
Abstract
Background
To study the inter-practice regional variation in the request of urinary albumin by general practitioners and compare to guideline recommendations.
Methods
A cross-sectional study enrolled laboratories from different Spanish autonomous communities. Laboratories were invited to report the number of urinary albumin requested by general practitioners during 2012 and 2014. Urinary albumin requested per 1000 inhabitants and the index of variability (90th centile/10th centile) was calculated, and compared between autonomous communities and time periods. To investigate potential inappropriate requesting in the management of diabetes and arterial hypertension, the actual number of requests was compared to the theoretical, based on prevalence and guideline recommendations.
Results
Urinary albumin requested per 1000 inhabitants was similar for years 2012 and 2014 (78.2 (60.1) to 85.4 (55.4); P = 0.235), as was the variability index (4.6 for both). There were significant differences between autonomous communities, with the indicator ranging from 46.0 (33.1) to 125.8 (64.3) (P < 0.05). The theoretical cut-off ratios of urinary albumin per 1000 inhabitants to manage patients with diabetes and arterial hypertension were, respectively, 78 and 159; no laboratory reached both values.
Conclusions
Requesting of urinary albumin showed a significant regional variability in primary care in Spain, and was insufficient to correctly monitor patients with diabetes and arterial hypertension.
Introduction
The clinical laboratory intervenes in 70% of clinical decisions and is a major player in the overall patient care process. 1 The laboratory procedure is divided into a series of sequential steps that begins when the clinician requests the tests regarding a certain diagnostic suspicion and finishes when they interpret the laboratory report. The search for the best patient outcome from the laboratory requires optimization of each and every step of the procedure, or total testing process (TTP). The TTP consists of numerous steps across multiple providers 2 ; only the analytical phase falls under direct laboratory control, while the pre- and post-analytic phases pertain to different stakeholders such as the ordering clinician, the nurses, the patient and others involved in patient identification, data entry, specimen collection and transport.
It is the pre-pre analytical, test request, and post-post analytical, laboratory report interpretation that are subject to the most errors and must be optimized to provide a patient-centric laboratory model. 3
Previous REDCONLAB studies to compare laboratory test ordering in Spain showed high variability in the request for laboratory tests in primary care4,5 and significant inappropriate test requests.6–8 However, the use of urinary albumin (MAU) by general practitioners (GPs) in daily medical practice has not been previously studied.
Measurement of MAU is an important tool to diagnose and monitor disorders of the kidneys. Patients with diabetes and high blood pressure – two of the three most prevalent diagnoses in primary care 9 – are at risk of nephropathy. Total protein measurement is insufficiently sensitive to detect the onset of diabetic nephropathy and urine albumin must be used. 10 There is evidence that the latter is a more sensitive test to enable detection of glomerular disease associated with some systemic diseases as hypertension. 10 Guidelines for the correct use of MAU are clear in both types of patients: the test should be used as a diagnostic tool and then on an annual basis for monitoring.11,12 In the most common types of chronic kidney diseases, albumin is the most abundant protein in urine and the more sensitive marker of disease. The National Kidney Foundation – Kidney Disease Outcomes Quality Initiative (NKF-KDOQI), 13 National Institute for Health and Care Excellence (NICE) 2008 14 and Kidney Disease Improving Global Outcomes (KDIGO) 2012 15 guidelines recommend MAU measurement over total protein to detect and monitor proteinuria.
Increasingly, chronic kidney disease is being managed by GPs and other non-nephrologists. There is a need to design strategies of communication between GP and laboratories for a better management of chronic kidney disease. 16
However, how this test is really used in daily medical practice is still unknown. As a first step in the design of any strategy for a better test request, it is necessary to investigate the actual requesting pattern, 12 and if possible to compare data to a theoretical ideal request if guidelines were followed.
The aim of this research was, first, to study the inter-practice regional variability in the number of requests of MAU per 1000 inhabitants in primary care in Spain; second, to investigate temporal evolution in two different annual REDCONLAB studies; and finally compare the true request to that recommended by guidelines as a surrogate for inappropriate demand.
