
Abstract
Background
Healthcare budgets face constraints, and laboratories have developed strategies to adapt to the concomitant increase in workload. Some of the tests (7.4%) may be attributed to unnecessary repeat testing. Electronic gatekeeping has been implemented at selected laboratories in South Africa to limit unnecessary repeat testing. We performed a study of chemistry tests subjected to electronic gatekeeping to determine its effectiveness as a sustainable demand management tool.
Methods
A 22-month retrospective study of chemistry test requests at a Pretoria hospital was performed. Tests violating electronic gatekeeping rules were rejected upon registration before analysis, and cost-savings were estimated from electronic gatekeeping-held tests. The impact of electronic gatekeeping on the test requesting pattern of clinicians was derived from the percentage cost of electronic gatekeeping-held tests.
Results
The total savings generated from electronic gatekeeping test rejections amounted to $84,380. Greatest savings were generated from high-cost tests: glycated haemoglobin ($14,139), urea ($8661) and thyroid-stimulating hormone ($7514). The average number of electronic gatekeeping-held tests as a percentage of their total requested number over 22 months was 3.18%.
Discussion
The savings from electronic gatekeeping-held tests were not as dramatic as anticipated, but were modest and may have some impact in a cost-constrained setting. Electronic gatekeeping was concluded not to have a substantial effect on the clinician test requesting pattern, demonstrated by the largely unchanged monthly percentage of electronic gatekeeping-held tests. As a solitary demand management strategy, electronic gatekeeping does not appear to be as effective as anticipated or as demonstrated in other studies.
Introduction
With the increasing pressure on healthcare budgets, clinical laboratories worldwide are faced with the challenge to reduce the cost of their services despite limited resources and a marked increase in workload. 1 In South Africa, the National Health Laboratory Service (NHLS), a public health enterprise that serves approximately 80% of the population, demonstrated an increase in total pathology test volume for 2013/2014 of 3%. The capital province, Gauteng, denoted an annual increase in test volume of 7% for 2013/2014 and 2014/2015.2,3 The increase in utilization of laboratory tests can be attributed to various factors. Laboratory contributors include improved access to testing, the introduction of auto-analysers and the development of new tests. Information technology, electronic requesting and reporting and rapid data transfer over the last decade have also contributed to the increased demand for laboratory testing.4–6 The increase in workload has not, however, been matched by an increase in funding to clinical laboratories. This has necessitated the utilization of innovative cost control strategies to maintain the profitability of laboratories. Demand management, a macroeconomic principle, has been adapted to health policies, to maximize the utility of limited health resources, with the focus on ensuring appropriate test requesting in the clinical laboratory setting. 7 Demand management measures employed by clinical laboratories have included vetting of expensive or uncommon tests, reflex and reflective testing, implementation of clinical protocols, request form design and computerized laboratory management systems. 8 Inappropriate repeat testing contributes to a laboratory’s total workload. The rate of inappropriate repeat laboratory testing was estimated to be 7.4% (95% CI: 2.5–12.3%; n = 55) in a 15-year (October 1997–January 2012) meta-analysis. 9 Physician uncertainty of minimum retesting intervals, habit, delay in result availability or poor access to results may contribute to inappropriate repeat requesting of laboratory tests, most significantly for hospital inpatients. 10 Inappropriate repeat testing can be curtailed by considering the minimum re-testing interval, based on the properties of individual tests and the clinical context for their use. 11 The NHLS has employed a system of electronic gatekeeping (EGK), utilizing minimum re-testing intervals, among other considerations, as a demand management strategy to limit inappropriate repeat testing. Often, cost implications are not central to the clinician’s consideration for laboratory test requesting. With this tool, cost-saving and efficient test requesting can be facilitated in a responsible way. 12 Since its implementation at selected NHLS laboratories in South Africa, an audit of chemical pathology test rejections by EGK has been performed at an academic hospital in Cape Town. 13 Findings revealed that 6.7% (4605 of 68,480) of chemistry tests were rejected due to EGK, according to site-specific criteria over a six-month period. No specific impact was reported on patient care in 80% of cases, and a total cost-saving of $36,759 was generated. 13 Whereas this audit verified the value of EGK as a demand management tool to facilitate cost-savings without detriment to patient care, its impact on the requesting patterns of clinicians deeming their acceptance of the intervention over an extended period, remains to be determined. Clinician response to a computerized system for managing potentially frequent laboratory testing was analysed by Janssens and Wasser. 12 They noted an initial increase in test rejections for two years following the implementation of their strategy. Quantitative information on the impact of various demand management strategies remains limited. In this paper, we determine the utility of EGK as a sustainable and profitable demand management tool. We performed an audit of the chemistry tests subjected to EGK to observe the impact on clinician test requesting patterns, since its implementation at an academic hospital in Pretoria, serviced by the NHLS. The savings from chemistry tests that have been subjected to EGK over 22 months will assist in determining the profitability and sustainability of EGK as an individual demand management strategy.
Method
Study design
This was a retrospective observational study of all the chemistry tests requested at the Pretoria NHLS academic laboratory over a period of 22 months (from January 2013, two months after the implementation of EGK). The period from December 2013 to April 2014 was excluded from the analysis. An EGK data processing error was identified at the institution that resulted in a gross under-estimation of EGK-held tests for that period. This laboratory services the Tshwane district and includes Steve Biko Academic Hospital (SBAH), an 866-bed tertiary institute in Pretoria. Only data pertaining to SBAH were included in the analysis.
