
Abstract
Background
The presence of C3-epimer (C-3-epi-25-hydroxyvitamin D) in infant serum may complicate 25-hydroxyvitamin D (25(OH)D) measurement when using liquid chromatography tandem mass spectrometry assays that do not separately measure the epimer. We measured the concentration of C3-epi-25(OH)D in neonatal samples in Western Australian using umbilical cord blood samples and a liquid chromatography tandem mass spectrometry assay that separately quantifies 25(OH)D and C3-epi-25(OH)D.
Methods
A total of 120 anonymized cord blood samples were analysed using a liquid chromatography tandem mass spectrometry assay that utilizes two CSH fluoro-phenyl columns in series. Chromatography was performed on a Waters Acquity Ultra Performance Liquid system, and quantification was using a Waters Quattro Premier XE mass spectrometer.
Results
C3-epi-25(OH)D3 was detected in all umbilical cord blood samples (median 5.2 nmol/L, IQR 3.7–6.6 nmol/L) and contributed 6.6% (SD 2.6, 95% CI [6.1, 7.1]) of the total 25(OH)D concentration. Mean 25(OH)D3 measured in cord blood was 79.1 nmol/L (SD 22.7 nmol/L). A positive relationship (R2 = 0.35, P < 0.0005) between 25(OH)D3 levels and C3-epi-25(OH)D3 was noted in this cohort. No samples contained 25(OH)D2 or C3-epi-25(OH)D2.
Conclusion
C3-epi-25(OH)D3 is present in all neonatal samples but contributes <10% of the total 25(OH)D concentration which is unlikely to be clinically significant. Liquid chromatography tandem mass spectrometry assays that do not separately quantify C3-epi-25(OH)D3 from other vitamin D metabolites may potentially overestimate neonatal 25(OH)D levels, but diagnostic misclassification in neonates is unlikely.
Introduction
Vitamin D is a cholesterol-derived 9,10-seco-steroid that plays an important role in bone metabolism.1,2 Supplementation with vitamin D prevents and treats rickets in childhood and osteomalacia in adults. The recognition of this important role has been one of a number of significant success stories in modern medicine. 1 The measurement of total 25-hydroxyvitamin D (25(OH)D) within human serum provides useful clinical information about the vitamin D status of a patient. 1 However, accurate and consistent measurement of vitamin D and its metabolites in human plasma has proven difficult due to the hydrophobic nature and tight binding of 25(OH)D to vitamin D binding protein (DBP).3–5 Various immunoassays have been developed including enzyme immunoassays, commercial immunoassays and protein binding assays to address this issue.1,6,7 However, these automated assays fail to detect 25(OH)D2 and 25(OH)D3 equitably and led to concerns about their appropriate use and the interpretation of 25(OH)D results.8,9
Liquid chromatography tandem mass spectrometry (LC-MS/MS) is an accurate method for quantitating vitamin D when performed rigorously. However, LC-MS/MS does have limitations. 1 One specific limitation is the inability of early LC-MS/MS assays to separately discriminate between 25(OH)D and its C3-epimer, C-3-epi-25-hydroxyvitamin D (C3-epi-25(OH)D).5,6 The consistent lack of agreement between conventional chromatography as part of LC-MS/MS analysis and the DiaSorin RIA (radioimmunoassay) has been attributed to the presence of this C3-epimer. 10 C3-epi-25(OH)D may have negligible effects on calcium homeostasis, but in vitro data suggest this metabolite has an equivalent effect on parathyroid hormone suppression compared with 25(OH)D.6,11 These findings challenge the importance of specifically detecting 25(OH)D separately from its isomeric form.
C3-epi-25(OH)D was found to account for a significant proportion of the circulating 25(OH)D in infants under one year of age with the use of a 5-dinitrobenzoyl-phenylglycine column and LC-MS/MS methodology. 9 Consequently, interpretation of the concentration of total 25(OH)D in an infant population without separation of the C3-epimer could result in the under detection of vitamin D deficiency. 9 Absolute concentrations of C3-epi-25(OH)D are believed to be higher in the infant population on average with levels decreasing towards adult concentrations after one year of age. 6 According to other studies, 25(OH)D assays that do not separately quantify C3-epi-25(OH)D are likely to report falsely elevated concentrations for both adult and neonatal populations.6,9,12,13
We investigated the prevalence and concentration of C3-epi-25(OH)D in 120 neonatal cord blood samples collected in Western Australia using an LC-MS/MS method that quantified total 25(OH)D and C3-epimers separately. We hypothesized that C3-epi-25(OH)D would be present in a significant concentration in samples of cord blood. In addition, as previous studies had reported the proportion of total 25(OH)D relative to C3-epimer is related to age, 6 we also hypothesized that the percentage of total 25(OH)D present in the C3-epimeric form would be consistent throughout our sample population as they were all collected immediately postpartum.
