
Abstract
Introduction
The ASSIST-CKD project is a national quality improvement programme, aiming to decrease the number of patients presenting late to renal services by enabling laboratories to review up to five years of estimated glomerular filtration rate results graphically and report deteriorating patients to their general practitioner.
Aim
To assess the impact of the project on the laboratory, and of patient reporting on general practitioner management and the local renal service.
Method
Each week two searches were performed (Search A: maximum age 65 years, maximum eGFR 50 ml/min/1.73 m2 and Search B: Age 66–120 years, maximum eGFR 40 ml/min/1.73 m2) on patients with an estimated glomerular filtration rate requested by their general practitioner within the previous seven days. Patients showing deterioration in estimated glomerular filtration rate had a printed graph sent to their general practitioner. Feedback on the graphs and their impact on patient management were obtained from the general practitioners via a questionnaire.
Results
A median of 37 patients/week were listed for review for Search A, with 32% reported; and Search B a median of 227 patients/week listed, 32% reported. General practitioner surgery questionnaires (29) showed the reports were well received. Of general practitioners responding to the questionnaire, 67% had reviewed a patient earlier than intended, 54% had reviewed local guidance, 48% had emailed the renal team and 48% had referred a patient on receipt of a graph; 34% had shown a graph to their patients, of whom 70% found that useful.
Conclusion
There is some evidence that ASSIST-CKD reporting has enhanced patient care; however, further long-term assessment is still required.
Introduction
Chronic kidney disease (CKD) is a common long-term condition that affects 6–7% of adults in the United Kingdom (UK) in its moderate to severe stages.
1
CKD is associated with an increased risk of cardiovascular disease
2
and progression to end-stage kidney disease.
3
Outcomes are particularly poor in those presenting late to renal services within secondary care, as there is insufficient time to prepare patients adequately for renal replacement therapy (RRT). The risk of death in patients presenting late is approximately doubled, compared with those referred earlier.