Gatekeeping procedure
EGK rules applied to selected analytes indicating time limits between repeat requests and conditions for over-ruling time limits.
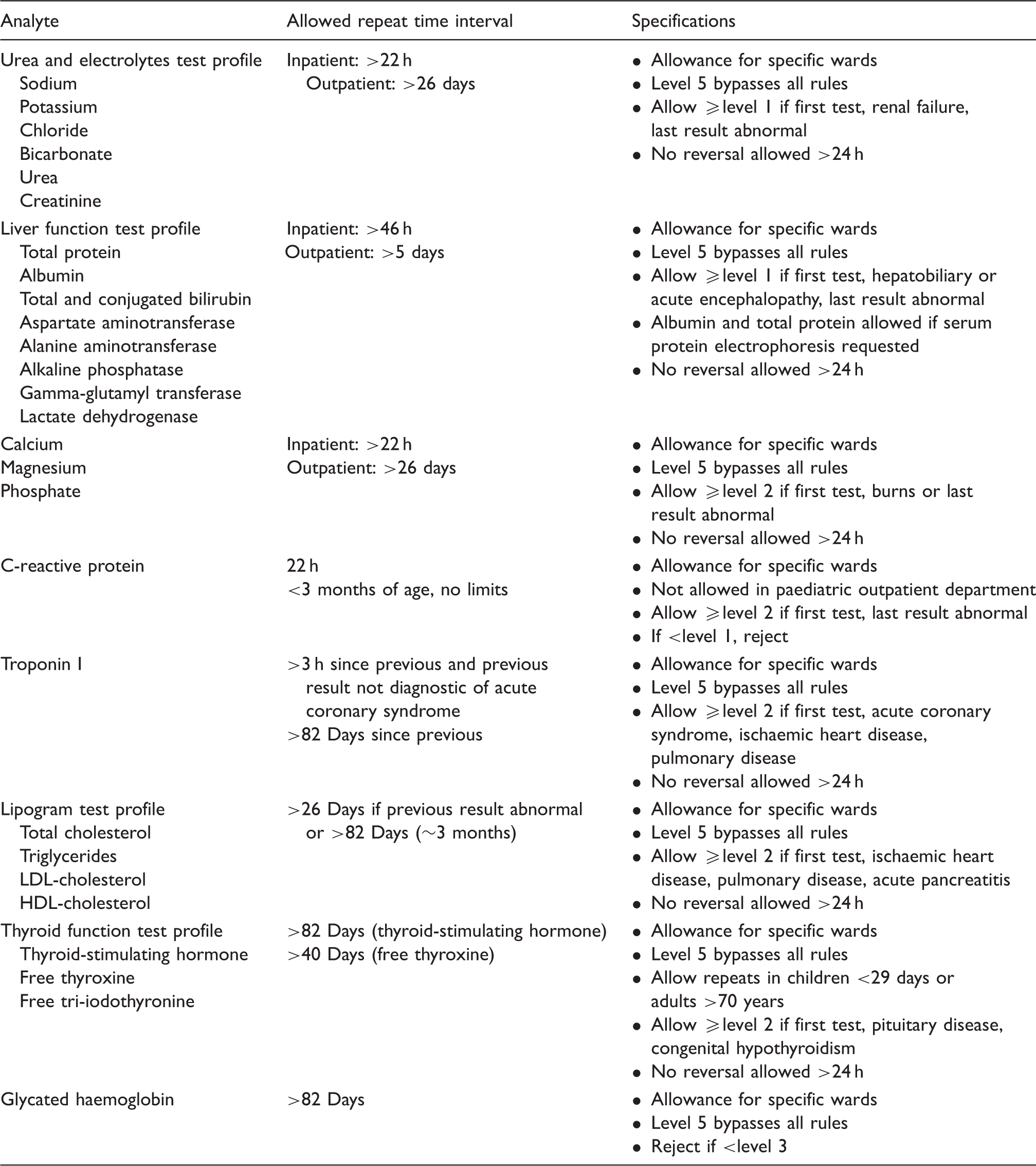
Note: Rules operate by defining conditions for outright rejection, as well as multiple conditions for when a test is allowed. Requesting clinician seniority is determined according to registered qualification and is programmed into the LIS.
Level 0 – no assigned seniority level.
Level 1 – Intern.
Level 2 – Medical officer.
Level 3 – Registrar (resident/specialist trainee).
Level 4 – Registrar and medical officer with consultant status, named chief medical officer.
Level 5 – Consultant/specialist.
