
Abstract
Background
Measurement of plasma metanephrines is regarded as one of the best screening tests for phaeochromocytoma/paraganglioma. Current guidelines recommend that samples are ideally collected in the supine position after 30 min rest and interpreted using supine reference ranges, in order to optimize the diagnostic performance of the test. Current practice in our centre is to collect samples for plasma metanephrines from seated patients. The aim of the study was to determine, if seated sampling for plasma metanephrines provides acceptable diagnostic performance in our centre.
Methods
Clinical and laboratory data of 113 patients, gathered over a four-year period 2010–2014, were reviewed. All had undergone preoperative plasma metanephrines measurement and had postoperative histopathology confirmation or exclusion of phaeochromocytoma/paraganglioma.
Results
Of 113 patients included in the study, 40 had a histological diagnosis of phaeochromocytoma/paraganglioma. The remaining 73 patients had an alternative adrenal pathology. The diagnostic sensitivity of normetanephrine or metanephrine above the upper limit of our in-house seated reference range was 93%. However, excluding three cases of paraganglioma determined clinically and biochemically to be non-functional raised the sensitivity to 100%. Diagnostic specificity was 90%. Applying published supine reference ranges made no difference to diagnostic sensitivity in this group of patients but decreased diagnostic specificity to 75%.
Conclusions
While these data are derived from a relatively small study population, they demonstrate acceptable diagnostic performance for seated plasma metanephrines as a screening test for phaeochromocytoma/paraganglioma. These data highlight a high diagnostic sensitivity for plasma metanephrines with seated sampling in our centre.
Introduction
The measurement of plasma metanephrines is widely recognized as one of the best screening tests for phaeochromocytoma/extra-adrenal paraganglioma (P/PGL).1–4 The higher diagnostic sensitivity of the measurement of metanephrines compared with catecholamines or catecholamine metabolites is thought to be due to their continuous production within phaeochromocytomas owing to the presence of high concentrations of catechol-O-methytransferase. 5 The production and diffusion into the bloodstream of metanephrines occur independently of the episodic secretion of catecholamines. Metanephrines are also produced in excess by sympathetic paragangliomas, but paragangliomas arising from the parasympathetic nervous system do not typically produce catecholamines. 6 Recent publications and guidelines have suggested that fasted, supine sampling (after 30 min supine rest) for plasma metanephrines should be regarded as mandatory due to the apparent improvement in diagnostic performance.4,7 It has also been suggested that where supine sampling is not practical and seated sampling is used, lower reference ranges based on a supine reference population should be used rather than seated reference ranges.4,7 This recommendation is based on data suggesting that diagnostic sensitivity is significantly higher when supine reference ranges are applied under seated sampling conditions rather than seated ranges.7,8 As phaeochromocytoma is potentially a life-threatening condition (due to the associated risk of adrenergic crisis), screening tests with high diagnostic sensitivity and high negative predictive value are required.
These recommendations have led to debate on the issue of appropriate sampling conditions and reference ranges.9–12 Some studies have suggested that seated sampling provides adequate diagnostic performance, in particular providing a high level of diagnostic sensitivity.13,14 A study carried out in our own centre when our liquid chromatography-tandem mass spectrometry (LC-MS/MS) method was originally established, found that plasma metanephrine measurements from samples taken during seated sampling and interpreted using seated reference ranges provided a diagnostic sensitivity of 100% and specificity of 96%. 14 Current routine practice in our centre is to collect samples for the measurement of plasma metanephrines with patients in a seated position. This practice is widespread due to the logistical difficulties of obtaining samples after 30 min in the supine position for all patients undergoing screening for phaeochromocytoma. We also use reference ranges based on a seated population when interpreting the results. 14 Our practice is therefore not concordant with recommendations that samples are taken in the supine position and interpreted using supine ranges. The aim of this study was to determine the diagnostic performance of our current approach of seated sampling with seated reference ranges and to determine the impact of applying published supine reference ranges to the interpretation of plasma metanephrines results obtained from seated patients.
Methods
A list of all patients who had adrenal histological analysis performed following adrenalectomy between January 2010 and October 2014 was gathered from our laboratory information system. The histological diagnosis for all patients was recorded and plasma metanephrines results generated prior to histological analysis were retrieved from the laboratory information system where available. All plasma metanephrines analyses were performed using a published LC-MS/MS method. 14 Patients with a histological diagnosis of extra-adrenal paraganglioma were also included in the search. This search was designed to provide a group of patients with a histological diagnosis of P/PGL and a group of patients with definitive exclusion of phaeochromocytoma. Approval for this audit was obtained from the Clinical Governance and Risk Department, Newcastle upon Tyne Hospitals NHS Foundation Trust (Caldicott Approval ID 4317).