4
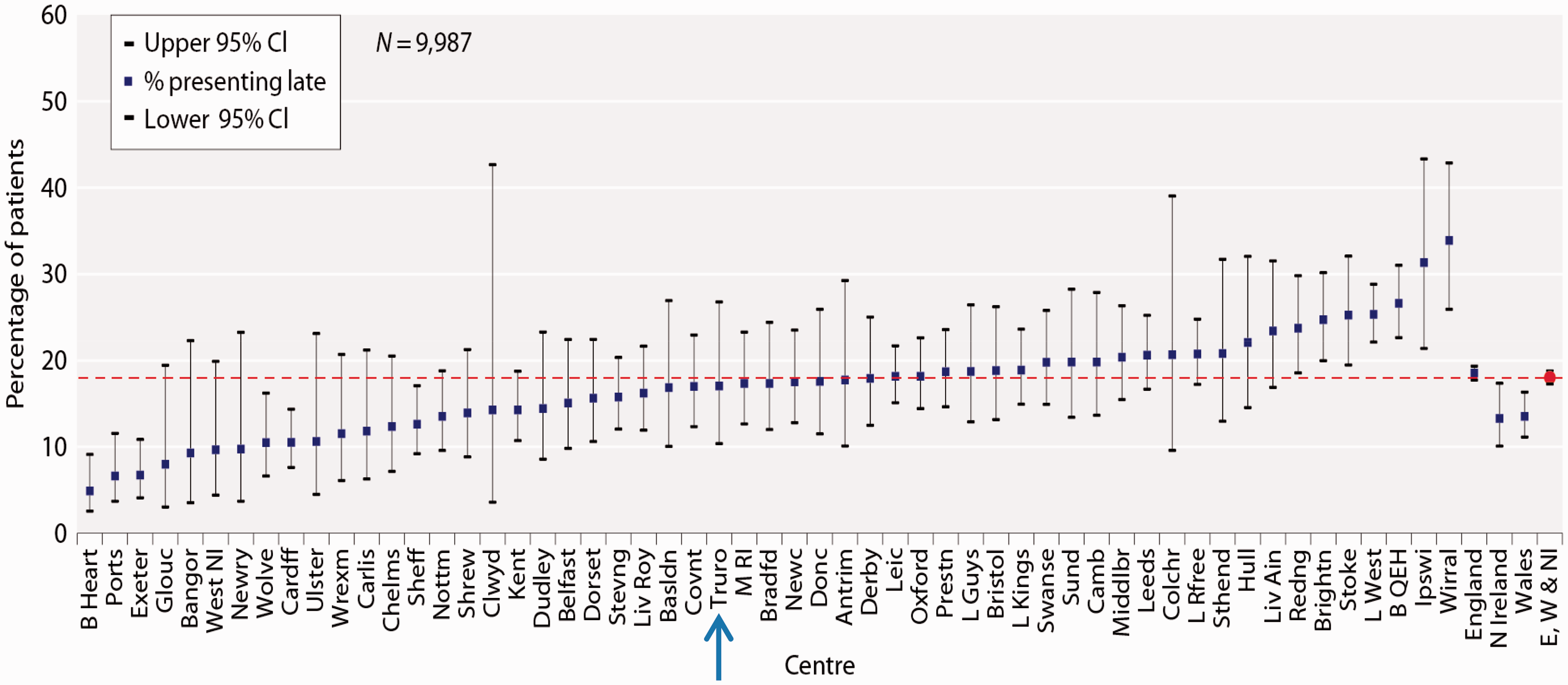
Data from the UK Renal Registry show major meaningful variation in late-presenting rates (applied to patients who are first seen at a renal centre less than 90 days before starting RRT). In 2013–2014, this proportion varied across UK renal centres from 4.9 to 33.9%
5
(Figure 1). Spreading and sharing best practice from high performing centres in order to reduce this variation is therefore an appropriate focus for quality improvement activity.
Late referral rates to renal units in England, Northern Ireland and Wales, 2013–2014, including Truro.
5
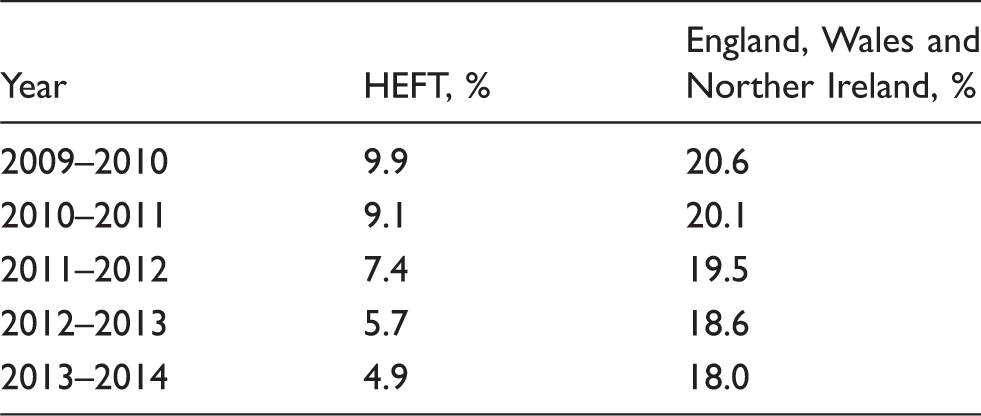
The percentage of patients referred late for dialysis in the Heart of England Foundation Trust (HEFT) compared with other areas of the UK. 5
ASSIST-CKD (A programme to Spread eGFR graph Surveillance for the early Identification, Support and Treatment of people with progressive Chronic Kidney Disease) is a national quality improvement project, funded by the Health Foundation, in which the HEFT eGFR graph intervention will be rolled out to laboratories serving up to 19 renal units across the UK. The programme has the potential to be highly cost-effective, implementing the service at a site covering a population of 800,000 costs approximately £10–12,000 per year, as compared with the annual cost of dialysis for one person of over £25,000, which can rise to over £30,000 if additional costs such as hospital transport are included. 9
In August 2015, the Clinical Chemistry laboratory at the Royal Cornwall Hospital (RCH) was the first laboratory in the UK to go live with the project. As such, we were keen to study the impact on the laboratory service, the GPs, the renal team and patients. Since any benefits on late presentation rates, and in particular dialysis, will not be immediately apparent, in the current report, we have focused on shorter term effects. We specifically looked at the impact on patients by asking the GPs if the ASSIST-CKD reports had influenced their patient management and also checked whether the renal team had seen any changes in the numbers of GP queries and referrals.