The laboratory is not fully automated, and test requests are manually entered into the LIS upon receipt of the request form and sample(s). Tests are thus only subjected to EGK upon receipt and registration of the clinicians’ requests. The following automated rejection comment reflects on the report for the tests which were registered and subsequently subjected to EGK: Test automatically rejected on the basis of the hospital's electronic gatekeeping rules. If it is clinically necessary for the test to be performed, the rejection can only be reversed by providing a valid approval number to the laboratory. This must be done before the stability limits of the test are exceeded. Schematic outline of the gatekeeping procedure.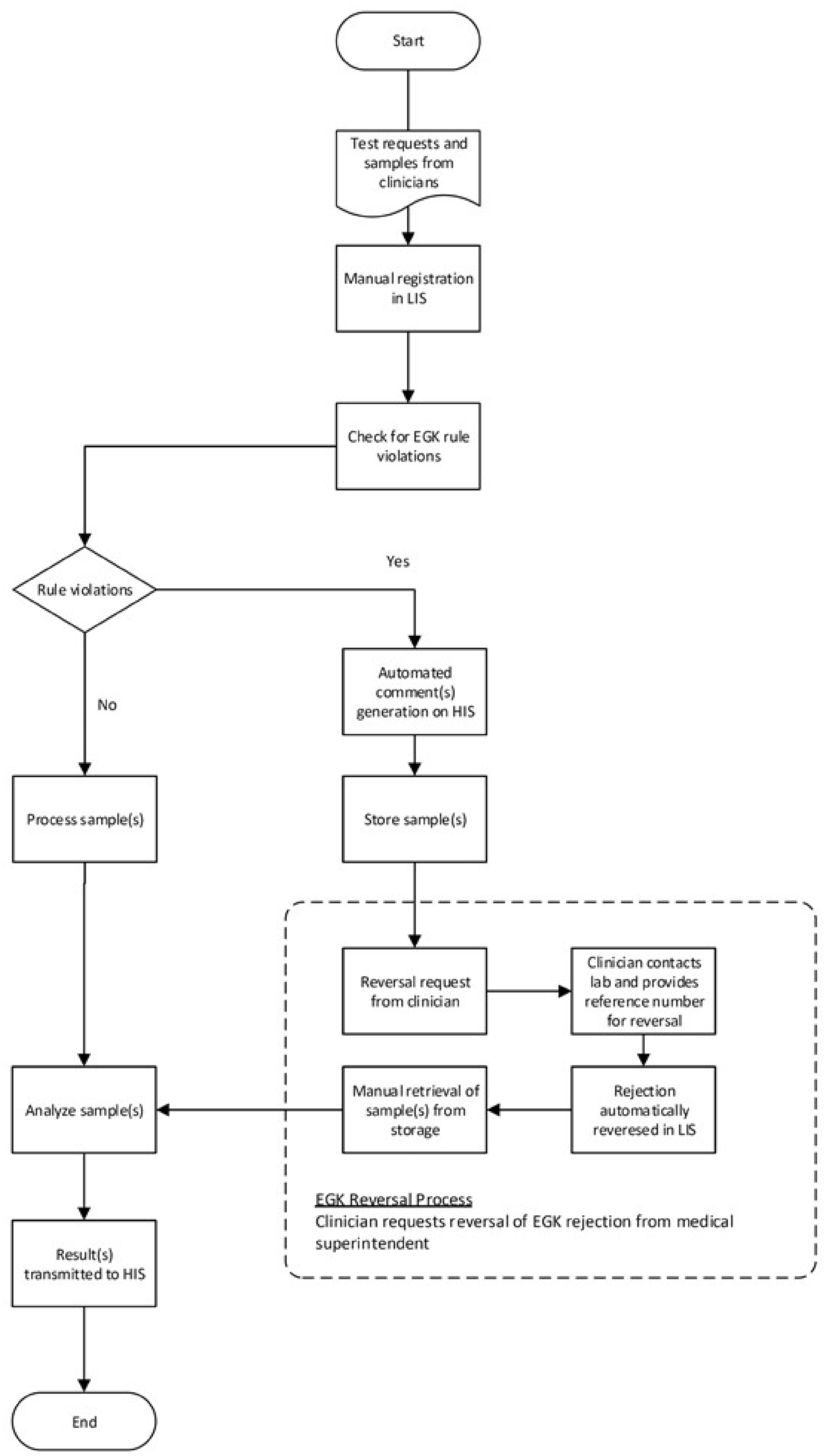
Data analysis
Data were obtained from the NHLS corporate data warehouse and included all chemistry tests requested and billed over the 22-month period as well as chemistry tests that were subjected to EGK (Table 1) and thus not billed. Cost-savings were computed from the number of tests subjected to EGK and the billed value of these tests. The impact of EGK on the requesting patterns of clinicians was determined by the number and tendency of EGK-held tests computed each month for the period of assessment.

The percentage of EGK-held tests was determined to account for changing patterns in requesting volumes over the period of assessment. This analysis was also computed for the urea and electrolytes test profile ([U&E] includes sodium, potassium, chloride, bicarbonate, urea and creatinine) and the liver function test profile ([LFT] includes total protein, albumin, total and conjugated bilirubin, aspartate and alanine aminotransferases, alkaline phosphatase, gamma-glutamyltransferase and lactate dehydrogenase), representing the most frequently requested tests. The thyroid function test profile ([TFT] includes thyroid-stimulating hormone, free thyroxine and tri-iodothyronine) was also included, as a representation of tests requested in the predominantly non-acute setting. Data were analysed using Microsoft Excel®. All monetary values were computed from Rands (R) to Dollars ($) using a conversion rate of R15.57 to 1$ as per the South African Reserve Bank exchange rate on 23 May 2016. 14 Tests were performed on the Beckman Coulter Unicel Dxc 600/800 and Dxi 600/800 platforms.
Ethical consideration
The study was approved by the University of Pretoria Ethics Committee.