Methods
Materials
25(OH)D3, 25(OH)D2 and C3-epi-25(OH)D3 were purchased from Sigma Aldridge St Louis, MO, USA, and deuterium-labelled 25-hydroxyvitamin D3 (d6-25(OH)D3) was obtained from Medical Isotopes Pelham, NH, USA. Astral Scientific, Caringbah, NSW, Australia supplied Chromsystems 6 Plus 1 Multilevel Calibrator set for 25(OH)D2 and 25(OH)D3. Tri-Level 25(OH)D Plus QC material was purchased from UTAK Laboratories, Valencia, CA, USA. All other chemicals were purchased at the highest commercially available grade.
Sample preparation
One hundred microliters of serum, calibrator or QC were added to a 1.5 mL polypropylene microcentrifuge tube with 12.5 μL of internal standard (hexa-deuterated 25(OH)D3), briefly mixed and allowed to incubate and 30 μL of sodium hydroxide (1 M) was gradually added to each sample gently to ensure the release of 25(OH)D from DBP but not denaturation of protein. The addition of 1 mL acetonitrile to each sample tube denatured proteins and enabled precipitation and removal of protein from the sample after centrifugation. 14 Samples were centrifuged at 15,000 rpm for 10 min at 4℃, and the supernatant transferred prior to sample concentration in a vacuum centrifuge. Dried samples were reconstituted with 100 μl 70:30 methanol: deionized water and measured in duplicate.
LC-MS/MS assay and analysis
A routine hospital laboratory assay for determining 25(OH)D in plasma or serum was used that utilized isotope dilution LC-MS/MS with electrospray ionization in positive mode. Two acidified ammonium acetate solvents in water and methanol were run as mobile phases with an increasing linear gradient of methanol to ensure separation of molecules during chromatography. The measurement of vitamin D metabolites and the C3-epimer was carried out on a Waters Acquity Ultra Performance Liquid Chromatography system and a Waters Quattro Premier XE mass spectrometer. The instrument parameters were set with a source temperature of 120℃. Capillary voltage and desolvation temperature were set to 2.5 kV and 350℃, respectively. Nitrogen was used as desolvation gas at 900 L/H and cone gas at 50 L/H. Singly charged transitions were monitored at mass/charge (m/z) 401.5 > 158.9 for quantification of 25(OH)D3 and C3-epi-25(OH)D3 (collision energy of 26 eV) and the water-loss transition m/z 413.5 > 395.4 as the qualifying ion (collision energy of 9 eV). Transitions, m/z 413.5 > 82.9 (collision energy of 20 eV) for quantification of 25(OH)D2 and the water-loss ion monitored as the qualifier ion at m/z 401.5 > 383.4 (collision energy 10 eV). Deuterated internal standards were monitored at m/z 407.5 > 158.9 and m/z 404.5 > 158.9 for d6-25(OH)D3 and d3-C3-epi-25(OH)D3, respectively, with collision energies of 26 eV. All ions were monitored continuously throughout the MS/MS run with an 80 ms dwell time. Chromatography was performed and baseline resolution achieved using two CSH fluoro-phenyl 1.7 μm, 2.1 × 100 mm columns in series at 50℃ fitted with a 0.2 μm Guard (Waters). Separation of the C3-epimer was based on the observation made by Van den Ouweland et al. 15 ; the fluorinated-bonded phase of the fluoro-phenyl column provides enhanced shape selectivity during chromatography. MassLynxs v4.1 was the operating system for the mass spectrometer and generated a chromatogram output for each sample. Data processing was then carried out by QuanLynx software calculating the peak concentration of each sample relative to a standard curve. A subsequent substudy of 30 samples (data not shown) analysed utilizing a tri-deuterium labelled d3-C3-epi-25(OH)D3 internal standard (IsoSciences, King of Prussia, PA, USA), which was not available at the time of initial analysis, verified that our LC-MSMS method accurately measured endogenous vitamin D metabolites including the C3-epimer with equivalent ionization efficiency.
