
Abstract
Background
Unnecessary blood tests are estimated to contribute to 25% of wastage in the National Health Service. The aim of this study was to assess the financial implication of clinical need-focused blood tests guided by a senior clinician in a district general hospital.
Methods
We conducted an observational longitudinal study over six months with pre- and postanalysis of a vetting intervention. A colorectal firm (Team A) implemented a vetting system that required a registrar or consultant to discuss which blood tests needed to be requested for each in-patient with junior doctors. Another colorectal firm (Team B) with a similar caseload was blinded to the study and was used as a control.
Results
The vetting initiative demonstrated a reduction of 33% of blood test requests, translating to a cost-saving of £2406 over three months. Following the intervention, the median number of tests requested per patient per day by Team A for C-reactive protein reduced from 0.8 to 0.63 (P = 0.0074), full blood counts reduced from 0.8 to 0.67 (P = 0.0138), liver function tests decreased from 0.8 to 0.6 (P = 0.0021) and urea and electrolytes fell from 0.8 to 0.63 (P = 0.0083). The number of tests per patient per day after the intervention was significantly less than the control group (P < 0.001). The length of hospital stay and admission to critical care were not adversely affected in the group that had less blood tests, P = 0.808 and P = 0.58, respectively.
Conclusion
The direction, by a senior clinician, of the requesting of blood tests by junior doctors to ensure that requests were based on clinical need, reduced the number of inappropriate blood tests and resulted in some reduction in laboratory costs.
Introduction
Laboratory pathology investigations cost the National Health Service (NHS) £2.5 billion per year in the United Kingdom (UK). 1 The Carter Review, a UK Department of Health commissioned review of pathology services in England, identified that 25% of pathology tests were unnecessary resulting in considerable wastage. 2 Several studies indicate that unnecessary tests account for between 25% and 40% of laboratory workload. 3 Miyakis et al., 4 reported up to 68% of tests performed in a medical department were not considered to have contributed towards management of patients.
Blood test requests are rising at a rate of 8% to 10% each year. 5 Clinical laboratories are under increasing pressure to reduce costs and increase efficiency in pathology services. 5 Several strategies to reduce unnecessary testing have been tried. 5 Prelaboratory measures include educational interventions for example face-to-face sessions, data feedback, report-linked information, educational bulletins and guidelines. 5 Educational strategies have reduced the volume of test requests in pre- and postintervention study designs and some randomized controlled trial studies; however, the effect is variable. 5 The impact of education may be limited due to the regular changeover of clinical staff. Within-laboratory strategies include automatic re-test rejection rules for specific tests if requested within a user-defined time window. 5 A national consensus document on recommendations for minimum re-test intervals for pathology tests has recently been published. 6 However, minimum re-test interval rules are not ideal in the acute setting as the test interval is very dependent on the clinical state of the individual patient and the results of previous investigations. 5 There is currently a lack of evidence for minimum re-test intervals, and their impact on clinical and patient outcomes. 5 Postlaboratory methods include review of the impact of the test results by the requesting clinical teams. However, the practicality of assessing this is challenging. 7
In the General Surgery Department at our district general hospital, the requesting, checking and acting upon blood tests is primarily the role of junior doctors ranging from foundation year 1 level to core surgical trainees. All blood tests are requested and viewed electronically, and the laboratory generally accepts all routine and urgent blood test requests irrespective of the grade of the requestor. It is possible that junior doctors request more tests, and that they request such tests more frequently than is necessary, out of fear of failing to request a test that a senior member of the team may later ask about. This problem may be compounded by anxiety associated with working in a new team every four to six months, after which period junior doctors generally changeover in the UK. The aim of this study was to assess the impact of implementing a vetting system, led and directed by a senior clinician, on the requesting practice of junior doctors and any possible financial impact this could have.
Methods
Study design
We conducted a longitudinal observational study to examine the blood test requesting pattern of one colorectal firm, Team A, over a three-month period from June to August 2014. As part of a quality improvement project aimed at reducing unnecessary and repetitive blood tests on patients, a vetting protocol was implemented by Team A.
After five months of following the vetting protocol, the number of blood tests requested by Team A was re-audited for three months from February to April 2015. The blood test requesting behaviour of another colorectal firm (Team B) was also observed during the same re-audit period. Team B was blinded to the study and the vetting protocol. The patient cohort under the care of Team B served as a control group for comparison.