Aim
To collate data on the number of patients being reviewed by the clinical biochemists per week and the time ASSIST-CKD took to perform, as well as the number of patients flagged. To assess the impact of ASSIST-CKD patient reporting on GPs, the management of their patients and, in turn, any impact on the local renal service.
Methods
Population
The Clinical Chemistry laboratory at RCH covers Cornwall (population of approximately 532,300), 10 serving one main acute hospital, two peripheral hospitals and six community hospitals, including one renal unit, as well as 68 GP surgeries (including branches) that have a catchment population of approximately 453,000. 11 Population demographics are 22% aged 0–19 years, 57% aged 20–65 years, 19% aged 65–84 years and 3% aged ≥85 years old. 10
ASSIST-CKD implementation, searching and reporting protocol
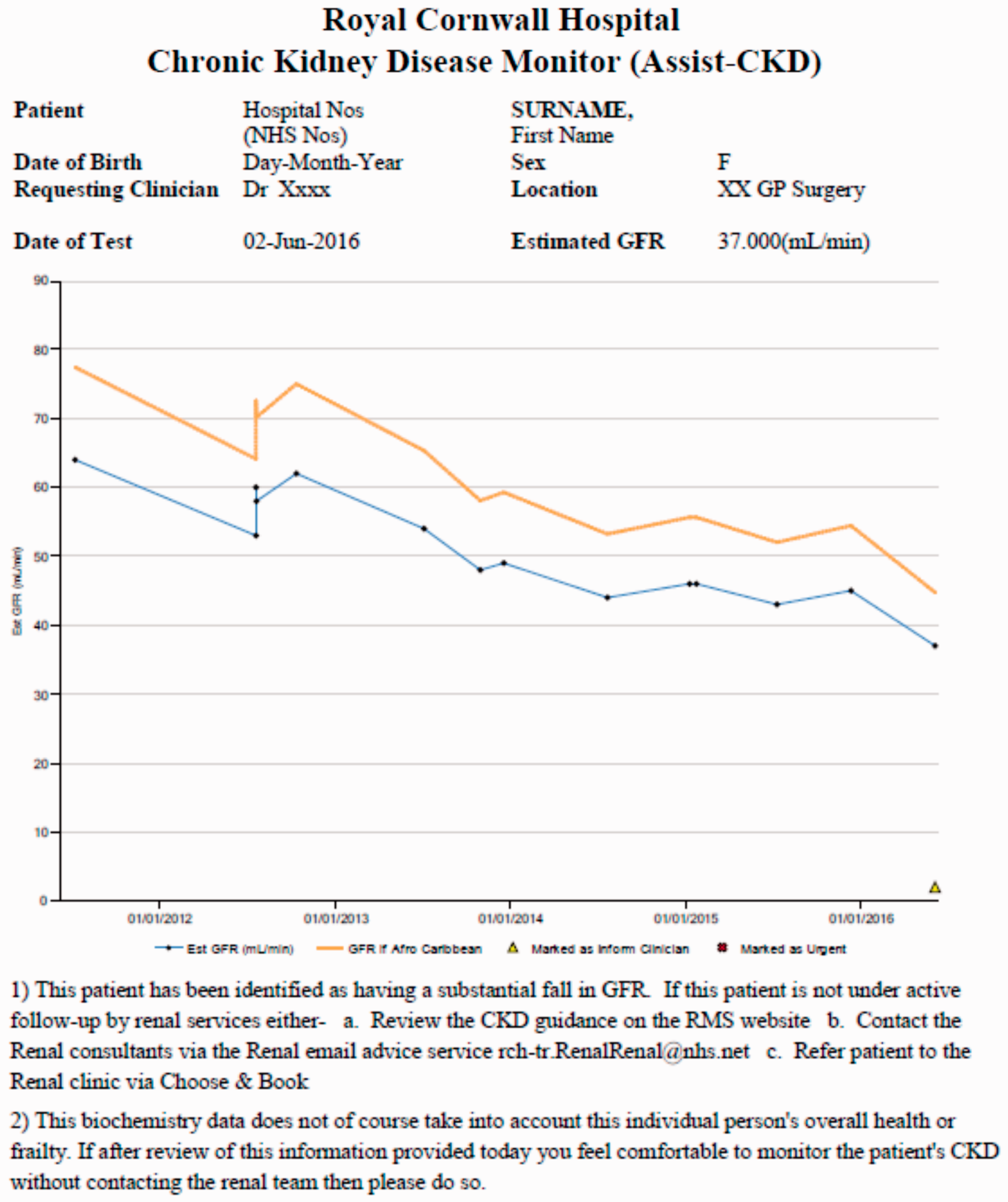
In August 2015, the Chronic Kidney Disease Monitor (ASSIST-CKD) programme (version 1) was installed and, in order to provide full patient history, every eGFR (calculated by MDRD, and, from June 2015, CKD-EPI equation) reported in the previous five years on patients ≥18 years old by our laboratory was uploaded. Patient history was kept up-to-date by means of a weekly automated download, from the Winpath (Clinisys, Chertsey, UK) Laboratory Information Management System (LIMS) of all the eGFRs reported in the previous seven days. These were then manually uploaded into the ASSIST-CKD programme by a clinical biochemist. Every week, two patient searches were performed as per the ASSIST-CKD protocol (Figure 2) on patients who have had an eGFR requested by their GP. The search dates were set to end with the Sunday just prior to the search being performed, and starting with the Sunday prior to that (i.e. seven-day search window). For each patient who met the criteria, the ASSIST-CKD programme created a five-year graph of all their