Characteristics of the patient populations studied.
P/PGL: phaeochromocytoma/paraganglioma.
Fisher’s exact test.
Mann-Whitney test.
Diagnostic sensitivity and specificity were calculated using the histological diagnosis as the diagnostic standard. Plasma metanephrines results were considered positive if normetanephrine and/or metanephrine were above the upper limit of the reference range. Plasma metanephrines results were considered negative when both normetanephrine and metanephrine were within the reference range. Diagnostic sensitivity and specificity were calculated using both local seated reference ranges (120 to 1180 pmol/L for plasma normetanephrine and 80–510 pmol/L for plasma metanephrine) 14 and published age-related supine reference ranges. 15
Results
Diagnostic performance of seated sampling with seated ranges
Of the 40 patients with a diagnosis of P/PGL, 37 (93%) had a plasma normetanephrine or metanephrine above the upper limit of the seated reference range (Figure 1). The three patients with plasma metanephrines within the reference ranges were all diagnosed with ‘non-functioning’ extra-adrenal paraganglioma. Two of these three cases also had normal urine metanephrines concentrations (which were not measured in the third case). If these three cases of non-functioning paraganglioma are excluded, then 37 of 37 cases (100%) of P/PGL had raised plasma metanephrines. Of these 37 cases, 4 (11%) had a plasma normetanephrine or metanephrine (whichever was higher) between 1 and 2 times the upper limit of the reference range, 6 cases (16%) had values between 2 and 4 times the upper limit and 27 cases (73%) had values greater than 4 times the upper limit of the reference range. Of the 37 cases of P/PGL with elevated plasma metanephrines, 16 (43%) were associated with an elevation in normetanephrine only, 1 (3%) metanephrine only and 20 (54%) associated with elevations in both normetanephrine and metanephrine. Of the 73 