Materials and methods
Setting
Spain is divided into 17 Autonomous Communities (AACCs), also divided into Health Departments (HDs) – according to demographic and geographic criteria with the aim of ensuring proximity of services for users – that cover a geographic area and its population throughout the Public National Health System. HDs are composed of several primary care centres and usually a single Hospital. The laboratory located at the Hospital attends the needs of every HD inhabitant. Every Spanish citizen possesses an Individual Health Care Card, which let access to public health services as a healthcare user throughout the National Health System.
Data collection
A cross-sectional study was designed and conducted at the University Hospital of San Juan de Alicante. In REDCONLAB 2012, a call for data was posted via email. As in the previous studies, Spanish laboratories willing to participate were invited to fill out an enrollment form and submit their results online. A questionnaire was addressed to the participants of previous studies of the REDCONLAB group that recommended other laboratories to join the current study. In 2014, the questionnaire was also addressed to the participants of previous REDCONLAB studies and a LinkedIn group was created (https://www.linkedin.com/in/redconlab-grupo-a5663bb7).
The numbers of MAU requested by the GPs for the years 2012 and 2014 from laboratories at different HDs across Spain were reported in both studies. Each participating laboratory was required to deliver data from local Laboratory Information Systems Patient’s databases and to provide data about the organization.
Data processing
Rates were expressed as number of tests per 1000 inhabitants in the HD. The index of variability was calculated as the top decile divided by the bottom decile (90th percentile/10th percentile). Results for both studies were compared. To the 2014 edition joined 10 AACC with more than 4 participants (in alphabetical order: Andalucía, Canarias, Castilla La Mancha, Castilla Leon, Extremadura, Galicia, Madrid, Murcia, País Vasco and Valencia). An 11th group was created with those AACCs that did not reach the 4 participants (in alphabetical order: Aragon, Asturias, Baleares, Cantabria and Cataluña). AACCs were codified by numbers to maintain confidentiality.
To investigate whether MAU was appropriately requested in the management of patients with diabetes and arterial hypertension, we compared the true request rate to the theoretical ideal value according to the prevalence of diabetes (6.98.1%) 17 and arterial hypertension (15.9%) 17 in Spain and according to guideline recommendations (MAU test at least once a year), taking into account the demographics of the Spanish population. 18
Statistical analysis
All analyses were performed using SPSS Inc. for Windows, Version 21.0 (Chicago, SPSS Inc.). Descriptive statistics were generated for test-utilization rates. The analysis of the distribution of the number of test requests per 1000 inhabitants was conducted by way of the Kolmogorov–Smirnov test. When there were potential differences in MAU request between AACCs, paired differences were evaluated by way of the U–Mann Whitney test.
In order to explore the variability through test-utilization rates comparison, the index of variability was used.
A two-sided P ≤ 0.05 rule was utilized as the criterion for rejecting the null hypothesis of no difference.
Results
Seventy-six laboratories participated in the 2012 REDCONLAB study, corresponding to a catchment area of 17,679,195 inhabitants; 110 laboratories from 15 AACCs participated in the 2014, corresponding to 27,798,262 inhabitants, or 60% of the Spanish population.
Descriptive analysis of urinary albumin (MAU) request in both REDCONLAB editions.
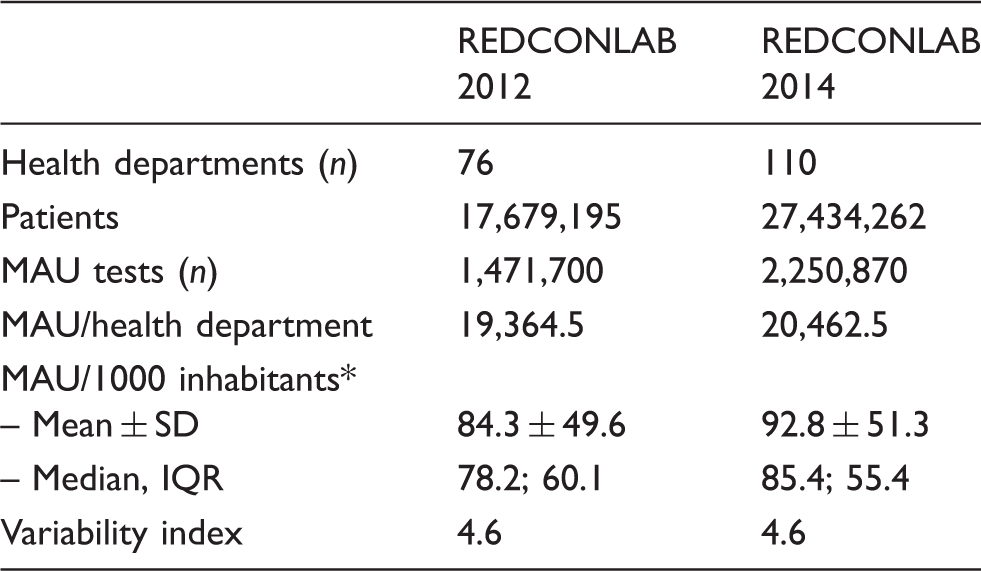
MAU: urinary albumin.