Vetting protocol
The senior clinicians in Team A were involved in the conception of this study, and all had agreed to integrate a vetting protocol into their routine clinical practice. The protocol involved reviewing the patient at the daily morning ward round. The senior surgeon in the team, either registrar or consultant, made a decision on whether to bleed the patient and which tests to request for the following day based on clinical need. This decision was personalized to the individual patient by considering several clinical factors such as previous results of blood tests and other investigations, the need to monitor the response to treatment, to correlate their clinical and laboratory findings and to assess disease severity and clinical progression.
The senior clinician discussed with the junior doctors which blood tests to request and briefly explained the rationale behind their decision. This discussion took place at the bedside at the same time as the senior clinician informed the junior doctors of the management plan for the patient. This process was repeated for each patient on the ward round. The junior doctors requested blood tests using an electronic ordering system. The test requesting was linked to the phlebotomy service, which conducted phlebotomy rounds once a day.
Data collection
The data were collected retrospectively from a database of serial measurements of inpatients’ blood results. This database was in the form of multiple electronic tables on the ward patient handover list, which was used by the clinical team to keep a daily record of their in-patients. Junior doctors compiled the dataset prospectively as part of usual clinical practice for all admitted patients. In this study, the following blood tests were evaluated: C-reactive protein (CRP), full blood count (FBC), liver function tests (LFTs) and urea and electrolytes (U&E). These blood tests were selected because they were perceived to be the highest volume of tests ordered by colorectal teams, and the database that was used for data collection was predesigned to contain these specific items only.
Since the blood test requests were retrospectively obtained from the ward list as the primary means of data collection, the dataset was validated to ensure it was complete. Validation was performed by cross-referencing blood tests recorded on the ward list with the online record of blood test requests on the electronic pathology ordering software. The software contained a historical trail of test requests for each patient.
Inclusion criteria were consecutive emergency and elective surgical admissions. Exclusion criteria included day-case elective procedures and 23-h admissions. These patients were excluded because the short hospital stay would not have yielded sufficient data to determine the blood test requesting behaviour of the clinical team. Patients transferred from other specialties were also excluded because the blood test requesting pattern would have been confounded by other clinical teams’ decisions.
Patient demographics including gender, date of birth, elective or emergency admission, length of stay and admissions to acute surgical care unit (ASCU) or critical care unit (CCU) were collected from two data sources, the electronic patient ward list and blueberry in-patient management system (BIMS), an electronic data system storing details of the patients’ admission and discharge.
Data analysis and statistics
The outcome measures included total number of test requests, median number of requests per patient per day and cost-saving. The cost-saving of the intervention was determined by the difference in the number of tests requested by colorectal Team A between the first and second cycles. This calculation was based on the NHS price for blood tests, which pertained to the cost of laboratory reagents. Our hospital laboratory informed us of the following costs: CRP – £1.43, FBC – £2.67, LFT – £9.88, and U&E – £2.20.
Statistical analyses were performed on GraphPad Prism 5.0 and Microsoft Excel 2007. Inpatient length of stay was analysed using the Kruskal–Wallis test. Admissions to ASCU or CCU were compared by Chi-square analysis. The differences in number of tests per patient per day between groups were calculated using the Mann-Whitney U test.
Results
Patient demographics
Demographic details of sample populations.