results. Every patient graph (for Search A and Search B) was reviewed, and both long-term trends (i.e. across five years), and shorter term changes were noted. Patients whose eGFR trend met the ASSIST-CKD criteria (Figure 2) were flagged as ‘inform clinician’ which added a triangle to the eGFR graph; graphs were created (Figure 3), printed and sent to the GPs. These included advice from the renal team including where to find local guidelines and how to contact them. On 11 January 2016, version 2 of the programme was installed, which included repairs to reported glitches and other improvements to the programme.
A flow diagram of the methodology for searching and reporting GP patients, as per the ASSIST-CKD project. An ASSIST-CKD graph-report with patient identification removed.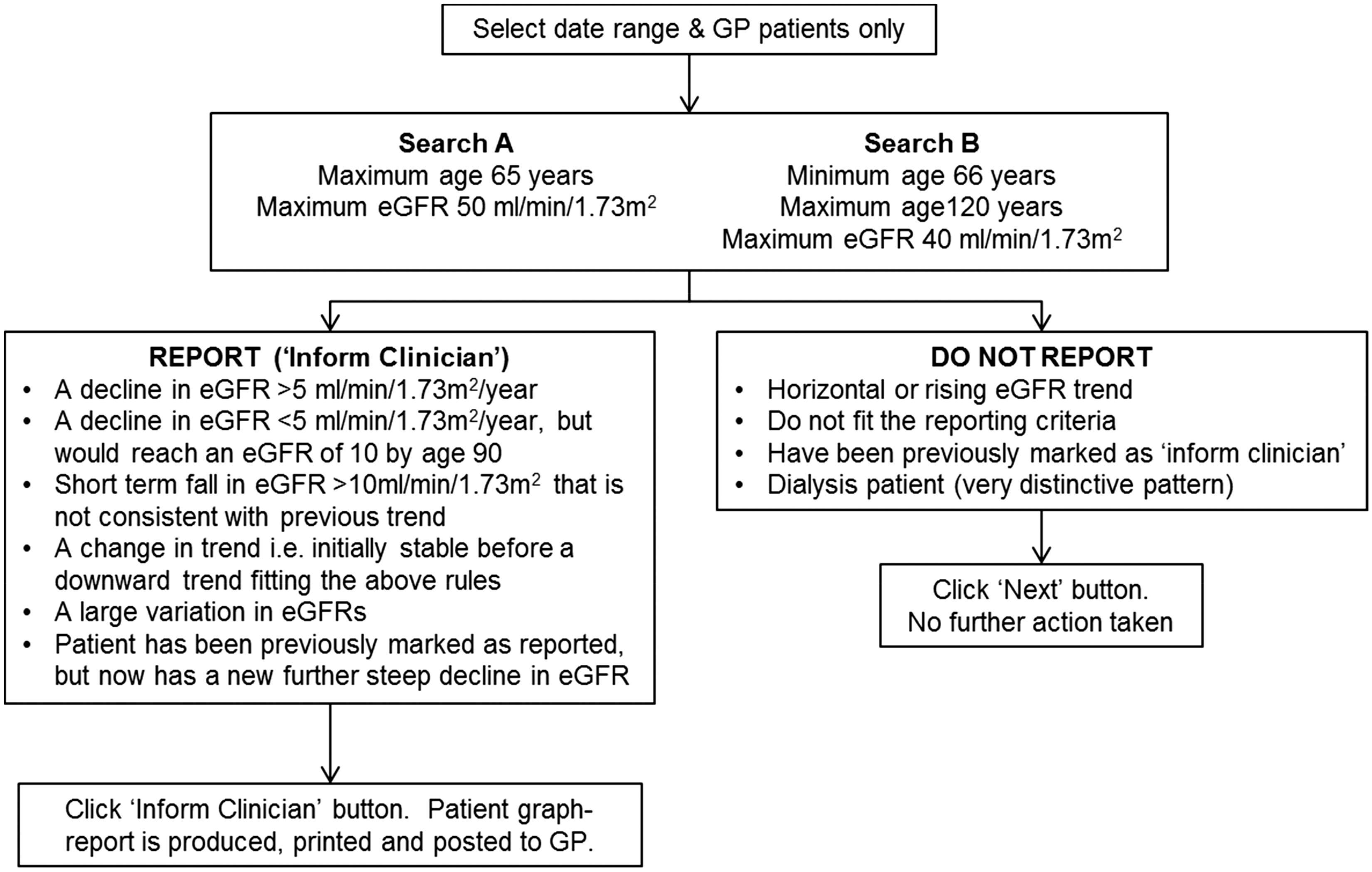
ASSIST-CKD laboratory data
Every week, the clinical biochemist who performed the ASSIST-CKD searches recorded the number of patient files extracted for both Search A and Search B, the number they flagged as ‘inform clinician’ and the time it took to do each run. The collected data was evaluated for the 17 weeks covering patient search dates 3 January to 1 May. Furthermore, two searches were performed using the ASSIST-CKD programme for the same time period, using Search A and Search B patient criteria, which were then filtered by those flagged as ‘inform clinician’. The patient data were transferred to Excel (Version 14, Microsoft Corporation®) for statistical analysis of gender, age and eGFR.
GP survey
In December 2015, four months after starting the ASSIST-CKD project, a questionnaire was created and posted to all 68 GP surgeries covered by our laboratory. In February 2016, a second printout was sent out to all the non-responding surgeries. The questionnaire included a short summary of the ASSIST-CKD service, 14 questions to be completed (multiple choice and a few free text) and the reason