
Abstract
Background
Demand management is an area of laboratory activity, which is becoming increasingly important. Within the health-care system, demand management can be defined as the use of health resources to maximise its utility. Tygerberg Hospital has introduced an electronic gate-keeping system. Chemistry tests which generate the highest cost are subjected to this system and may be automatically rejected according to a set of rules. This study aimed: (1) to identify the number of chemistry tests rejected by the eGK; (2) to identify which of these rejected tests were subsequently restored and (3) to assess the impact of rejections on clinical outcome and cost-saving.
Methods
A retrospective audit was conducted to determine the number of chemistry tests rejected and subsequently restored over a 6-month period. The case-notes of patients for whom requested tests previously rejected had been restored were randomly selected and investigated to assess clinical impact. Any cost-saving was calculated.
Results
A total of 68,480 tests were subjected to gate-keeping, and 4605 tests (6.7%) were rejected while 679 (14.7%) of these were restored by the requestor phoning the laboratory after obtaining authorisation. After examining a subset of clinical notes it was found that in most cases (80%), patient care was unaffected. The total cost saved was £25,387.
Conclusions
The majority of the rejected tests were unnecessary and following rejection, real savings were made. Electronic gate-keeping is a simple, effective and sustainable method of demand management.
Introduction
Globally, health-care systems are under great pressure to reduce cost while continuously providing quality and efficient care. Laboratory services form an integral part of any health-care system and are experiencing similar pressure to ensure cost-effective diagnostic testing within a limited budget. It is estimated that 70–80% of all health-care decisions affecting diagnosis, treatment and follow-up involve pathology investigations. 1 Attention has previously focused on laboratory medicine as a potential source of savings, presumably because their costs are perceived as being easily identifiable and quantifiable. 2
Most clinical laboratories continue to see an increase in workload every year, usually without any matching increase in budget.1,3–5 Various reasons have been proposed to explain this increase in demand; these include: an increase in the number of geriatric patients; an increase in the numbers of patients with chronic diseases; better-informed patients; a wider availability of tests with quick turnaround times and increased use of test requesting by medical practitioners for medicolegal reasons such as protection from litigation.3–6 Increases are seen in both appropriate and inappropriate requests. Inappropriate laboratory requests include both over- and under-utilisation. Examples of tests that are most subject to over-utilisation include routine automated tests such as full blood counts and chemistry panels. 7 Various studies have reported that 8–30% of all requests could be considered inappropriate depending on the tests analysed and criteria used.1,4,8–11 In its broadest sense, an inappropriate request is one that should not be processed, because it is requested in the wrong patient, at the wrong time, in the wrong way, or is for the wrong test. 2
Demand management is now becoming an established concept in laboratory medicine. Initiatives to manage upstream demand and downstream interpretation of laboratory tests are crucial to defining the mission of clinical laboratories. 12 Within a health-care system, the term can be defined as manipulating the use of health resources to maximise their utility. 13 Demand management should be distinguished from demand control which refers to control of the volume of requests received by the laboratory. It should focus on ensuring appropriate requesting and therefore has an inbuilt quality aspect. 2 The ideal strategy for demand management should ensure that the right test is done on the right patient at the right time. 6 Strategies used to introduce demand management include: altering pathology request forms; clinician education; audit and feedback; introduction of clinical guidelines; instituting computer rules and reminders; introduction of rules and agreements aimed at restricting requests; process changes; changes in reimbursement policies; electronic decision-support systems and budget holding and financial controls.2–5,7 The approaches used are constrained by quality considerations related to the patient’s well-being and the required care, as both overuse and underuse of diagnostic testing affects patients. 14 Eliminating unnecessary testing may result in a number of benefits including decreasing cost, eliminating work-ups of falsely abnormal results and reducing hospital acquired anaemia. 7 Research on the effectiveness of many of these approaches remains limited. 14 Bates et al. 15 performed one of the first large studies on demand management in 1999, investigating the effect of computerised reminders on test requesting. There is however a paucity of research into the impact of demand management on patient care.