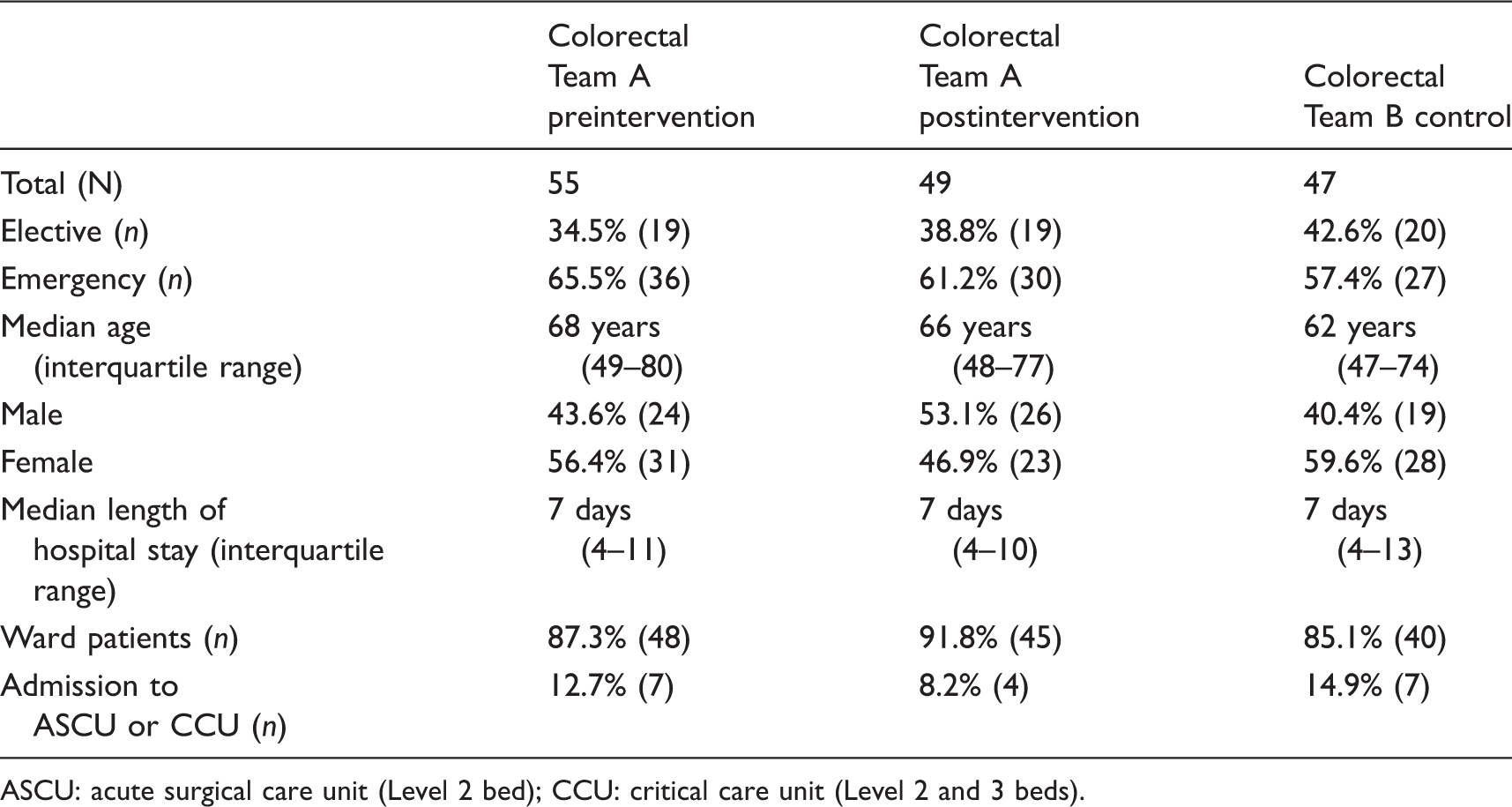
ASCU: acute surgical care unit (Level 2 bed); CCU: critical care unit (Level 2 and 3 beds).
The median length of stay for patients in all three groups was seven days, and there was no significant difference between groups (P = 0.808). There was no significant difference in the proportion of patients admitted to ASCU or CCU between the three groups (P = 0.58).
Test requests
Following the vetting intervention, the median number of tests requested per patient per day by Team A for CRP reduced from 0.8 to 0.63 (P = 0.0074), FBC reduced from 0.8 to 0.67 (P = 0.0138), LFT decreased from 0.8 to 0.6 (P = 0.0021) and U&E fell from 0.8 to 0.63 (P = 0.0083). The median number of tests requested per patient per day by Team A after the intervention were significantly less than the control group Team B for CRP (P = 0.0003), FBC (P = 0.0005), LFT (P = 0.0003) and U&E (P = 0.0003). The medians, interquartile ranges and P values are displayed as box and whisker plots in Figure 1.