for the questionnaire being sent. Questions covered four main areas. First, were the ASSIST-CKD graphs sent to the GPs clear and easy to understand, and was the information provided on the reports useful? Second, after receiving a report did the GPs look up local CKD guidelines, contact the renal team by email or phone, and/or refer patients? Additionally, did receiving ASSIST-CKD reports make them review patients earlier than intended, and did it have an impact on the way the GPs review long-term changes in their patient’s renal function? Third, had the GPs shown any graphs to patients, and did they or their patient find it useful? Finally, would they prefer electronic reporting of the graphs in the future? The questionnaire also contained opportunity for responders to provide free text feedback. All data from the responses were collated into Excel.
Renal team feedback
In May 2016, the renal team were asked to provide formal feedback on the impact they felt the ASSIST-CKD reporting had on email/phone/letter queries and also on clinic referrals.
Results
ASSIST-CKD laboratory data
The clinical biochemist’s log for the service performed over the 17-week period showed a median of 37 patients listed for review per week for Search A, with 12 (32%) being flagged as ‘inform clinician’; a median time of 8 min/week was taken to perform the patient search and review all the graphs. Search B had a median of 227 patients listed per week, with 72 (32%) being flagged, and taking a median time of 40 min/week to perform the patient search and review all graphs. Therefore, altogether 264 patients per week were listed by the two ASSIST-CKD search criteria as requiring review, taking approximately 48 min to perform. Further time was required for the ASSIST-CKD programme to collate the ‘inform clinician’ patient list and convert into individual patient graphs; and then for these to be printed and sorted for posting.