patients with P/PGL excluded as the cause of an adrenal lesion, 7 (10%) had raised plasma metanephrines, all between 1 and 2 times the upper limit of the reference range. All but one of these 7 raised metanephrines was due to elevated normetanephrine only, with both normetanephrine and metanephrine elevated in the remaining case.
Plasma concentrations of normetanephrine or metanephrine (whichever was higher) expressed as multiples of the upper limit of the seated reference range (logarithmic scale) for patients with and without phaeochromocytoma or paraganglioma (PPGL). Horizontal lines highlight the upper limit of the reference range and twice the upper limit of the reference range.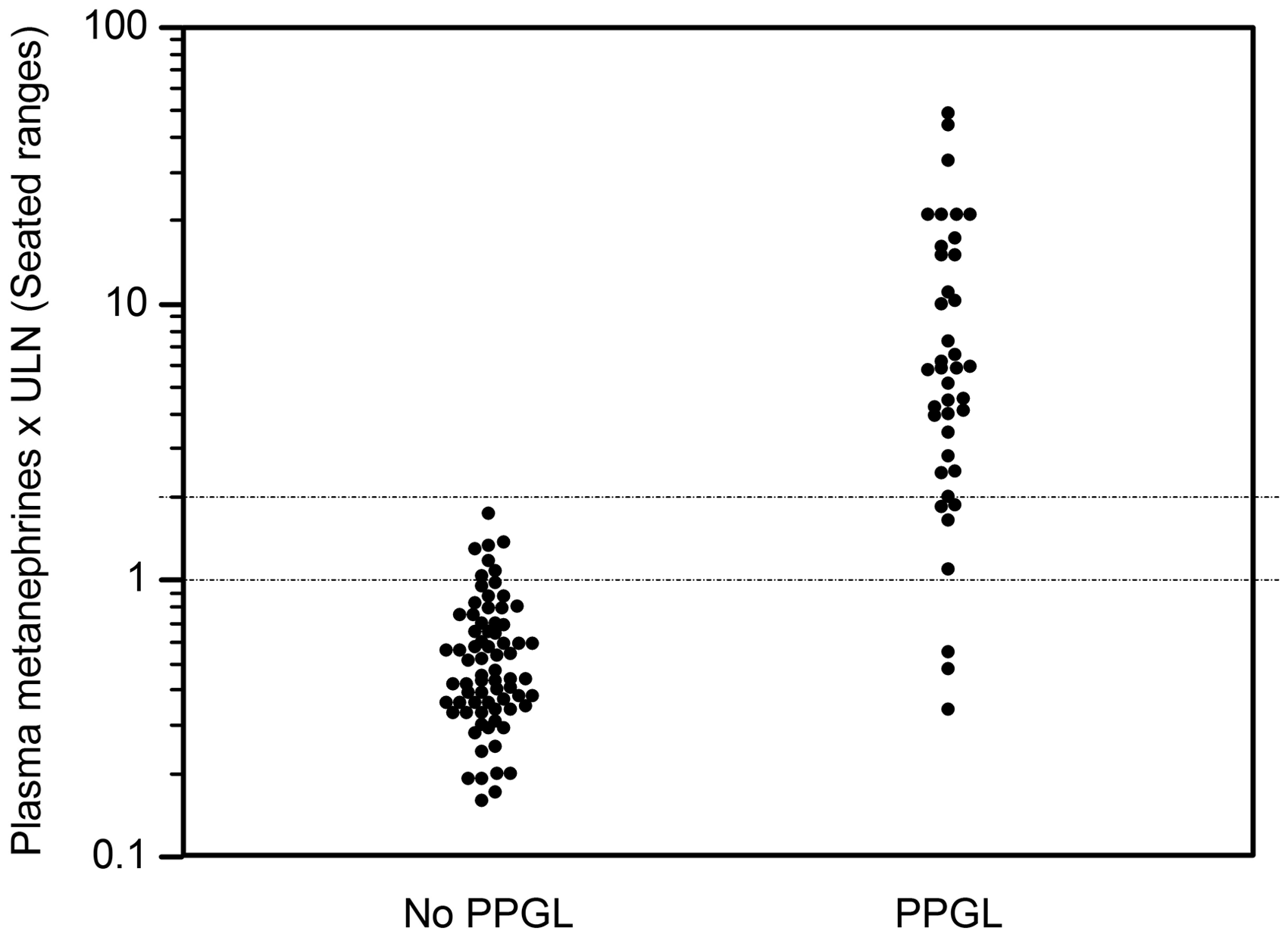
Impact of using supine reference ranges
In order to investigate the effect of using supine references ranges on the diagnostic performance of seated sampling in our centre, published supine ranges were also applied to the plasma metanephrines results for these two groups of patients. The supine ranges applied were age-related reference ranges published by Eisenhofer et al.
15
Of the 40 patients diagnosed with P/PGL, 37 (93%) had a plasma normetanephrine or metanephrine above the upper limit of the seated reference range (Figure 2). The three patients with results within the reference ranges were the same three cases of apparently non-functioning paraganglioma described above. Of the 37 cases with raised plasma metanephrines, 1 (3%) had normetanephrine or metanephrine between 1 and 2 times the upper limit of the reference range, 6 cases (16%) had values between 2 and 4 times the upper limit and 30 cases (81%) had values greater than 4 times the upper limit of the reference range. Of the 73 patients with P/PGL excluded as the cause of an adrenal lesion, 18 (25%) had raised plasma metanephrines, 17 of them between 1 and 2 times the upper limit of the reference range and 1 between 2 and 4 times the upper limit.