Median frequency of blood test requests per patient per day by colorectal team a pre- and postintervention, and colorectal Team B control group. Error bars represent interquartile range.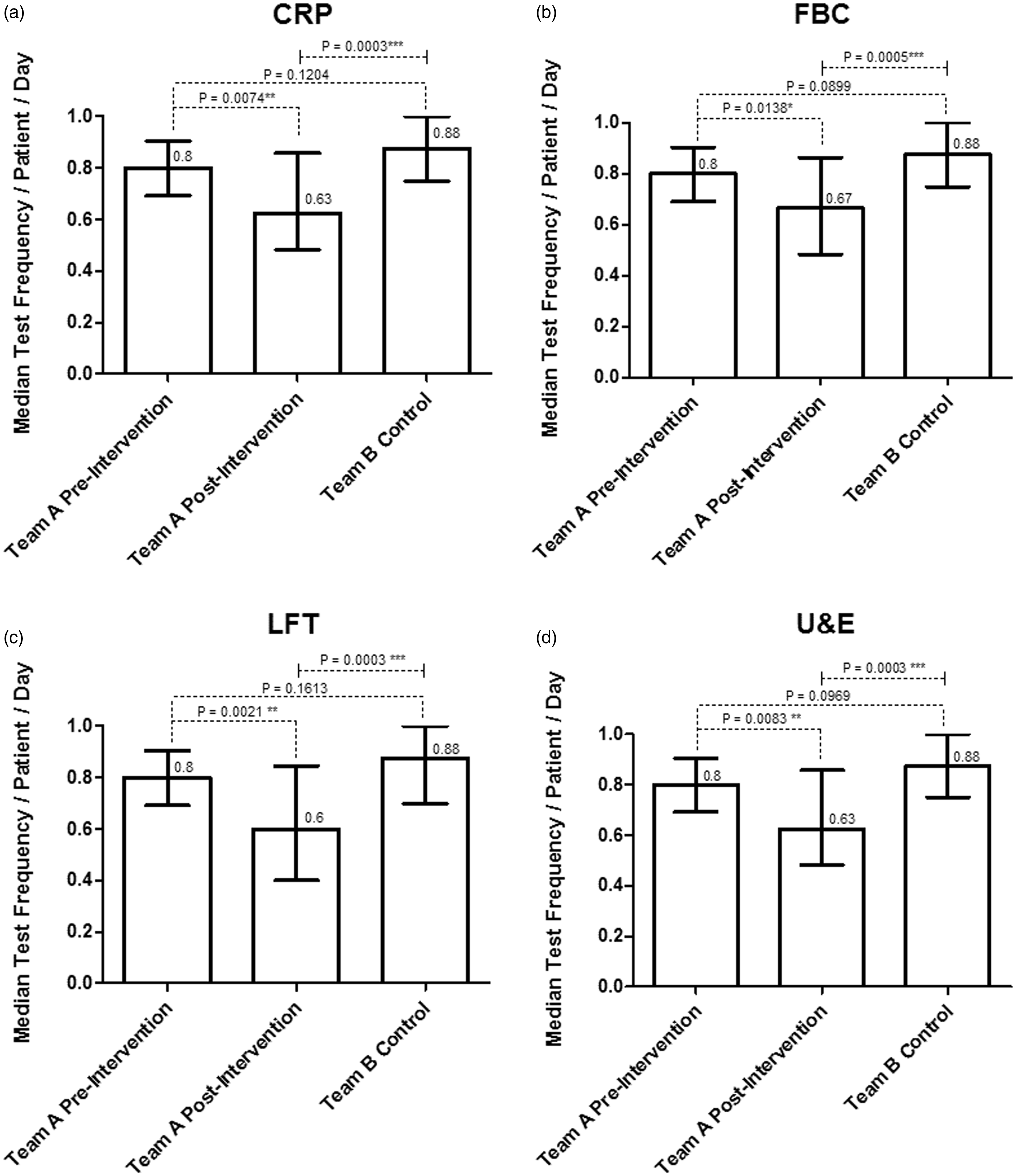
Cost-saving
Total number of blood tests requested pre- and postintervention.
