
Abstract
Background
The growing number of laboratory investigation requests is placing an increased burden upon NHS resources. Around a quarter of all tests are unnecessary repeats, and almost a third have no impact on patient management. Doctors recognise that tests should only be performed when clinically indicated, but a culture persists of undertaking unnecessary repeat investigations.
Methods
A cohort study was undertaken at a district general hospital to observe the impact of introducing educational interventions in the form of a poster and a series of educational lectures, encouraging clinicians to consider whether an investigation was clinically indicated. Data was collected from nine different sites across the hospital run by different medical teams regarding the number of tests undertaken and the impact on patient care.
Results
Data from over 13,000 tests and over 2000 patients was analysed from nine different sites across the hospital. There was a significant reduction (33%, p = 0.0001) in the number of blood tests performed. This reduction in testing saved £7006 over the course of 1 month, in addition to other benefits. There was a reduction in testing in eight out of the nine sites in which the study was undertaken, demonstrating good generalisability of results. There was no significant increase in length of admission or mortality.
Conclusion
Educational interventions to doctors have a significant and safe impact in reducing the number of unnecessary investigations, providing cost saving benefits to the NHS.
Introduction
Undertaking laboratory investigations is placing an increasingly large burden upon the NHS in a period when budgets are being stretched. Over a billion tests are run by hospital pathology laboratories each year, costing the NHS around £2.2 billion. 1 The Carter Review into pathology services within England found that the number of tests being performed is increasing at around 10% per year. 2 Furthermore, this report found that approximately a quarter of all tests were unnecessary repeats. 2 Overall, it has been reported that only 32.1% of investigations are considered to have made an impact upon patient management. 3
There are several reasons as to why unnecessary tests may be undertaken. These include physicians being unaware of the costs associated with tests, lack of education regarding benefit and harm of tests, practising defensive medicine, and the culture of the hospital. 4 Although there is acceptance amongst doctors that tests should only be performed due to clinical need, a culture of performing ‘daily bloods’ persists in many hospitals. 5
The issue of excessive laboratory tests has been appreciated by physicians across the globe, with promising results from a few different approaches to reducing unnecessary testing. These have included requiring senior oversight when requesting bloods, unbundling test panels, distributing flyers and providing lectures to staff.4–7 Within the UK, the Royal College of Pathologists have also issued guidance on minimum retest intervals in an effort to reduce unnecessary repeat tests. 8
On the general medical wards at the Royal Bolton Hospital, around 7500 blood tests are undertaken each month. These tests are performed by either phlebotomists or trained staff on the ward. Tests that are taken by the phlebotomists are requested by the ward doctors the previous day using the electronic request system. If the patient requires blood tests on the day or the phlebotomists are unsuccessful, ward clinical staff undertake them.
Methods
Study design and setting
This study is a primary analysis of quantitative data, gathered through information provided by the medical records department at Royal Bolton Hospital, a district general hospital in the north-west of Greater Manchester. The objective of the study was to determine whether undertaking an educational lecture and producing informational posters could reduce the number of blood tests performed. The study was undertaken in nine different sites within the hospital. Data were collected regarding the number of blood tests undertaken on medical wards throughout the hospital over a given month prior to interventions and in the month following interventions.
Data collection
The medical records department at the hospital provided a list of all medical inpatients from 1 June 2018 to 30 June 2018 (inclusive). A proforma was then used to collect information on how long each patient was in hospital, whether the patient had died during their stay, and how many medications they were discharged with. The hospital’s pathology reporting system (ICE) was used to obtain the number of blood tests undertaken during this time period for each ward. Following the implementation of interventions, the same data were gathered for the second cohort of patients between 1 November 2019 and 30 November 2019 (inclusive). The same medical wards were used in both groups. In total, the data from 13,063 blood tests and 2029 different patients were analysed. The cost of each of the 140 different types of blood tests undertaken was also obtained from the medical records department to assist in the cost analysis of this study.
Statistical analysis
Using Graphpad Prism 8.0, a Shapiro–Wilk normality test was carried out to determine normality, the correlating analysis is stated with each result. Data are stated as mean +/− standard deviation (SD), and statistical significance was established at p < 0.05 probability.
Interventions
The first intervention that was implemented was an informative poster (Figure 1) to remind clinicians to consider whether the test they were ordering was clinically indicated. This was deemed to be the most important information to give to lower inappropriate testing, as doctors tend to agree that undertaking tests when not clinically indicated is not correct practice.