The ASSIST-CKD data retrieval for the period from Sunday 3 January to Sunday 1 May using Search A criteria listed 470 patients, of which 201 (43%) were flagged as ‘inform clinician’. Of these, 51% were female, with an age range of 23 to 65 years (median: 59), an eGFR range of 2–50 (median: 42) and spanning 54 GP requesting locations. Search B criteria listed 3098 patients, of which 1153 (37%) were flagged. Of these, there was an equal gender split (50% female), with an age range of 66 to 101 years (median: 81), eGFR range of 2–40 (median: 33) and spanning 62 GP locations.
GP survey
A summary of the questionnaire questions and breakdown of the answers provided.
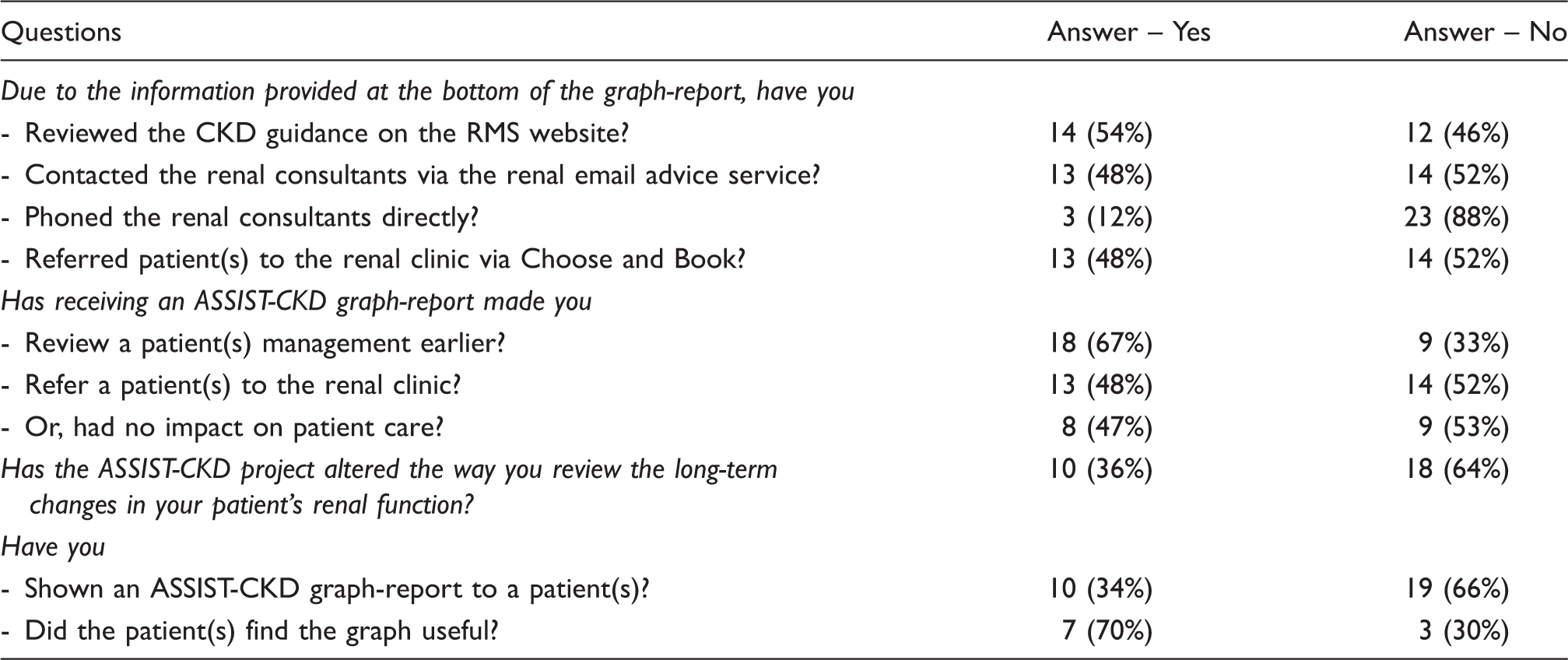
RMS: referral management system.
