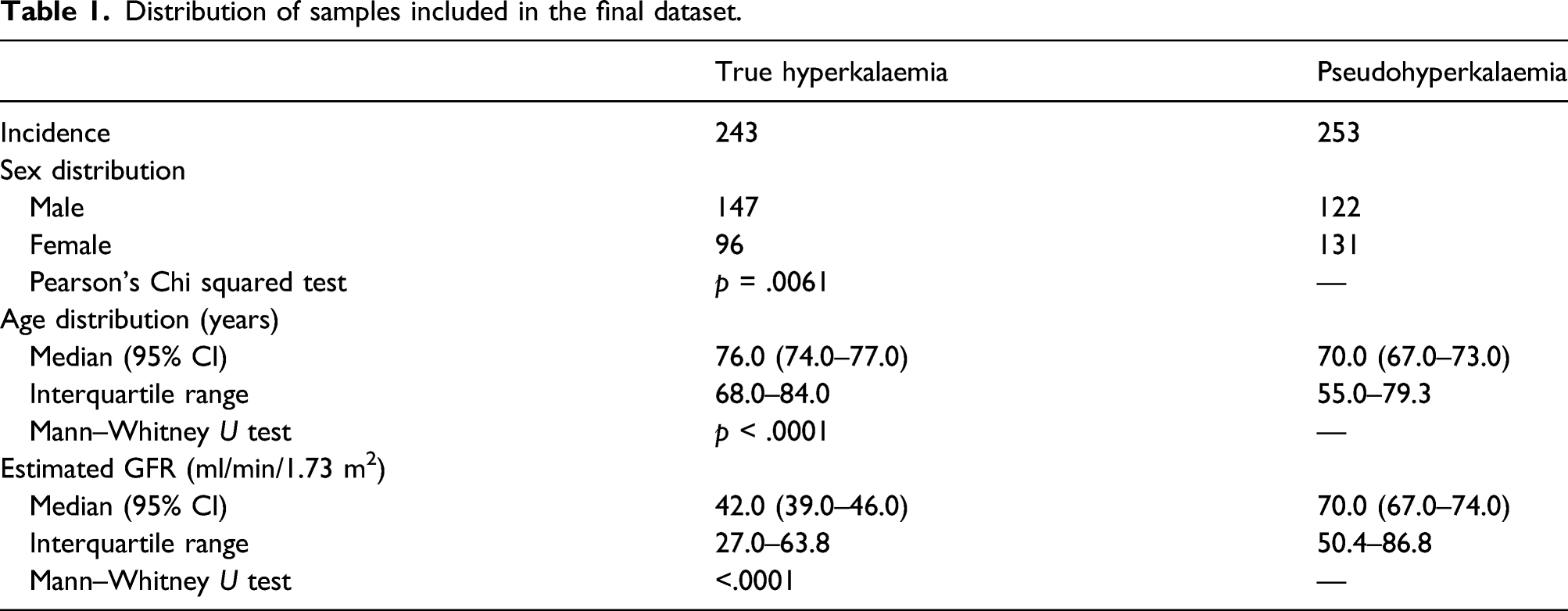
Distribution of samples included in the final dataset.
As also observed by Morris et al., true hyperkalaemia was associated with reduced eGFR. We found that for initial potassium results >6.0 mmol/L, eGFR ≥90 mL/min/1.73 m2 had an NPV of 72%; this increased to 83% when only initial potassium results of ≥6.5 mmol/L were included, and to 100% when only those samples with initial potassium ≥6.5 mmol/L and concomitant normal full blood count (FBC) were included. However, analysis of the receiver operating characteristic (ROC) curves using the DeLong et al. method 2 showed that there was no statistically significant benefit to considering the FBC, in line with the findings of Morris et al. 1
Overall, our findings support those of Morris et al. Together, these studies show in a large dataset that true hyperkalaemia is not associated with normal renal function (eGFR ≥90 mL/min/1.73 m2). Our data also show remarkably similar rates of pseudohyperkaemia, of approximately 50%. This is a significant proportion of high potassium results, so being able to better identify true hyperkalaemia could have a large impact on how we communicate these results.
Morris et al. suggested that there is no need to telephone potassium results ≥6.5 mmol/L to out-of-hours primary care providers if eGFR is ≥90 mL/min/1.73 m2, and that such results can be safely telephoned the next working day. They suggest that this would not only reduce unnecessary calls to the out-of-hours service provider and subsequent patient anxiety, but that it also provides a potential economic benefit from reduced emergency department attendances. Given that our NPV is not 100%, there is a risk that some cases of true hyperkalaemia may be missed. However, this would be mitigated by telephoning the results the next working day.
The protocol of Morris et al. was followed closely to allow direct comparison of data. An exception is that we do not report potassium results on samples more than 8h old; the cutoff Morris et al. applied was 6 h. However, this difference did not appear to affect the observed rate of pseudohyperkalaemia. Overall, our study extends the findings of Morris et al. These findings have important implications for urgent communication of high potassium results more widely, and may merit consideration in the Royal College of Pathologists’ critical results communication guideline. 3
Footnotes
Acknowledgements
We would like to thank Thomas Morris for his help and guidance in recreating this study. With thanks to Edmund Lamb for helping to edit the final daft.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
SS.
Contributorship
EB organised data analysis and drafted the initial manuscript. DL assisted with data collection and SS helped to design the study. All authors reviewed and edited the manuscript and approved the final version.