Patient population
Samples of umbilical cord blood were collected into plain serum tubes immediately at the time of birth for routine clinical purposes from a population of 120 anonymized samples. Centrifuged samples were refrigerated for 7 days, and serum was separated and stored frozen at −20℃ until required for analysis. This study was reviewed by the Royal Perth Hospital Human Research Ethics Committee but deemed exempt from formal review under section 5.1.22 of the 2007 National Statement.
Results
Analytical characteristics
Optimal baseline resolution and adequate signal to noise ratio of the peaks for the 25(OH)D metabolites allowed successful identification of the individual analytes (Figure 1). Intra-assay coefficient of variations (CVs) for C3-epi-25(OH)D3 were 3.1–8.7% (25–175 nmol/L) and inter-assay CVs were 11.8–19.7 % (25–175 nmol/L). Intra-assay CVs for 25(OH)D3 were 2.1–3.7% (25–206 nmol/L) and inter-assay CVs were 4.7–7.1% (25–206 nmol/L). The limit of detection was 1 nmol/L for 25(OH)D. Absolute recovery was determined by triplicate LC-MS/MS analysis and was >90%.
Analyte quantification
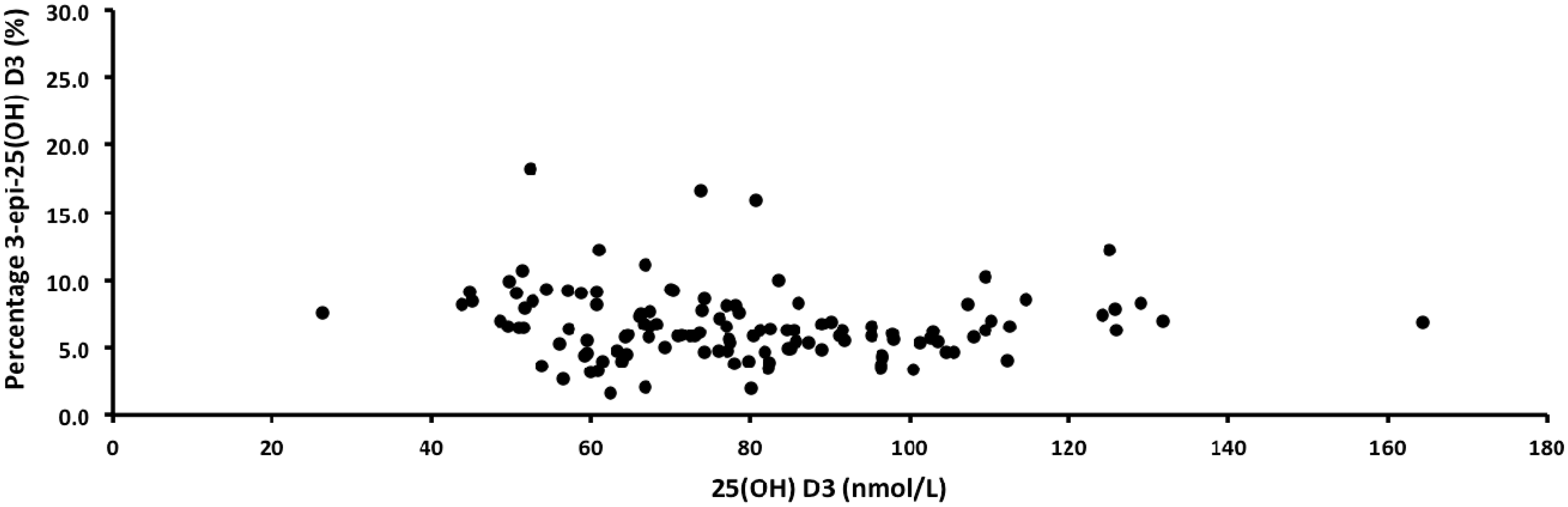
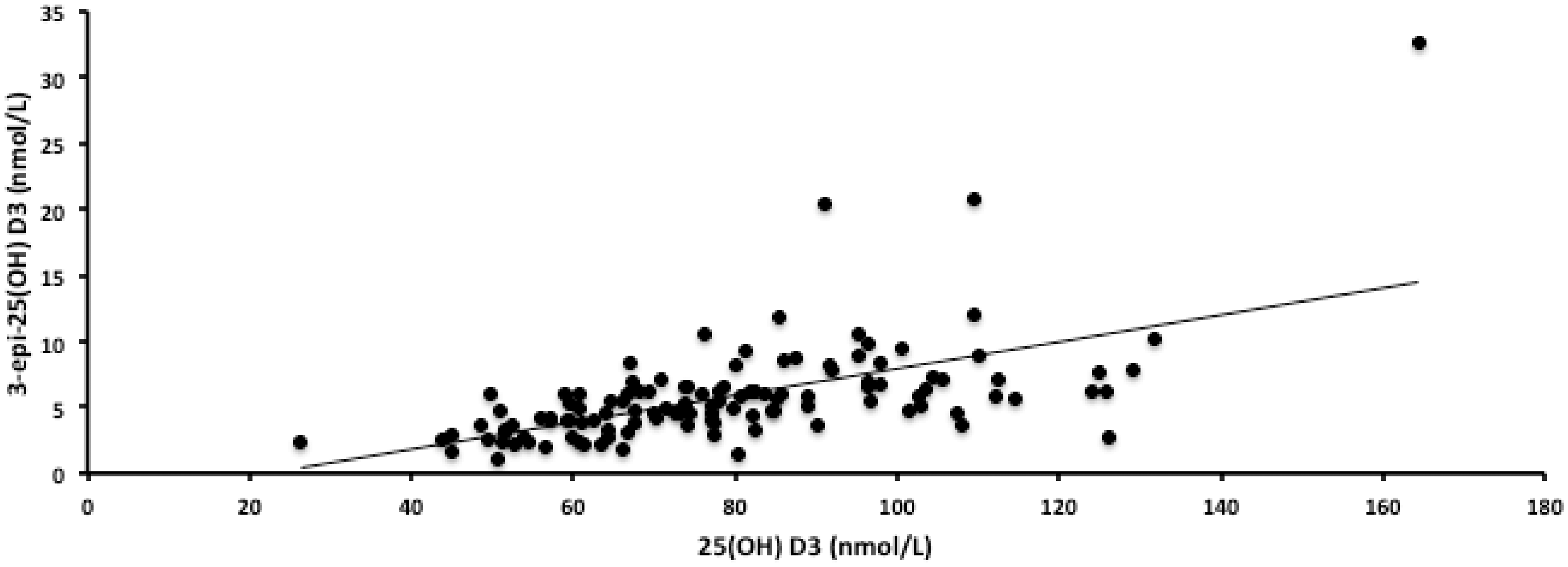
The mean concentration of 25(OH)D3 measured in the 120 samples of cord blood was 79.1 nmol/L (SD 22.7 nmol/L); 26.4 nmol/L was the lowest concentration in the sample population and 164.3 nmol/L the highest. Only seven