Renal team feedback
Feedback was sought from the renal team who deemed that the ASSIST-CKD project had been successfully introduced. An innovative emailing system allowing GPs and other healthcare professional easily and quickly to contact the renal consultants for advice had been in place since 2010; this email point of contact was included in the ASSIST-CKD patient reports. In the initial few weeks of the project, there was an influx of general inquiries from GPs via email (1–2 per week) on patients who had been identified; and informative and supportive information was provided. Furthermore, in response to the queries the information provided on the reports was amended to state that the ASSIST-CKD report was based on biochemistry data and so did not take into account the current status or management of the patient, accordingly the number of queries fell. The renal team believe that the GPs have used the ASSIST-CKD reports and the information provided on them (on seeking local guidance, using the email service and/or referring patients) sensibly, and in some cases, this has prompted referrals to the renal clinic. Likewise, in many other cases, GPs have continued to manage patients in primary care, sometimes after seeking support and advice from the email advice line. There does not appear to have been an increase or decrease in the number of new patient referrals to the renal department since the introduction of ASSIST-CKD nine months ago.
Discussion
The Clinical Chemistry laboratory at RCH was the first laboratory in the UK to go live with the ASSIST-CKD project. The previous HEFT project, that had run for over ten years, had suggested that alerting GPs to long-term falls in eGFR could delay the requirement for dialysis/transplantation, and/or over time reduce the number. 6 The ASSIST-CKD project is designed to cover the UK (19 renal units) in order to collate further data and to analyse the impact of flagging patients with deteriorating eGFR. 8 However, changes to dialysis or transplantation numbers or trends will take a few years to be seen. We therefore wanted to find out what the short-term impact was, particularly to try to assess the reaction of GPs to the new service, including any benefits or downfalls, the impact on the renal team and on the laboratory providing the service. These were all areas that have not been previously examined in detail.
Our laboratory, which covers a GP catchment of approximately 453,000 patients, listed each week a median of 264 patients to review as per the ASSIST-CKD criteria. It took a median of 48 min to search for the patient and then review all the eGFR graphs, of which 32% were flagged as ‘inform clinician’ by the clinical biochemist. There was variation in the median age and eGFR, even though the gender split was similar for both sets of search criteria. The variation in the percentage of patients recorded as flagged ‘inform clinician’ in the clinical biochemist’s log (Search A: median 37 reviewed with 12 (32%) flagged and Search B: median 227 reviewed with 72 (32%) flagged) vs. the ASSIST-CKD data-pull (Search A: median 470 reviewed with 201 (43%) flagged and Search B: median 3098 reviewed with 1153 (37%) flagged) is possibly due to the latter taking into account flagged patients that met the search criteria, but the flagging was performed prior to the search time window.
The GP questionnaire found that the ASSIST-CKD reporting was having an impact on patient care within months; with 67% of GPs reporting that the ASSIST-CKD graph reports had prompted them to review a patient earlier than planned and 48% had referred a patient. However, 47% of responders also selected that there had been no impact on management. The main port of call for advice post-receipt of a graph was the local CKD guidelines (54%), followed by contacting the renal team via email (48%), referring a patient (48%) or contacting the renal team by phone (12%). The feedback on the graphs was positive with 97% finding them clear and easy to read, and 71% finding the text information useful. Also 31% of the free text comments were positive and another 31% considered neutral. Another element of the graphs is that they lend themselves to being shown to a patient, with 34% of GPs responding to say they had done this and 70% of those finding it useful.
We found the feedback of the renal team to be very positive. After an initial flurry of queries after the initiation of the intervention, it settled down. Some of this may be due to the long-established renal service email system at RCH and also to the flexibility of changing the information on the ASSIST-CKD graphs.
Conclusions
We have found that ASSIST-CKD reporting is already having an impact on patient care in the short time that we have been reporting since August 2015. The ASSIST-CKD project team are continuing to roll out the project to another 18 sites around the country, and further assessment to the impact on both short-term and long-term patient care and outcome will be evaluated.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by ASSIST-CKD (via a Health Foundation grant) for a one year pilot.
Ethical approval
Not applicable.
Guarantor
AB.
Contributorship
AB and AM set up the ASSIST-CKD project at RCH. AB, AM and AP performed the weekly ASSIST-CKD searches and completed the clinical biochemist’s log. AB conceived the idea for and wrote the article, created the questionnaire and collated the data; collated the clinical biochemist’s log data; and also performed and collated the data for the ASSIST-CKD data-pull. SD was the renal liaison and also provided the renal feedback. NT and HG wrote the introduction on behalf of the ASSIST-CKD team. All authors reviewed and edited the paper, and all were in agreement on its submission.