The simplest demand management strategy is probably to use minimum retest interval (MRI) data to prevent duplicate testing. These are adopted by many laboratories based on criteria such as analyte half-lives and analytical variability. 3 However, other factors including synthesis and breakdown, i.e. the homeostatic balance and any underlying pathology have to be considered when establishing any MRI. An MRI should be practical and should also take into acount the likely frequency of outpatient follow-up. 14 The Association for Clinical Biochemistry and Laboratory Medicine provided a set of evidence-based recommendations for appropriate MRIs based on the properties of the test and the clinical situation. 16 Filtering tests that are requested too frequently has been reported to decrease test turnover by 15% or more.4,17–20
In the laboratory at Tygerberg Hospital, an electronic gate-keeping system (eGK) was introduced as a pilot project to cut down on costs. The National Health Laboratory Service (NHLS), which administers and manages all laboratory services in the public sector in South Africa, recently appointed an eGK committee to expand the practice to other teaching hospitals and eventually all NHLS laboratories in South Africa. The purpose of the present study was to identify the number of tests rejected and restored (i.e. approved for analysis) by the eGK as well as cost saved, and to investigate the impact of any such rejections, on clinical outcomes.
Methods
Ethical consideration
The study was approved by the Stellenbosch University Ethics Committee. A waiver of consent was approved due to the nature of the study and the difficulties foreseen in tracing such a large group of individuals.
Study site
A retrospective audit was conducted at the NHLS Chemistry laboratory at Tygerberg Hospital (TBH). This laboratory provides a 24 h diagnostic service to TBH and smaller peripheral hospitals and clinics, and receives approximately 100,000 chemistry test requests each month. Tygerberg Hospital is situated in Cape Town, South Africa and provides inpatient and outpatient care to public health-sector users. It is a 1400 bed multidisciplinary teaching hospital affiliated with Stellenbosch University. The NHLS is the preferred provider of pathology services to the public health-sector and is therefore funded by the Department of Health.
Test ordering and gate-keeping