Plasma concentrations of normetanephrine or metanephrine (whichever was higher) expressed as multiples of the upper limit of published supine reference ranges (logarithmic scale) for patients with and without phaeochromocytoma or paraganglioma (PPGL). Horizontal lines highlight the upper limit of the reference range and twice the upper limit of the reference range.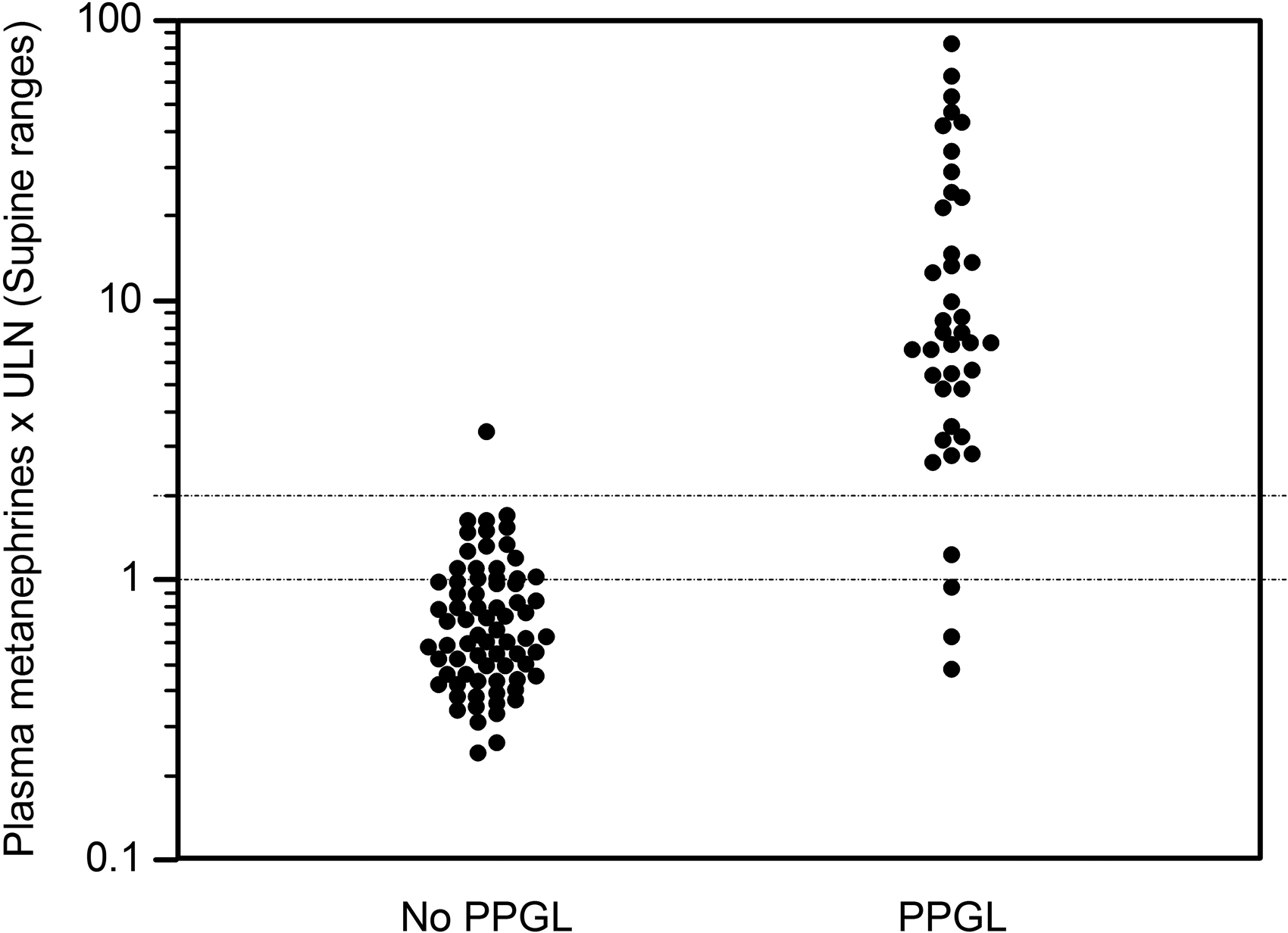
Diagnostic sensitivity was 93% for both seated and supine reference ranges (or 100% if three apparently non-functioning paragangliomas are excluded). Diagnostic specificity was 90% when seated reference ranges were applied and 75% when supine reference ranges were applied.
Discussion
Diagnostic performance of seated sampling with seated ranges
The aim of this study was to determine the diagnostic performance of plasma metanephrines with seated sampling and interpreted with seated reference ranges in our centre. The two groups of patients included in this study were a group of 40 patients diagnosed with P/PGL and a group of 73 patients with an alternative adrenal pathology as determined by histological analysis. Thirty-seven of the 40 patients in the P/PGL group had elevated plasma metanephrine, normetanephrine or both, where an elevated result was defined as being greater than the upper limit of the seated reference range. There were therefore three patients with apparently false negative plasma metanephrines results. However, these three patients diagnosed with paraganglioma had no history of symptoms of catecholamine excess. As well as having normal plasma metanephrines, two of these patients also had urine metanephrines performed, which were within the reference ranges in both cases (urine metanephrines analysis was not performed for the third patient). When lower published age-related supine reference ranges 15 were applied to these three cases, the plasma metanephrines remained within the reference ranges. As the plasma metanephrines were within the supine reference ranges for samples taken in the seated posture, it is likely that they would also have been within these reference ranges if the samples had been collected in the supine posture. It therefore appears that these are cases of non-functioning paraganglioma, which cannot be diagnosed through the measurement of metanephrines. If these three cases of apparently non-functioning paraganglioma are excluded from the study, the calculated diagnostic sensitivity of seated sampling with seated reference ranges is increased to 100%. The diagnostic specificity of plasma metanephrines using seated sampling and seated reference ranges was 90%. All false-positive results were in the range of 1 to 2 times the upper limit of the seated reference range. Therefore, applying a cut-off of 2 times, the upper limit of the reference range resulted in a diagnostic specificity of 100% for the population studied. However, in the range of 1 to 2 times the upper limit of the reference range there was overlap between patients with phaeochromocytoma or functional paraganglioma and patients without P/PGL. It is therefore not possible to exclude or diagnose P/PGL in patients with results in this range without further investigation.