Results
Cost-savings
Count of billed tests and test profiles, their EGK-held counts, the cost-saving according to the billed value of the tests, savings lost from EGK reversals and the effective savings from EGK-held tests.
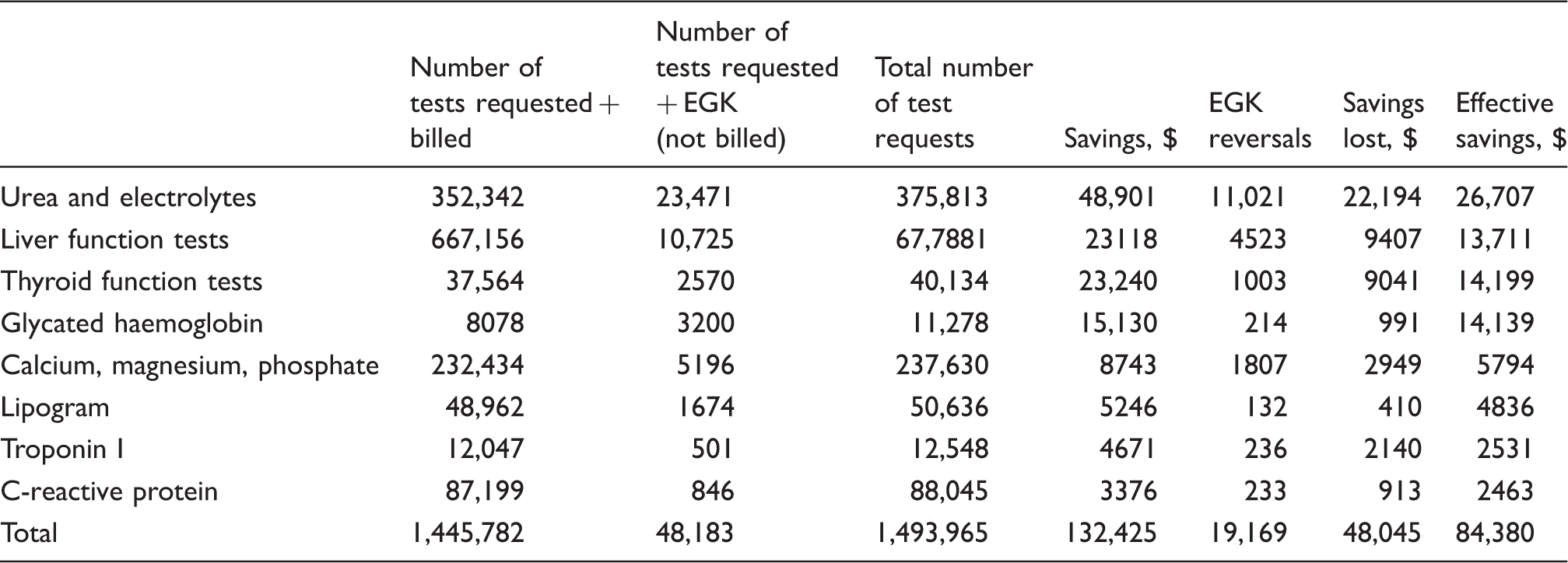
Savings were computed according to the billed value of the EGK-held tests. A total of 19,169 EGK reversals resulted in a loss of savings of $48,045. Effective savings of $84,380 were thus achieved. Tests most frequently subjected to EGK included the U&E profile and glycated haemoglobin (Figure 2); however, the greatest savings were generated by glycated haemoglobin ($14,139), urea ($8661) and thyroid-stimulating hormone ($7514), owing to their higher billed values (Figure 3(a)).
Count of EGK-held tests and reversals. (a) Cost-saving from EGK-held tests with reflected reversals; (b) quarterly cost-savings from highest saving EGK-held tests. (December 2013 excluded from Quarter 3).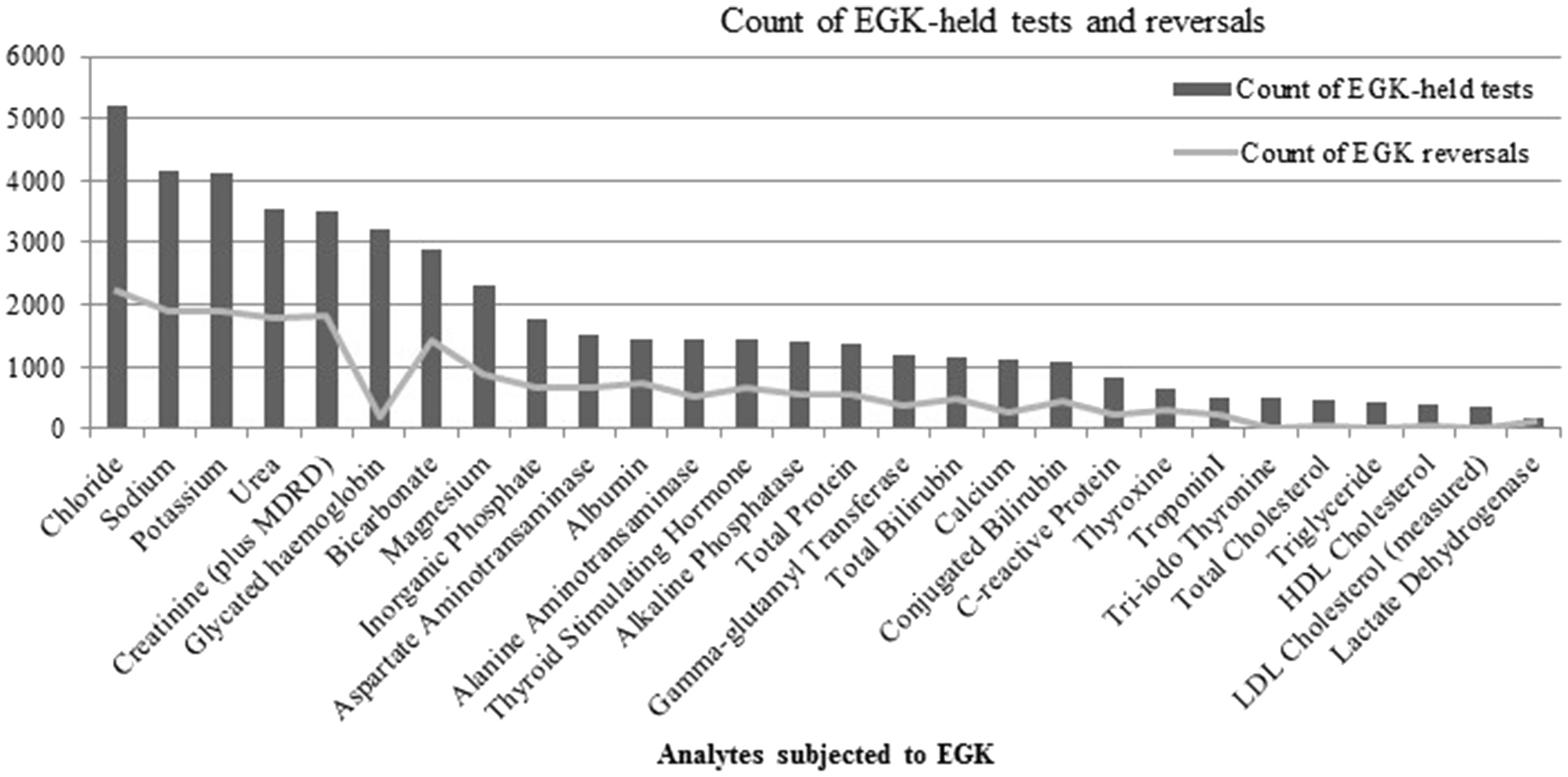
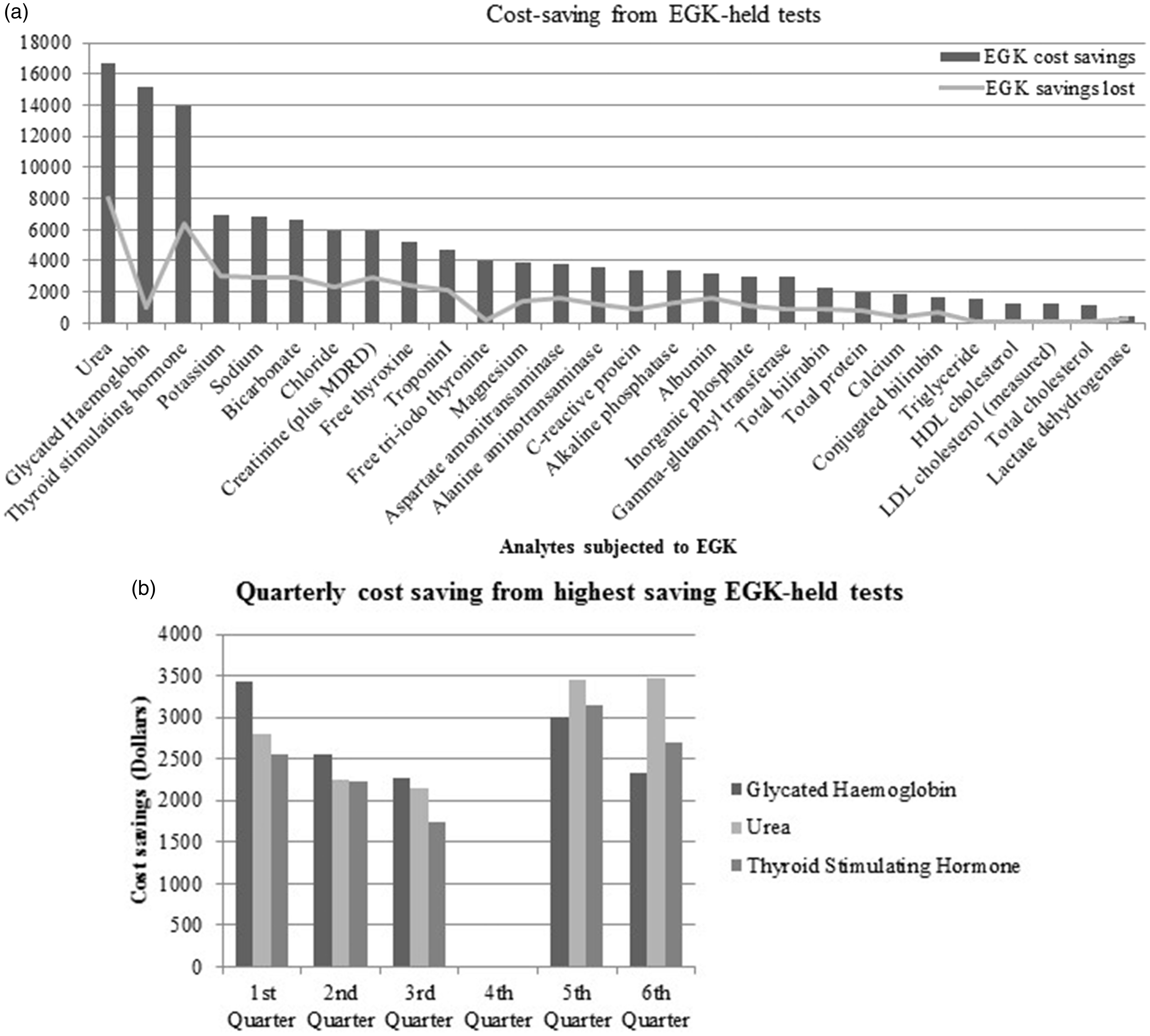
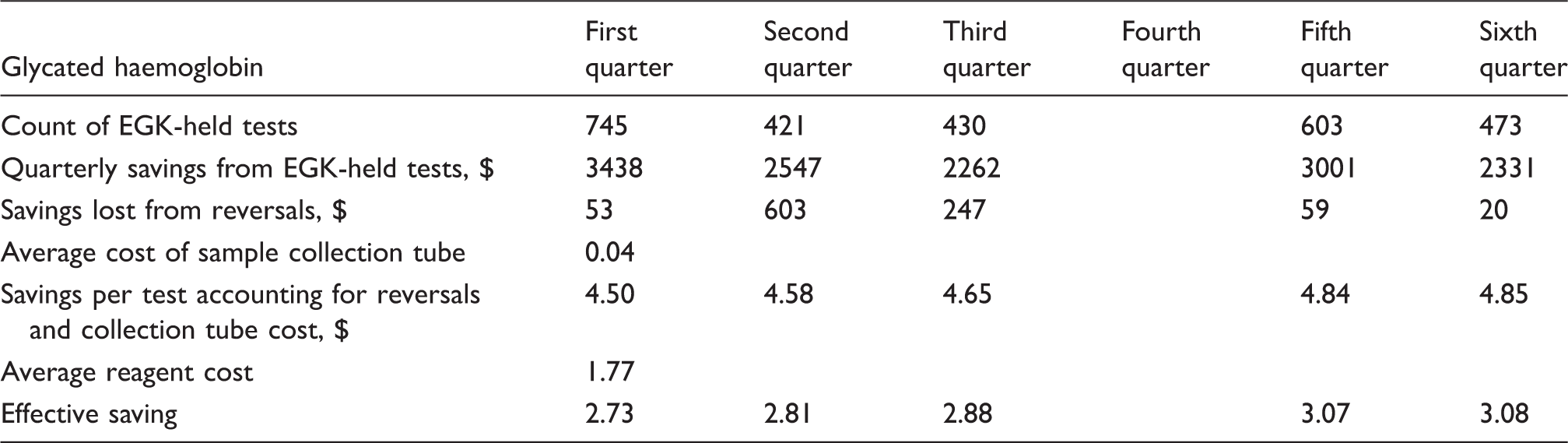
Quarterly savings per test generated by glycated haemoglobin accounting for estimated lost savings and reagent cost saved (December 2013 excluded from Quarter 3).
Requesting patterns