Electronic gate-keeping rules applied at TBH chemical pathology laboratory and tests subjected to eGK.
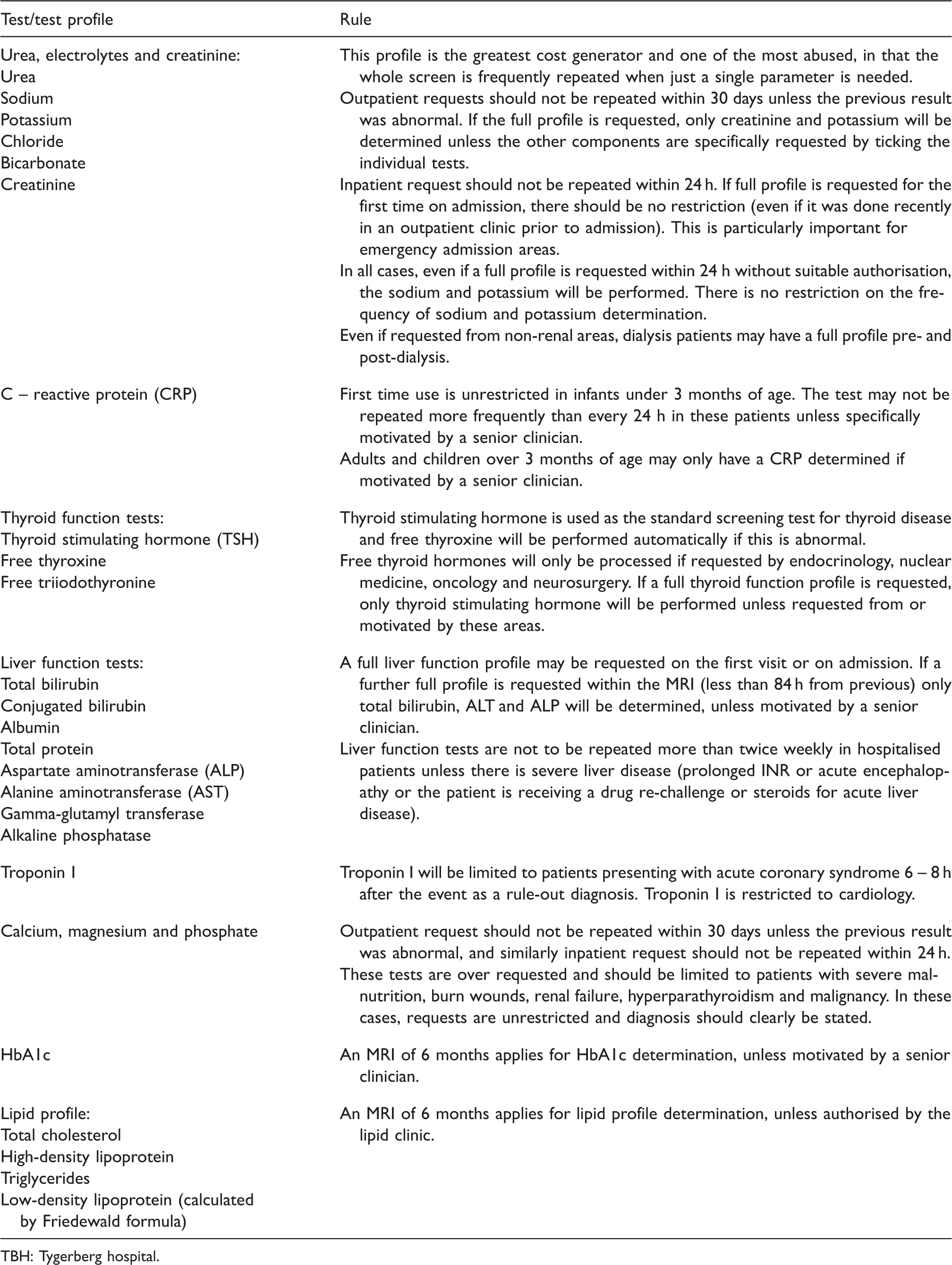
TBH: Tygerberg hospital.
Tests are requested using a laboratory request form, which is completed manually by the clinician. The clinician is thus unaware of rejection at the time of the request. Laboratory reception staff capture the data and enter the various tests requested onto DISAlab. Results are reported using DISAlab and can be accessed by the clinicians once authorised. If a test has been rejected due to a gate-keeping rule violation, then a message explaining the reason for the rejection is displayed on the report.
The clinicians may telephone the laboratory to restore the rejected test if it is clinically indicated. The laboratory technologist on duty will restore the rejected request after the clinician has obtained authorisation and will document this by entering an authorisation code onto DISAlab. Restored tests are performed immediately after this process is complete. Since the department does not have a fully automated laboratory system, the technologist will find the sample in the storage area and load it into the analyser for processing. Tests requested for both inpatients and outpatients treated at TBH are subjected to eGK.
Data analysis
The laboratory information system of the NHLS, DISAlab, was used to extract the laboratory data for the 6-month study period (1 July–31 December 2013). The number of requests subjected to eGK was obtained and a rejection rate was calculated. Restored tests were also extracted and the percentage of restored to rejected tests was calculated. Only tests that were rejected and subsequently restored were used in this calculation and we did not include tests that were repeated after the initial rejection. Cost-saving was calculated by using the average cost per test over the 6-month period. For this calculation, we used the official rate charged by the laboratory to perform the tests.
To assess the clinical impact of the rejections on patient care, a hundred restored tests were selected by simple random sampling and clinical notes were evaluated. Clinical impact was assessed and defined as:
delayed further laboratory investigation; result unavailable for imaging study; result unavailable for surgical procedure; delayed discharge (by at least 24 h); delayed/prolonged treatment; no specific impact (except delayed result).