5
The medium of a poster was used as it was cost-effective and could not be ignored (as emails or information on the intranet might be). Furthermore, a previous similar study that used flyers to disseminate information to reduce inappropriate testing had good efficacy.
4
‘Think before you tick’ poster.
The second intervention that was implemented was a series of 15-min educational lectures to junior doctors at the trust to encourage them to consider whether a test was appropriate (Figure 2). In this lecture, the information on the poster was re-iterated. However, additional information was also delivered, such as the pros and cons of undertaking tests as well as the cost of each test. This information has also been shown to be effective in improving duplicate investigations,
6
but were not included within the poster to avoid overwhelming the audience with too much information. Presentation from educational lecture.
Results
Patient demographics
As shown in Figure 3, in the pre-intervention cohort, a total of 1018 patients were spread across the medical wards, with an average age of 70.28 +/− 17.59 years. In the post-intervention cohort, there were a total of 1011 patients, with an average age of 69.45 +/− 18.11 years. No significant difference was found between the two groups (Mann–Whitney, p = 0.295). The age of patients in each cohort.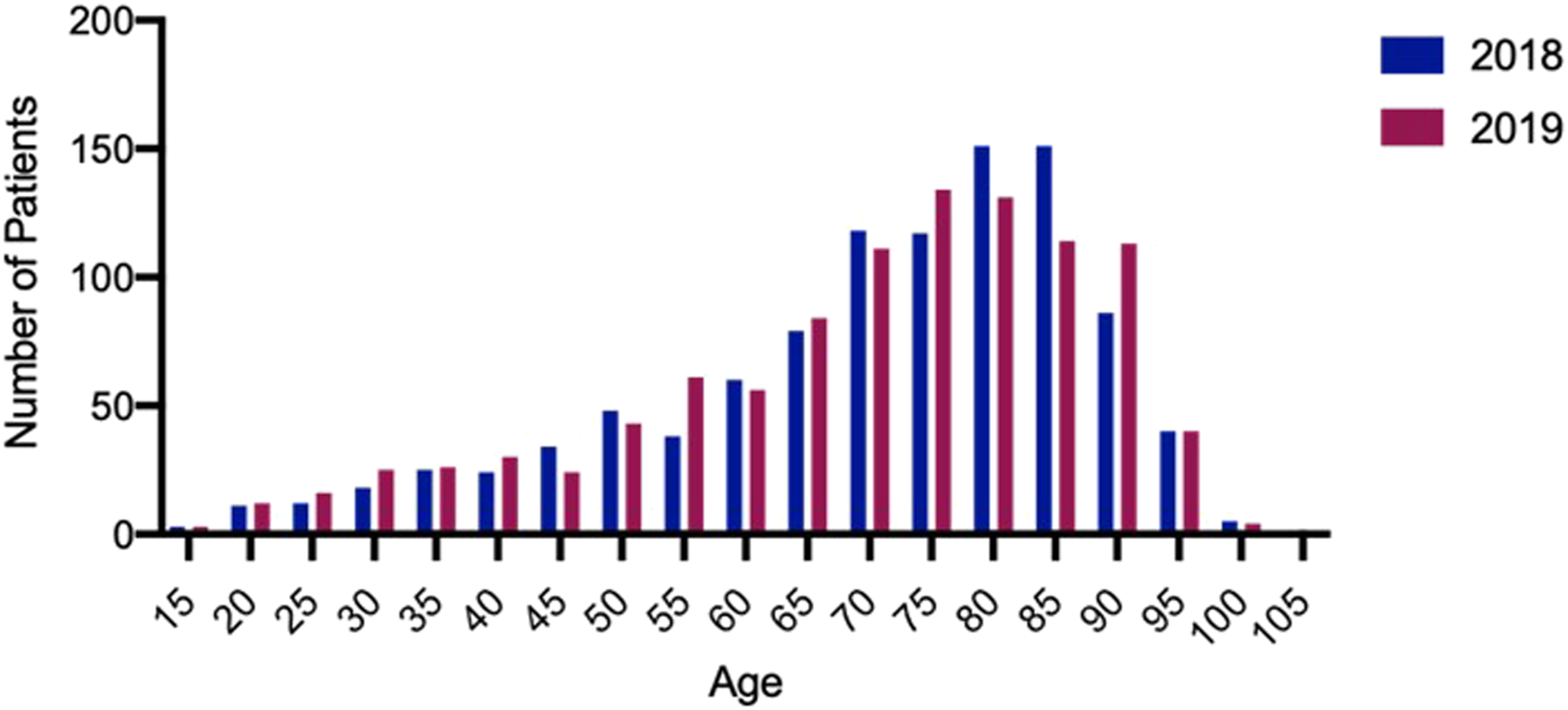
Clinical outcomes
Patients had a mean length of stay of 6.06 (SD = 6.26) days in the pre-intervention cohort and 5.69 (SD = 6.42) days in the post-intervention cohort (Figure 4), a significant decrease between the two cohorts (Mann–Whitney, p = 0.0296). The number of ward days in each cohort.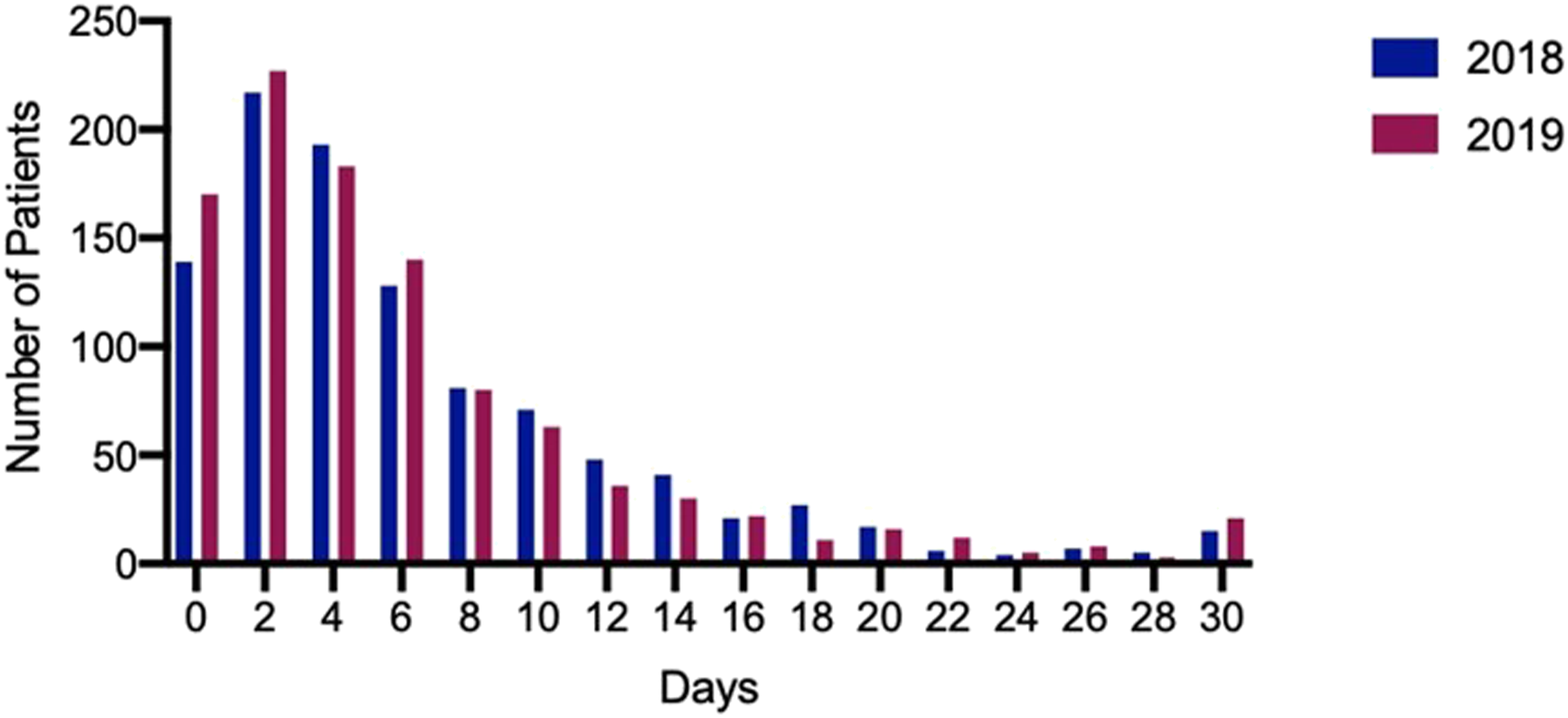
Finally, mortality in the pre-intervention cohort was 9% and in the post-intervention cohort was 9%, with no significant difference between the two groups (Chi-square, p = 0.565).
Blood test results
Two sample paired t-test analysing number of blood tests performed.