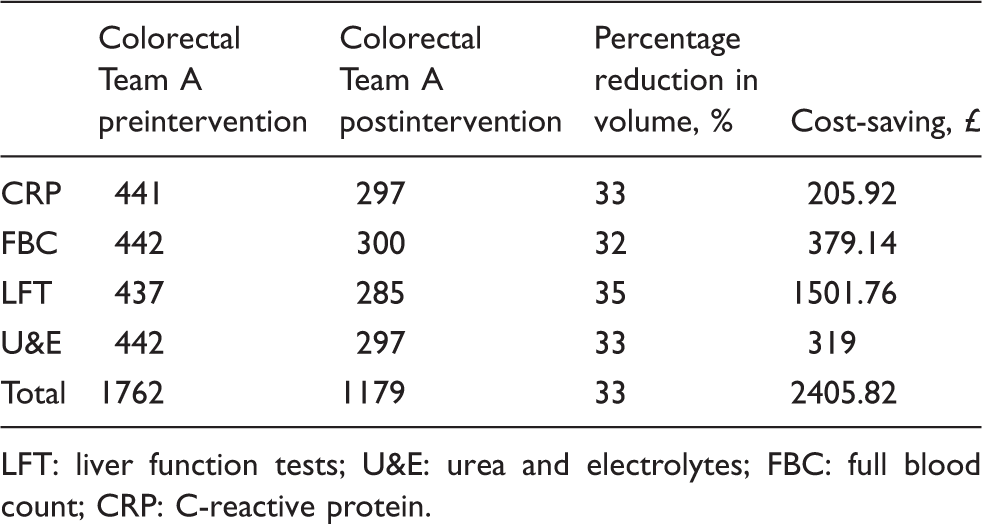
LFT: liver function tests; U&E: urea and electrolytes; FBC: full blood count; CRP: C-reactive protein.
Discussion
The reduction of unnecessary laboratory testing is an important area to consider in the attempt to contain costs. In this study, the number of blood test requests decreased on average by 33% after implementing a vetting procedure, based on clinical findings and under the direction of a senior clinician. No significant difference in length of hospital stay or admission to ASCU/CCU was seen in the group that had fewer blood tests. The number of blood tests requested per patient per day by Team A following the intervention were lower than the number requested before (P < 0.05); they were also smaller than the number requested by the control group Team B (P < 0.001).
Verbal feedback from junior doctors in both colorectal Team A and Team B indicated that uncertainty over the need for a particular test was the foremost reason why they ended up requesting unnecessary blood tests. This is among a wide range of other possible reasons such as lack of clinical experience, belief that the test may provide psychological reassurance to the patient, lack of awareness of the cost implications, patient and peer pressure, as well as lack of clear guidelines.5,8 The vetting undertaken by the senior clinician may have offset some of these factors by providing junior doctors with some guidance and insight into the rationale behind requesting particular blood tests during the ward round. Senior house officers (SHOs) and registrars report that ward rounds assist them in learning about clinical science and management of patients. 9 A survey by Gibson and Campbell 10 of SHOs identified ward rounds as an important learning opportunity. The respondents valued working in a team and gaining support from consultants, which helped them to deliver patient care and improve their knowledge. 10
Impact of the study
The impact of reducing unnecessary blood tests by 33% was financial with a laboratory cost-saving of £2406. Other potential benefits of requesting fewer blood tests include a reduction in the number of phlebotomy episodes, less discomfort and anxiety experienced by the patient, and a lower risk of false-positive results, which may subject patients to referrals, further investigation and follow-up. 5 The healthcare cost associated with laboratory testing itself is a fraction of all these downstream activities. 11 There are a lack of studies that evaluate the impact of reducing blood test requesting on patient outcomes outside of the laboratory. 5
The group of patients that received fewer blood tests in our study did not experience adverse effects in terms of length of hospital stay (P = 0.808) or admission to ASCU or CCU (P = 0.58). Wang et al., 12 reduced the number of blood tests over three months in a coronary care unit and demonstrated no adverse effects on clinical outcomes including length of stay, hospital mortality, readmission to the intensive care unit, readmission to the hospital or days of ventilator support.
Smith et al. 13 experienced an increase in biochemistry tests requested by junior doctors at Glasgow Royal Infirmary, in the UK. They introduced a vetting system in which a consultant clinician had to contact the clinical biochemistry consultant to request all out-of-hour tests. They reported a reduction of requests by 40% and concluded that senior clinical staff should take greater responsibility for use of laboratory services. A Canadian laboratory implemented a vetting system for specialist tests that needed to be referred to outside laboratories. 14 The requester had to email or fax an explanation of the clinical indication for the test, which was vetted by a clinical pathologist. This method led to a 50% reduction in test requests. Interestingly, 99% of the cancellations were by the requester. Their results suggest that an intervention targeted at the requester, which requires the requester to rationalize the clinical test, is a powerful means of laboratory stewardship. We feel it is important that demand optimization of laboratory resources should include shared responsibility with the requester, and there should be senior clinician involvement, as demonstrated in our study.