P = 0.235.
According to guidelines and disease prevalence data, 1,378,977 and 2,810,992 MAU would have been necessary to manage diabetes and arterial hypertension in our patient cohort for year 2012, and 2,168,264 and 4,419,924 in 2014. That results in theoretical cut-off ratios of 78 and 159 tests per 1000 inhabitants for a correct management of diabetes and hypertension.
Figure 1 displays the request for MAU in each HD, as number of tests per 1000 inhabitants, for both study editions, and compares graphically the actual demand to the theoretical data; 38 and 56 laboratories reached the threshold to manage diabetes and only 4 and 11 the arterial hypertension goal, in 2012 and 2014 respectively. Not a single laboratory reached both theoretical cut-offs.
(a) Rate of requests of urinary albumin (MAU) per 1000 inhabitants by Health Department (HD) for the 2012 REDCONLAB edition. Column chart displaying the number of MAU requests per 1000 inhabitants for the 2012 REDCONLAB edition. Horizontal lines display the theoretical values for diagnosis and management of diabetes and arterial hypertension (HBP). (b) Rate of request of urinary albumin (MAU) per 1000 inhabitants by Health Department (HD) for the 2014 REDCONLAB edition. Column chart displaying the number of MAU requests per 1000 inhabitants for the 2014 REDCONLAB edition. Horizontal lines display the theoretical values for diagnosis and management of diabetes and arterial hypertension (HBP).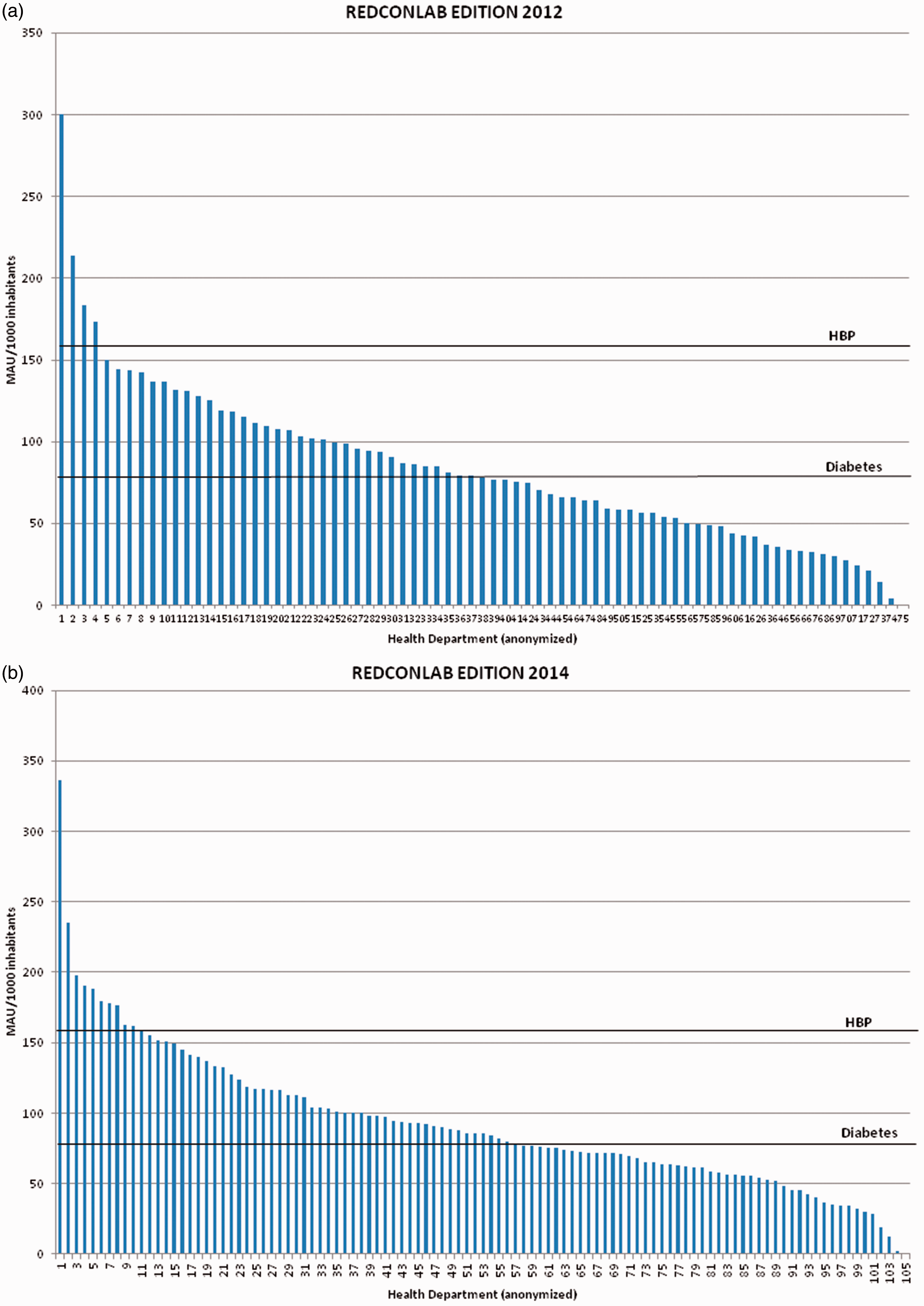