The monthly count of EGK test rejections and the percentage of EGK-held tests (to their total requested number) over the 22-month period are represented in Figure 4(a).The average percentage of EGK-held tests was 3.18%. Figure 4(b) further demonstrates the percentage of EGK-held tests to their total requested numbers alongside the pattern mirrored by the U&E, the LFT and the TFT test profiles.
(a) Trend of the number of EGK-held tests and their percentage of total requested tests from January 2013 to March 2015. (data exclude the period from December 2013 to April 2014). (b) EGK-held tests represented as a percentage of their total requested numbers: total, U&E test profile, LFT test profile and TFT test profile (data exclude the period from December 2013 to April 2014);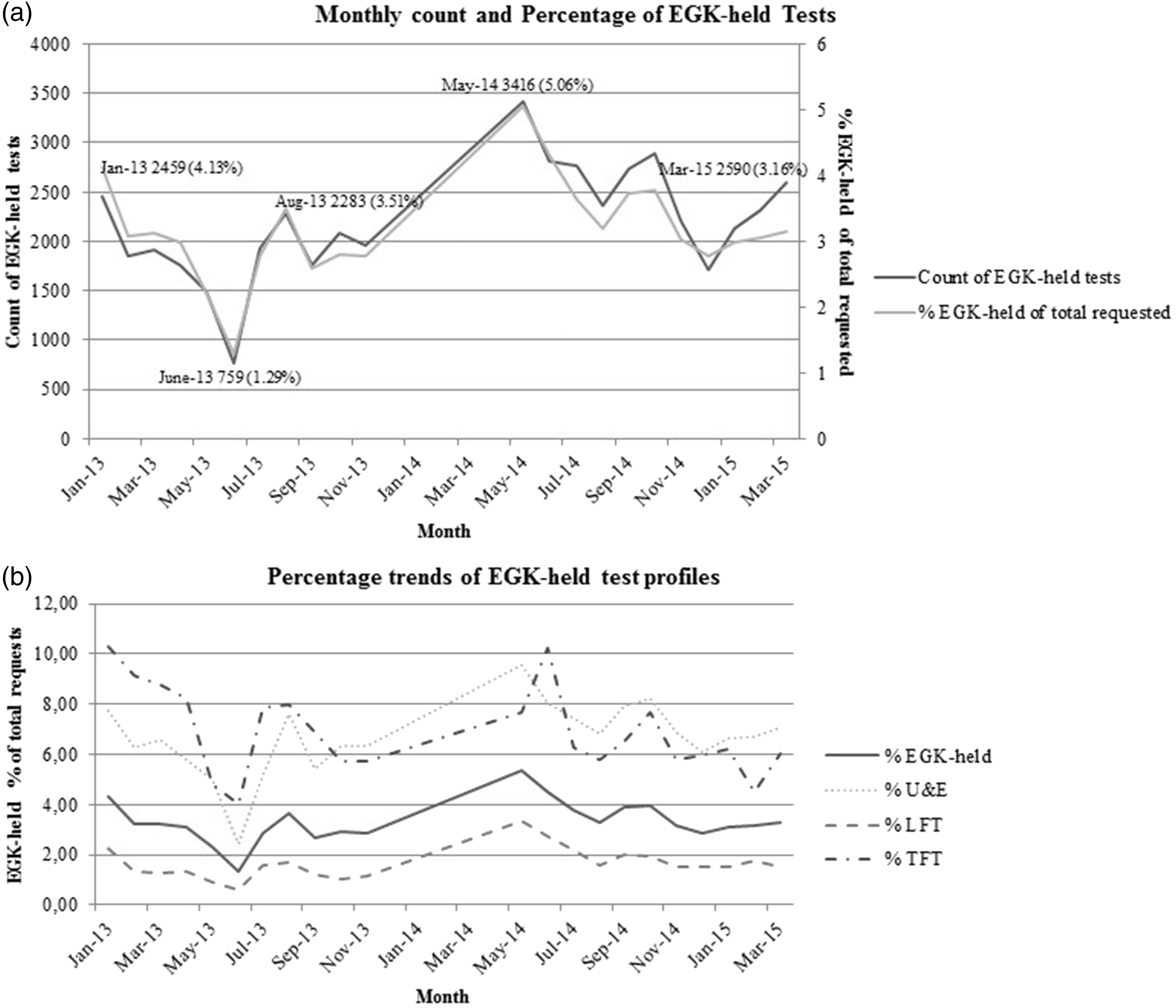
Discussion
With this study, we determined the cost-savings from and the impact of, EGK chemistry test rejections since the implementation of EGK as a demand management tool at a tertiary hospital in Pretoria, South Africa. Savings amounted to $84,380 over 22 months. The percentage pattern of EGK test rejections to their total requested counts was used to infer the impact of EGK on clinicians’ test requesting behaviour since the implementation of EGK. No notable impact was demonstrated.
Of the 1,445,782 tests subjected to EGK, 48,183 (3.33%) were rejected, lower than the region’s percentage increase in total pathology workload for this period. The albeit modest workload decrease accommodates the critical national shortage of medical technologists. High-cost tests generated more savings