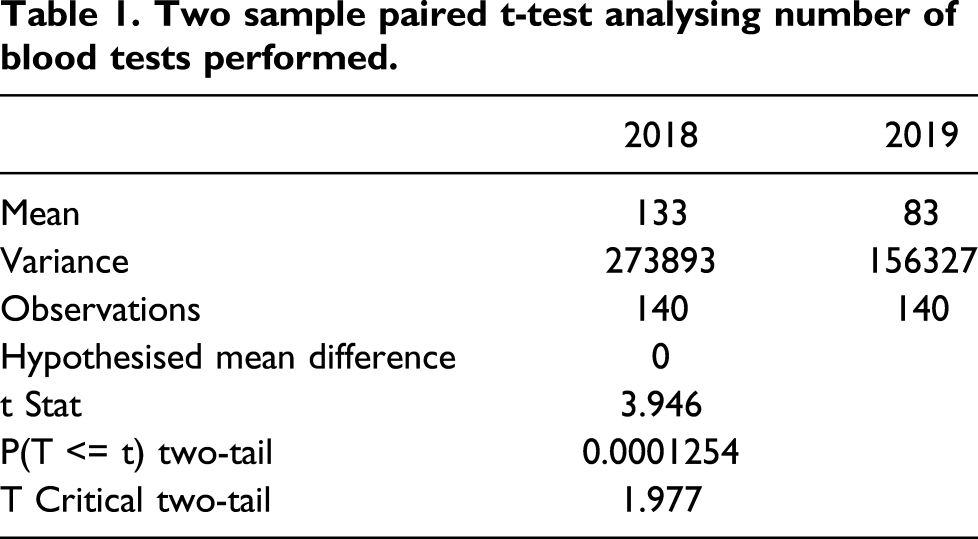
Across the nine different sites in which the study was undertaken, there was a reduction in blood testing in eight sites and an increase in the remaining site. These eight sites had a reduction of between 30% and 54%, and the remaining site had an increase of 13% (see Figure 5). The single site that had a 13% increase in tests also had 53% more patients in the post-intervention cohort, which may have contributed to the anomalous result. In total, there was a 33% reduction in blood testing across all sites. Change in number of blood tests across sites following interventions.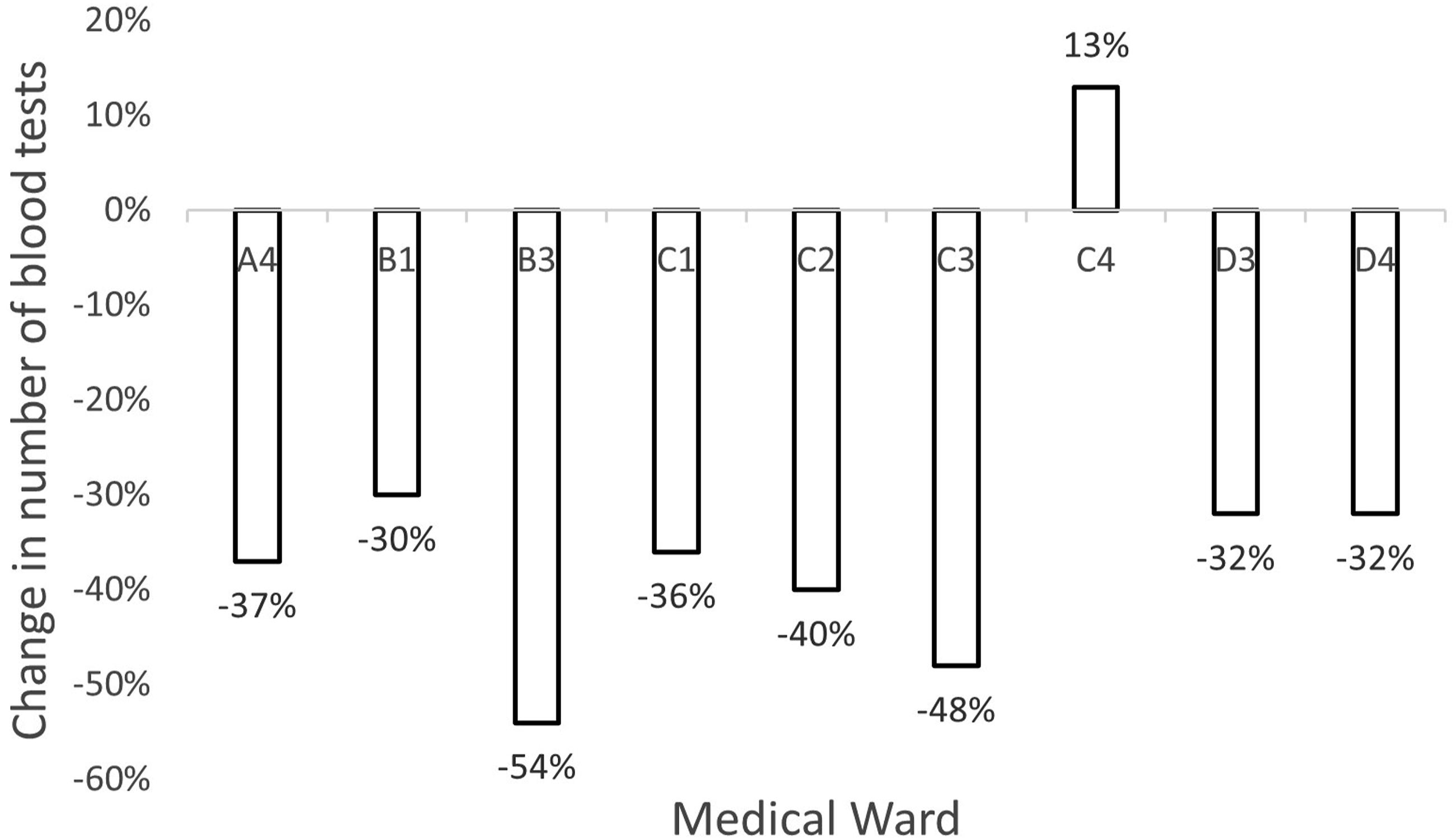
Cost savings
A breakdown of cost per test was obtained from the medical records department. The total cost of blood tests in June 2018 was £18,626.81, and in November 2019 was £11,620.75. In total, there was a £7006.06 (37.6%) reduction in costs between the 2 months.
Limitations
There were three main limitations of this study. Firstly, different months were selected for analysis between the 2 years of the study (June 2018 and November 2019). The month selected for the pre-intervention cohort analysis (June 2018) was chosen from the previous year. This was selected as the planned intervention was scheduled to launch in May 2019 (with data collection planned for June 2019); however, this was delayed to September and October 2019 and therefore post-intervention data were collected for the subsequent month of November 2019. This limitation was mitigated by ensuring that the post-intervention month chosen had the same number of days, and by ensuring there was no significant difference in the number or demographics of patients included. Secondly, it is noted that there would have been a slight change in cohort of junior doctors working at the hospital between these dates: however, this factor is unlikely to have caused the sustained reduction in testing across sites observed in this study. Finally, a third cycle the following year to assess whether reductions were sustained was planned for June 2020; however, this was not possible due to the COVID-19 pandemic, which drastically altered the number of inpatients and demographics of patients in the hospital. It is anticipated that when new junior doctors rotate onto positions at the trust the impact of interventions would be reduced, and therefore including the presentation and continued educational activities during local inductions will be necessary to sustain reductions.