Limitations
The study was confined to the evaluation of only blood tests: CRP, FBC, LFT and U&E. Other blood tests were not evaluated. This was primarily due to the retrospective method of data collection. Data were collected from a database on the patient ward handover list, which contained fields for only the aforementioned blood tests. While the database limited data collection to a small number of high-volume tests, it had the advantage of allowing a standardized method for data collection. Other lower volume but more expensive tests may have been worthy of focus of our vetting intervention as even a modest reduction could yield considerable cost-saving. Another limitation of the retrospective data collection is that not all emergency admissions were included in our study. Patients admitted under the on-call surgical team were first recorded on a separate inpatient ward list for emergency patients only. The emergency ward list was not used for data collection because the rapid turnover of some of the patients made it difficult to identify them reliably in a retrospective analysis. It was normal practice for details of emergency admissions to be transferred to the consultants’ inpatient ward list if they were not discharged by the end of the consultants’ on-call, which lasted three or four days. Therefore, some patients that were discharged while under the care of the on-call team were not included in our study.
Our cost analysis took into account only the marginal cost of laboratory reagents, and this represents the actual saving of avoiding a test. The laboratory staff, analyser costs and overheads are not removed by a relatively small reduction in test numbers. In order to achieve a substantial saving, there would need to be a very significant cut in workload accompanied by downsizing of the laboratory, use of smaller, cheaper analysers and fewer staff. The effects of a significant reduction in tests also have potential impact on costs related to other areas of the hospital, such as a reduction in the numbers of staff operating the phlebotomy service, and reduction in the number of porters required to transport blood specimens from the wards to the laboratory. An alternative approach to using vetting, by senior clinicians, of the sort described in this study, in order to realize savings, is to implement large-scale improvements in efficiency within laboratory services. Our hospital is currently attempting to do this by consolidating pathology services into a network of laboratories across a wider geographical area. 15 The aim is to enable laboratories in the East of England to operate on a hub and spoke model whereby non-urgent tests from general practice are consolidated at the hub laboratories, and each spoke hospital has a smaller satellite laboratory, which has an on-site pathology service focused on fast turnaround of critical tests for its own inpatients. 15 This initiative is underway and the outcomes in terms of cost-saving is not known at present.
The authors acknowledge that the costs of laboratory tests are subject to geographical variation and that any cost-saving will be dependent on local laboratory costs. Therefore, the financial saving demonstrated in this study could be significantly over-estimated and may not be replicable at other hospitals. The extrapolated cost-saving for our general surgery department of £125,103 is based on a number of assumptions: (1) all 13 clinical teams having a similar baseline test request frequency; (2) each are capable of achieving at least the same reduction in test requests as Team A; (3) each are able to sustain this practice throughout the year; (4) all admit a similar case load as Team A. These assumptions significantly over-estimate the projected department annual cost-saving.
The vetting protocol has a resource implication. It requires a consultant or registrar to spend time on discussing their decision to request blood tests with junior doctors. This process when carried out for each patient can have a cumulative effect in lengthening the ward round, and there is a risk that senior clinician time is taken away from other duties. A critical factor in determining the benefits of the vetting intervention is the need to ensure a long-term sustained effect in order to prevent return to original requesting patterns. This limitation was minimized in our study as the intervention was targeted at core members of the clinical team at consultant level who were able to safeguard the vetting process irrespective of regular reconfiguration of the clinical team due to changeover of junior doctors. The vetting process has been successfully integrated into routine practice for Team A.
Further work will include (1) re-audit, to assess the sustainability of the senior clinician led-vetting process; (2) department-wide rollout of this intervention; (3) further research on the wider implications of this intervention on patient and clinical outcomes, and its impact on the phlebotomy, laboratory and clinical services.
In conclusion, the process of vetting of test requesting carried out by and directed by senior clinicians’ was a relatively simple and efficient change in clinical practice to establish and which reduced the number of unnecessary blood tests by 33%. In our laboratory, this translated to a cost-saving of £2406 over three months. However, the saving made by other laboratories and clinical teams adopting this approach may vary depending on local laboratory costs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work was deemed an improvement study and not a study on human subjects, and local policy indicated that ethical approval was not required.
Guarantor
AN.
Contributorship
VG and NRJ conceived the study and supported the implementation of the vetting intervention. AN conceived the study, developed the vetting protocol, and was involved in study design. ZM researched the literature, performed data collection, statistical analysis, and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.