Ten AACCs had more than four participants and six did not reach the four contributors and are grouped in the 11th group. The request per 1000 inhabitants was significantly different in the 11 different groups, with medians ranging from 46.0 to 125.8 (P < 0.05) (Figure 2).
Urinary albumin (MAU) per 1000 inhabitants indicator results in different autonomous communities (AACCs). Boxplot for urinary albumin (MAU) per 1000 inhabitants indicator results regarding autonomous communities (AACCs). There are significant differences (P < 0.05) between AACC 1 and the rest of AACC (except AACCs 8, 10 and 11); between AACC 4 and the rest of AACC (except 6, 7 and 9); and between AACC 3 and AACC 10.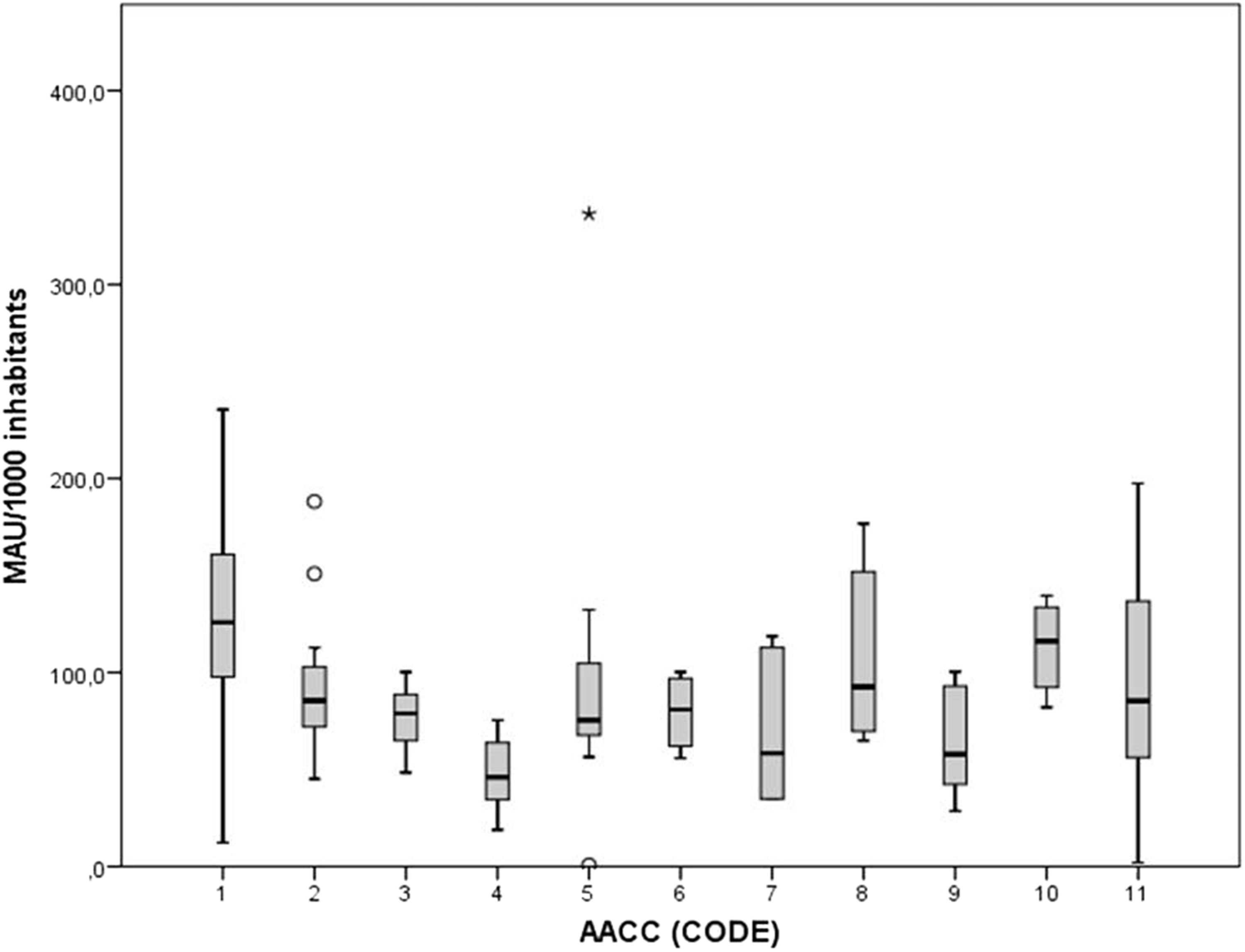
Discussion
There was a high regional variability in the request of MAU in primary care. The reasons behind such regional variability are unclear. The results do not seem to be affected by differences in patients’ accessibility to medical service, as enrolled clinical laboratories belong to the Spanish National Health Service, and all applicable residents have free access to their primary care physician and to the hospital. 19
The rate of request was similar in both studies and was insufficient to meet the guideline recommendations to properly manage patients with diabetes and arterial hypertension. Although there is an overlap between the two conditions, the request of MAU seemed low when compared to current recommendations. Furthermore, MAU is also used in additional medical conditions which have not been taken into account in our study. Despite the established recommendations, the request rate did not increase over the years.
The role of laboratory tests has evolved over time, currently providing important tools not only to diagnose but also to manage chronic, progressive illness. Diabetes and arterial hypertension are very prevalent conditions and two of the most frequent indications for laboratory testing in primary care, 9 representing 11.3% of the total. There is a need to improve the requesting of laboratory tests in both conditions through the design and establishment of interventions to solve the under-requesting through laboratory test utilization programs. 20
Our results show once again that we can learn from studies on regional differences in the use of laboratory tests 21 and suggest a need for interventions for a better request.
The study had some limitations. The regional differences in the request of MAU could be partly explained by case mix variations in the different areas, the possible variability in the patient population or by different degrees in the management of chronic and kidney disorders in primary care. A second limitation is the potential difficulty in the generalization of our results to non-public environments, with no specific population or inhabitants to be covered. Finally, we do not know the number of patients with regular HbA1c measurements as this would have allowed some view on the diagnostic efficiency in the different AACC's and also provided information about the relative efficiency of practices in terms of how well the identified diabetics are treated.
Conclusions
The request of MAU showed a significant regional variability in primary care in Spain and was insufficient to correctly monitor patients with diabetes and hypertension.