in comparison to high-volume tests. Total savings were moderate (1.78% of corresponding billed tests). Analysis of the quarterly savings generated by glycated haemoglobin (highest saving test) demonstrated unsatisfactory findings (Table 3). When EGK reversals (lost savings), collection tube costs (lost savings) and cost saved from reagent not utilized are accounted for, the ‘profit’ generated per quarter, per test ($2.73, $2.81, $2.88, $3.07 and $3.08, respectively) are not as remarkable as anticipated. Considering costs not accounted for (labour, transport, processing, steps in EGK reversals), this saving per test may be inconsequential. The laboratory in which the study was undertaken is multidisciplinary and houses chemistry, haematology, microbiology, virology, immunology, serology and anatomical pathology departments. Transport, labour and consumable costs pertaining to individual departments cannot be separated.
Our results showed similar average monthly savings ($3835) in comparison to an academic hospital in Cape Town also serviced by the NHLS ($5245); however, the rejection rate between the two institutions varied 10-fold (3.18% over 22 months, Pretoria compared with 6.7% over six months, Cape Town). This may be explained by the higher request volumes of chemistry tests subjected to EGK (65,717 per month for Pretoria, 11,413 per month for Cape Town) or may be indicative of the effect of site-specific rejection criteria. 13 Alternatively, it may demonstrate the adjustments that are likely to occur over a protracted period. Our rejection rate is more in keeping with that reported by Janssens and Wasser of 0.56% in their study where 44 tests were subjected to minimum retesting interval rules, in comparison to our 31 tests. Tests included routine chemistry requests as well as specialized DNA and autoimmune profiles. 12 With our current EGK rules, there is room for greater savings as our programme still permits a degree of unnecessary repeat testing. Longer retest interval limits would facilitate higher cost-savings; however, a more conservative approach was employed to implement the system and facilitate the requirements of the requesting clinicians.
The monthly percentage of EGK-held tests to their total requested volumes remained largely unchanged. A decline in EGK-held tests would ideally be expected in a setting where the tool has assisted clinicians to adjust their test requesting behaviour to align with the implemented EGK criteria. Despite the implementation of EGK, total chemistry test requests exceeded the annual provincial increase in pathology test volume (7%) for 2013/2014 (7.7%) and 2014/2015 (9.6%).2,3 In this regard, EGK did not have a substantial effect on the clinician test requesting pattern in our setting, as assessed by the monthly percentage of EGK-held tests to their total requested volumes.