Statistical analysis
Microsoft Excel® was used to analyse data.
Results
Total tests requested, rejected and restored
List of tests studied, rejected and restored by eGK with cost-savings in £Sterling.
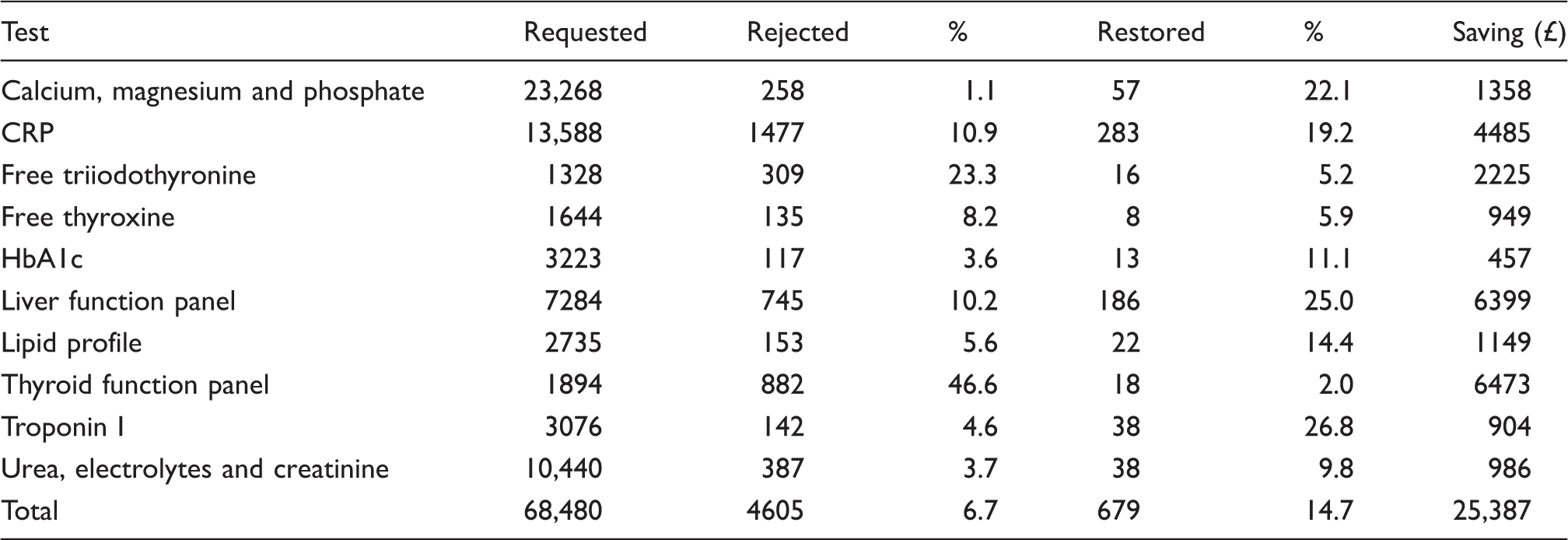
Cost-saving
The biggest cost-saving was seen on thyroid and liver function testing. An overall cost-saving of £25,387 was achieved by eGK. Table 2 gives a breakdown of all tests studied, rejected, restored and cost saved.