Footnotes
Acknowledgements
Members of the REDCONLAB working group are the following: Vidal Perez Valero (Hospital Regional Universitario de Malaga, Hospital Universitario Virgen de la Victoria, Malaga); Félix Gascón (Hospital Valle de los Pedroches, Pozoblanco); Isidoro Herrera Contreras (Complejo Hospitalario de Jaen); Maria Angeles Bailen Garcia (Hospital Universitario Puerta del Mar de Cadiz); Cristobal Avivar Oyonarte (Hospital de Poniente, El Ejido); Esther Roldán Fontana (Hospital La Merced, AGS Osuna); Fernando Rodriguez Cantalejo (Hospital Universitario Reina Sofia de Cordoba); Jose Angel Noval Padillo (Hospital Universitario Virgen del Rocio); M Angela Gonzalez García (AGS Norte de Cadiz); Ignacio Vazquez Rico (Hospital Juan Ramon Jimenez de Huelva); Cristina Santos (Hospital Rio Tinto); Angeles Giménez-Marín (Hospital de Antequera); Maria del Señor López Vélez, Jose Vicente García-Larios (Hospital San Cecilio de Granada, Hospital Virgen de las Nieves, Granada); Federico Navajas Luque (AGS Este de Málaga-Axarquía); Amado Tapia (Hospital de Barbastro); Maria Esther Sole LLop (Hospital de Alcañiz); Juan José Puente (Hospital Clínico Universitario Lozano Blesa); Patricia Esteve (Hospital Ernest Lluch); Maria Teresa Avello Lopez (Hospital San Agustín-Aviles, Hospital Valle del Nalon); Emilia Moreno Noguero (Hospital Can MIsses); Ana Maria Follana Vazquez (Hospital Mateu Orfila); Jose Luis Ribes Valles (Hospital de Manacor); Ma Luisa Fernández de Lis Alonso (Area de Salud de Fuerteventura); MC Martin-Fernandez de Besoa (Hospital Nuestra Señora de la Candelaria, Tenerife); Leopoldo Martin Martin (Hospital General de la Palma); Miguel Angel Pico Picos (Hospital Universitario de Canarias); Casimira Dominguez Cabrera (Hospital Universitario de Gran Canaria Dr Negrín); Marta Riaño Ruiz (Hospital Insular de Gran Canaria); Juan Ignacio Molinos (Hospital Sierrallana de Torrelavega); Luis Fernando Colomo (Hospital de Laredo); Jose Carlos Garrido (Hospital Universitario Marques de Valdecilla); Enrique Prada de Medio (Hospital Virgen de la Luz de Cuenca); Pilar Garcia Chico (Hospital General Universitario de Ciudad Real); Simon Gomez-Biedma (Hospital General de Almansa); Jesús Dominguez (Hospital Universitario de Guadalajara); Antonio Menchem (Complejo Hospitalario de Toledo); Laura Navarro Casado (Complejo Hospitalario Universitario de Albacete); Fidel Velasco Pena (Hospital Virgen de Altagracia, Manzanares); Carolina Andrés Fernandez (Hospital General de Villarobledo); Ma Carmen Lorenzo Lozano (Hospital Santa Bárbara de Puertollano); Joaquín Domínguez Martinez y Oscar Herrera Carrera (Hospital General Mancha Centro y Hospital General de Tomelloso); Maria Teresa Gil (Hospital Nuestra Señora del Prado Talavera de la Reina); Ma Angeles Rodriguez Rodriguez (Complejo Asistencial Universitario de Palencia (Hospital Rio Carrion)); M. Victoria Poncela Garcia (Hospital Universitario de Burgos); Luis Rabadan (Complejo Asistencial de Soria); Vicente Villamandos (Hospital Santos Reyes, Aranda del Duero); Nuria Fernandez Garcia (Hospital Universitario Rio Hortega-Valladolid); Jose Miguel Gonzalez Redondo (Hospital Santiago Apostol de Miranda de Ebro); Cesareo Garcia (Hospital Universitario de Salamanca); Luis Garcia Menendez (Hospital El Bierzo); Pilar Alvarez Sastre (Complejo Asistencial de Zamora); María Dolores Calvo Nieves (Hospital Clínico Universitario