The requesting pattern remained unchanged for the U&E, LFT and TFT test profiles (Figure 4(b)). Owing to their lower request volumes in comparison to LFT, U&E and TFT test profiles demonstrated a higher percentage of EGK-held tests as compared with the total test repertoire subject to EGK. TFTs were considered to represent tests that are requested in the predominantly non-acute setting. These percentages show that requesting patterns have remained unchanged over an extended period, independent of the clinical setting, since the implementation of EGK as a demand management tool at the institution. In order to remain an effective and sustainable cost-saving tool, it would therefore need to be permanently instituted. A risk of long-term implementation, however, is a decline in efficacy, as users develop strategies to overcome the criteria for rejection as they gain insight and experience in its use. In the study by Janssens and Wasser, following an intervention aimed to reduce unnecessary repeat testing, they observed an initial increase in rejection frequency for as long as two years following the intervention. However, this ultimately decreased to levels lower than the initial proportion rejected. This observation was deemed as an acceptance of requesting clinicians of the implemented system; however, the steady decline in laboratory testing experienced was not solely attributed to their intervention, but considered to be due to multiple measures that improved the clinicians’ awareness of laboratory costs and their impact. 12 Krasowski et al. 15 evaluated the impact of different interventions to promote effective utilization of laboratory testing in a case study over five years. Greatest savings were generated by strategies applied to tests referred to other laboratories (23% decline, annual direct institutional savings $600,000). Cancellation of high frequency, duplicate test requests demonstrated a comparably moderate decline of 8% with estimated annual savings of less than $400,000. 15 EGK holds the potential to facilitate greater savings with interventions applied to lower frequency, higher cost, specialized tests. 16 Determining the root cause of wasted care can facilitate focused interventions to improve laboratory test utility. Sadowski et al. 17 identified automated test ordering as a driving factor for misuse of laboratory testing. Their intervention aimed to reduce automated testing generated improved outcomes compared with a generalized demand management intervention.
In the current study, the essentially unchanged requesting pattern, 29 months following the implementation of EGK, may be interpreted as an unsuccessful attempt at demand management. In its absence, test requesting behaviour would presumably be unchanged. Although this pattern may be attributable to clinicians not accepting the demand management strategy, it may also reflect the high turnover of requesting clinicians through different departments as part of their training. At this tertiary institution, tests are predominantly requested by trainee interns and registrars. Their level of experience and stage of training would affect their utilization of laboratory tests. 18 This emphasizes the drawback of not having a bi-directional communication network between the ordering system and the laboratory database. 12 The delay in feedback of tests requested and subjected to EGK, which may vary from hours to weeks, depending on when the reports are viewed, leads to greater frustration with the laboratory services and reduces the chance of the requestor having learnt about appropriate test requesting. 12 In a tertiary centre employing computerized physician test ordering, Bates et al. found that physicians would change their test requesting behaviour when given suggestions based on patient-specific information, such as the display of the date and previous test result and computerized prediction of an abnormal test result. 19
Recognized limitations of this study include an overestimation of cost-savings. The total cost of consumables utilized for drawing blood samples, transport to the laboratory and labour costs for EGK-held tests could not be separated from costs to other pathology departments serviced by the audit laboratory. Additional labour costs associated with reversal of EGK-held tests (including sample retrieval and additional labour) were not accounted for. EGK development, implementation and maintenance costs were not factored into the effective cost-savings.
Requesting patterns were inferred from laboratory test request numbers, and no direct clinician input was sought. Within the framework of this study, we did not consider the reasons for EGK test rejections nor their clinical impact.
Conclusion
We concluded that the savings generated by EGK were unexpectedly moderate. As the strategy was easy to implement, monitor and sustain, this may have some impact in a cost-constrained setting. The monthly percentage of EGK-held tests and test profiles was largely unchanged during the period of assessment; therefore, EGK was concluded not to have a substantial effect on the clinician test requesting pattern. When used in conjunction with other demand management tools previously reported, EGK may have the potential to result in a collectively larger reduction of unnecessary repeat laboratory test requests and serve to improve the utility of laboratory tests in a cost-constrained setting. However, as a sole demand management tool in the study setting, EGK was not evidenced to be as effective a strategy as demonstrated in other studies.
Footnotes
Acknowledgements
The authors thank Mr M Tepper (Corporate Data Warehouse, NHLS) for his assistance with data mining, Mr RC Chibba (Senior business strategy advisor, Eskom, BComm, MBA) for his contribution to data streamlining and analysis, Professor PJ Becker (Biostatistician, University of Pretoria) for statistical consultation and Dr SP Dlamini (Chemical Pathologist) for his guidance with data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of the University of Pretoria approved this study (REC number 392/2015).
Guarantor
TSP.
Contributorship
AKP and OK conceived the idea for the study. TSP designed the data collection process. AKP gathered and analysed the data for the study, researched the literature and produced the first draft of the manuscript. AK, OK and TSP designed the study. The ethics application was completed by AKP, OK and TSP. TSP researched the literature and revised the first draft of the manuscript into its final form. All authors have accepted responsibility for the entire content of this submitted manuscript and approved submission.