Discussion
The increasing burden of unnecessary laboratory investigations was highlighted by the Carter review in 2006. However, this study demonstrates that the issue of unnecessary testing is still prominent. Simple interventions of negligible cost encouraging clinicians to consider whether tests were clinically indicated were able to reduce associated costs by 37.6%. There was no significant increase in both mortality or length of stay, demonstrating that this reduction in laboratory tests has been a safe one. Furthermore, the high number of data points analysed and the concordance of results across eight out of the nine sites demonstrates the validity and generalisability of these results.
There are many advantages of reducing unnecessary tests beyond simply saving money. It can improve patient satisfaction by reducing discomfort and reducing interrupting sleep for early morning bloods. From a medical perspective, it reduces the risk of infection and iatrogenic anaemia. Finally, it reduces workload on staff having to take the bloods, analyse them in the laboratories, and reviewing results.
If this cost saving was extrapolated out over a year, it would represent a saving of over £84,000 for the hospital.
Conclusion
Encouraging doctors to consider whether testing is clinically indicated (in the form of a poster and short lecture) led to a safe and significant reduction in the number of blood tests ordered, with the potential for large annual savings.
Footnotes
Acknowledgments
Acknowledgments go to the Royal Bolton Hospital for helping undertake this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
not applicable
Guarantor
MT
Contributorship
MT researched literature, collected data, delivered the educational lecture and wrote the first draft of the manuscript. HC and MW developed the informational poster and collected data. MW and AB undertook data analysis. AB led the conceived the project, collected data and managed the project. All authors reviewed and edited the manuscript and approved the final version.