de Valladolid); María Isabel Llovet (Hospital Universitario Verge de la Cinta (Tortosa)); Nuria Serrat (Hospital Joan XXIII de Tarragona); Ma José Baz (Hospital de Llerena, Badajoz); Maria Jose Zaro (Hospital Don Benito-Villanueva); M Carmen Plata (Hospital Campo Arañuelo, Navalmoral de la Mata); Pura Garcia Yun (Área de Salud de Badajoz (Hospital Infanta Cristina, Hospital Perpetuo Socorro y Hospital Materno Infantil)); Milagrosa Macías Sánchez (Area de Salud de Caceres (Complejo Hospitalario San Pedro de Alcantara)); Ma Montaña Jimenez (Hospital Virgen del Puerto de Plasencia); Lola Máiz Suarez (Hospital Lucus Augusti, Lugo); Berta Gonzalez Ponce (Hospital Da Costa, Burela); Aida Perez Fuertes (Hospital Arquitecto Marcide, El Ferrol); M. Amalia Andrade Olivie (Hospital Xeral-Cies, CHU Vigo); Pastora Rodriguez (Hospital Universitario de A Coruña); M. Mercedes Herranz Puebla (Hospital General Universitario Gregorio Marañon); Antonio Buño Soto (Hospital Universitario La Paz, Madrid); Fernando Cava (BR Salud); Tomas Pascual (Hospital Universitario de Getafe); Carmen Hernando de Larramendi (Hospital Severo Ochoa de Leganes); Raquel Blázquez Sánchez (Hospital de Mostoles); Pilar Díaz (Hospital 12 de Octubre, Madrid); Ana Díaz (Hospital Universitario de La Princesa); Marta Garcia Collia (Hospital Ramon y Cajal, Madrid); Maria Angeles Cuadrado Cenzual (Hospital Clinico Universitario San Carlos); Santiago Prieto Menchero (Hospital Universitario de Fuenlabrada); María del Carmen Gallego Ramírez (Hospital Rafael Mendez, Lorca); Jose Luis Quilez Fernandez (Hospital Universitario Reina Sofia de Murcia); Maria Dolores Albaladejo (Hospital Santa Lucia, Cartagena); Maria Luisa Lopez Yepes (Hospital Virgen del Castillo de Yecla); Alfonso Pérez Martínez (Hospital Morales Meseguer); Antonio López Urrutia (Hospital de Cruces, Bilbao); Adolfo Garrido Chércoles (Hospital Universitario de Donostia); Carmen Mar Medina (Hospital Galdakao-Usonsolo); M Carmen Zugaza (Unidad de Gestion Clinica de Alava); Francisco Javier Aguayo gredilla (Hospital Universitario de Basurto); Silvia Pesudo (Hospital La Plana); Carmen Vinuesa (Hospital de Vinaros); Julian Díaz (Hospital Francesc de Borja, Gandia); Marisa Graells (Hospital General Universitario de Alicante); Diego Benitez Benitez (Hospital de Orihuela); Arturo Carratala (Hospital Clinico Universitario de Valencia); Consuelo Tormo (Hospital General de Elche); Francisco Miralles (Hospital Lluis Alcanyis, Xativa); Amparo Miralles (Hospital de Sagunto); Jose Luis Barberà (Hospital de Manises); Juan Molina (Hospital Comarcal de La Marina, Villajoyosa); Martin Yago (Hospital de Requena); Mario Ortuño (Hospital Universitario de la Ribera (Alzira)); Maria Jose Martinez Llopis (Hospital de Denia); Nuria Estañ (Hospital Dr. Peset); Ricardo Molina (Hospital Virgen de los Lirios, Alcoy); Juan Antonio Ferrero (Hospital General de Castellon); Begoña Laiz Marro (Hospital Universitario y Politecnico La Fe de Valencia); Goitzane Marcaida (Consorcio Hospital General Universitario de Valencia)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
MS.
Contributorship
MS, ML-G, EF, and CL-S conceived, designed and drafted the manuscript; MS, ML-G, EF and CL-S revised the final manuscript. All authors contributed to the concept, reviewed all versions of the manuscript and commented, and approved the final revised version of the manuscript.