Clinical impact
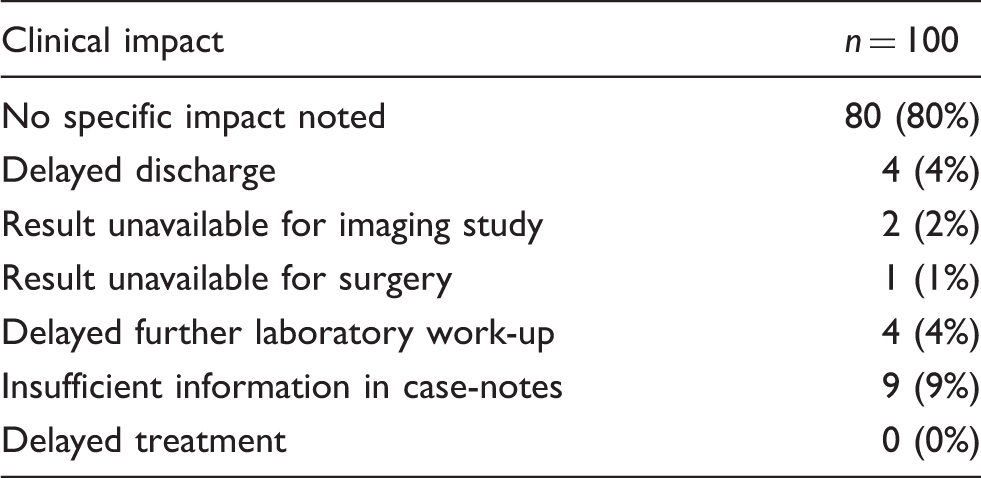
Assessment of clinical impact of rejections.
Discussion
In this paper, one of the first from Africa, we describe the effect of the rejection of tests, carried out by the eGK system, upon cost-savings and clinical impact, which were implemented by our laboratory as a means of demand management. Budget constraints and a rise in test requests led to the implementation of eGK rules in 2010 as a pilot programme with a view to national implementation sometime in the future.
We found eGK to be an effective and sustainable demand management tool. We found that most rejected tests were not restored, which questions whether these tests were in fact necessary or appropriate in the first place. The use of eGK did not appear to have a negative impact on patient care and was an effective cost-saving tool. This system will now be rolled out nationally in South Africa to save costs in the public health-care sector.
Our results showed a rejection rate of 6.7%, which is higher than that has been described in other studies. Janssens and Wasser 14 investigated a computerised system for managing overtly frequent laboratory testing and calculated cost-savings. However, these authors studied a different test profile than we did. Our study included more routine, frequently requested tests whereas those outlined in the report by Janssens et al. were less routine in nature. These authors also used a less stringent MRI in their study, compared to that used in the present one, and this could explain the lower rejection rate of 0.56%, which they reported. 14 Tyrrell et al. 21 evaluated the effect of two different methods of demand management, i.e. implementation of MRI and use of a testing schedule, on requesting patterns in an intensive care unit. Implementation of MRI resulted in an overall 22.7% reduction in total requesting activity, whilst following the introduction of a testing schedule, a fall of 13.4% in such activity was observed. 21 Hutton et al. 19 examined CRP requesting patterns after implementing disease-related protocols, MRI and consultant only requesting. Implementation of these strategies resulted in an overall reduction of 85% in the number of requests, saving approximately £10,000 per annum. However, both these studies investigated the overall reduction of test requests and not rejection rates due to the implementation of these strategies per se.
Our second finding was that 14.7% of rejected tests were later restored by the requesting clinicians. This suggests that the majority of rejected tests were most probably unnecessary or not urgently needed for patient management. However, it is possible that some rejected tests were not restored but rather were repeated, especially if the turnaround time exceeded the MRI of the test. Thyroid function testing was by far the most frequently rejected test and only 2% of rejected thyroid function tests were subsequently restored. In our laboratory, TSH is the first-line test of thyroid function; consequently, all requests for free thyroxine and triiodothyronine made as part of a full thyroid function profile are rejected. However, if the TSH result is found to be abnormal, then free thyroxine will be performed as a reflex test without the need for telephonic authorisation to restore the test. This strategy may well therefore explain the low rate we observed for restored thyroid function tests.