Impact of using supine reference ranges
Applying published age-related supine reference ranges to this population did not provide an improvement in diagnostic sensitivity. The three cases of apparently non-functioning paraganglioma were associated with plasma metanephrines results within the reference range regardless of whether seated or supine ranges were used. Diagnostic specificity was significantly compromised when supine reference ranges were used. Specificity decreased significantly from 90 to 75% when the supine ranges were applied. Using supine reference ranges in practice would therefore result in a much higher false-positive rate, which could lead to unnecessary further investigation of patients without P/PGL. A higher false-positive rate could also lead to cases of P/PGL with mild elevations in plasma metanephrines being more likely to be incorrectly dismissed as false positives due to the larger number of patients with elevated plasma metanephrines results. P/PGL is a relatively rare disorder, so it is important to consider the pretest probability of P/PGL when interpreting positive results, particularly in the range of 1 to 2 times the upper limit of the reference range. For example, in a population with a P/PGL prevalence of 5% (e.g. in patients with an incidentally discovered adrenal mass16,17), a test with 90% specificity would provide a positive predictive value (PPV) of 33%, while a test with 75% specificity would provide a PPV of 17%. In a population with a P/PGL prevalence of 0.5% (e.g. in hypertensives from a general out-patients setting18,19) tests with 90% and 75% specificity would provide PPVs of 5% and 2%, respectively. However, plasma metanephrines results greater than two times the upper limit of the reference range would have a much higher positive predictive value.
Shortcomings of the study
This study has a number of significant shortcomings. Firstly, the population is relatively small with only 37 cases of functional P/PGL identified over four years. This means that the calculated diagnostic sensitivity of 100% (for functional P/PGL) could be an over-estimate. In this sample of 37 cases of P/PGL studied, there was one case where the plasma metanephrines were only slightly elevated with a normetanephrine concentration of 1.1 times the upper limit of the seated reference range (or 1.2 times the upper limit of the supine reference range). If a larger sample of patients was studied, it is more likely that cases of false-negative plasma metanephrines would be identified. The second shortcoming of the study is that the patients studied come from a highly selected population. By only including patients that have undergone adrenal surgery, cases with a low clinical suspicion for P/PGL and negative plasma metanephrines results have not been included. This group of patients could include some cases of undetected P/PGL. The selected nature of the study population also means that the calculated diagnostic specificity may provide an overly optimistic impression of the accuracy of a positive result in clinical practice (see previous paragraph for discussion of positive predictive values likely to be achieved in practice).
Conclusion
Despite the shortcomings of the design, this study provides evidence that the use of seated sampling and seated reference ranges provides a high degree of diagnostic sensitivity in screening for phaeochromocytoma and functional extra-adrenal paraganglioma in our centre. Introducing reference ranges determined using subjects in the supine position (as recommended in Endocrine Society guidelines 4 ) did not improve the diagnostic sensitivity of the test, but did have a significant detrimental effect on diagnostic specificity. Increasing the sample size included would improve the reliability of this study. As phaeochromocytoma and paraganglioma are rare disorders, a multicentre study may be required to achieve this. Given that routine practice in many UK centres is to carry out seated sampling for plasma metanephrines in most cases, a collaborative effort to create a larger data-set to inform future practice with regard to sampling posture and appropriate diagnostic thresholds would be beneficial.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Approval for this audit was obtained from the Clinical Governance and Risk Department, Newcastle upon Tyne Hospitals NHS Foundation Trust (Caldicott Approval ID 4317).
Guarantor
CB.
Contributorship
CB conceived the study, analysed data and wrote the first draft. BT, SB and DN were involved in conceiving the study and interpretation of data. SJ was involved in gathering patient information from the laboratory database. All authors reviewed and edited the manuscript and approved the final version of the manuscript.