The total cost-saving was calculated as £25,387 or 0.6% of the total hospital budget assigned to laboratory services. During the 2012/2013 financial year, £4.6 million was spent by TBH on laboratory services, which was 17.7% more than in the previous financial year. This particular annual increase is much larger than the usual 8% we observe annually. However, during the study period, there was a consolidation of laboratory services, which resulted in work from regional laboratories being sent to the central academic laboratory. This service re-configuration resulted in the unusually large increase in the service costs of the central laboratory. Other authors assessing the effect of test frequency filtering found a saving of 0.33% of total cost of testing with a rejection rate of less than 1%. However, as previously discussed, this study investigated a different test profile with a less stringent MRI. 14 Reductions in individual test volumes have a relatively small impact on the overall operating budget of a hospital. 7 However, laboratory tests are estimated to impact up to 70% of all medical decisions. 1 Consequently, the downstream costs of laboratory testing – both appropriate and inappropriate – are substantial. 7
We further found that in 80% of cases patient care was unaffected by eGK rejections, although this was very difficult to assess and relied on completeness of information in the case-notes. In 11% of the cases that we investigated, some impact was noted. Discharge was delayed in four patients but other factors may have contributed to this delay. The cost of an extra day in hospital should be weighed against the cost saved by the eGK. The impact of the test rejections on patient care may not always have been clearly documented and a platform where clinicians can report adverse events due to rejections should perhaps be considered. Although many articles were recently published on demand management, few have looked at the impact on patient outcomes. Wang et al. 22 assessed strategies to reduce unnecessary testing in a coronary care unit and found that reduced testing did not have any adverse effects on outcomes but the power of the study to assess outcomes was limited. Measuring clinical outcomes is difficult as the impact of changes in laboratory testing is unlikely to be sufficiently large to produce statistically significant changes in unequivocal endpoints such as death or hospitalisation, and surrogate endpoints are therefore needed. 13
In South Africa, approximately 3.5% of provincial budgets are directed towards meeting the costs of pathology services in the public sector. 23 Developing countries in particular need to look at demand management as a means to ensure appropriate utilisation of limited resources. South Africa has a large burden of disease due to a large prevalence of HIV/AIDS and tuberculosis, together with the rise in non-communicable diseases. Systems like the one described in this study could potentially reduce waste and redirect funds to where they are needed. The NHLS saw this opportunity and an eGK committee has since been established to examine the possibility of expanding this system to other pathology disciplines and eventually to all NHLS laboratories across South Africa to save cost in the public health-care system.
Our study has several limitations. Firstly, only chemical pathology test rejections from one site were investigated. Secondly, clinical impact was assessed by investigating patient case-notes, and this assessment relied on the completeness and availability of case-notes. Only patient case-notes from those patients for whom tests were restored were selected to assess clinical impact. This assumes tests that were not restored had no significant impact on patient care which might not be the case. Unfortunately, we did not look at the turnaround time after restoring a test. If this turnaround time was excessive, clinicians may have decided to repeat the test on a fresh specimen rather than ask for it to be restored and this could affect our findings. We calculated cost-saving by using charge per test not performed but did not take into account time and effort required to restore rejected tests. Finally, only those tests restored through following the correct procedure, i.e. by documenting the authorisation code on the laboratory information system, were extracted during the data-gathering exercise. This could have led to an underestimation of restored tests if this procedure was not always followed.
In conclusion, health-care systems are under immense pressure to reduce costs while still providing high-quality and efficient patient care. Laboratory services, which are an integral part of this health-care system, seem to be under even more pressure to reduce their costs. However, this is in the background of an inexorable year-on-year rise in laboratory workload. Demand management has been recognised as an important concept by which laboratories may reduce costs and eGK is an effective method of reducing unnecessary test requests and effectively managing demand. In the present study, we have shown that eGK can be successfully implemented in a large laboratory with minimal impact on patient care.
Footnotes
Acknowledgements
We would like to acknowledge Mr W Kleinhans for data mining and Mrs D Loubser and hospital administration for their assistance with regard to the laboratory budget.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
The study was approved by the ethical committees of the University of Stellenbosch (S14/03/052).
Guarantor
Prof. AE Zemlin.
Contributorship
All authors contributed to the planning, conduct and reporting of the work.