samples in our cohort had concentrations of 25(OH)D3 less than 50 nmol/L; 39 samples had concentrations between 50 and 70 nmol/L and the remainder of samples were >70 nmol/L. The C3-epimer was detected in all cord blood samples (range 1.0–32.7 nmol/L); the mean concentration was 5.8 nmol/L, the median concentration measured was 5.2 nmol/L (IQR 3.7–6.6 nmol/L) and on average C3-epimer contributed 6.6% (SD 2.6%, 95%CI [6.1, 7.1]) of the total 25(OH)D concentration (sum of 25(OH)D3 and 3-epi-25(OH)D3), as shown in Figure 2. There was a moderate positive correlation (R2 = 0.35, y = 0.1018x − 2.2542, P < 0.0005) between the concentration of 25(OH)D3 and the concentration of C3-epi-25(OH)D (Figure 3); 25(OH)D2 was analysed in all cord blood samples but no trace of this analyte or its C3-epimer was detected consistent with the lack of ergocalciferol supplementation in our population.
Chromatogram demonstrating the baseline resolution and adequate signal to noise ratio of the peaks for 25(OH)D2, 25(OH)D3 and C3-epi-25(OH)D3. C3-epi-25(OH)D3 percentage contribution of total 25(OH)D (%) compared with the concentration of 25(OH)D3 (nmol/L) measured by LC-MS/MS in 120 samples of Western Australian cord blood. Concentration of C3-epi-25(OH)D3 (nmol/L) with the concentration of 25(OH)D3 (nmol/L) measured by LC-MS/MS in 120 samples of Western Australian cord blood (R2 = 0.35, y = 0.1018x − 2.2542, P < 0.0005).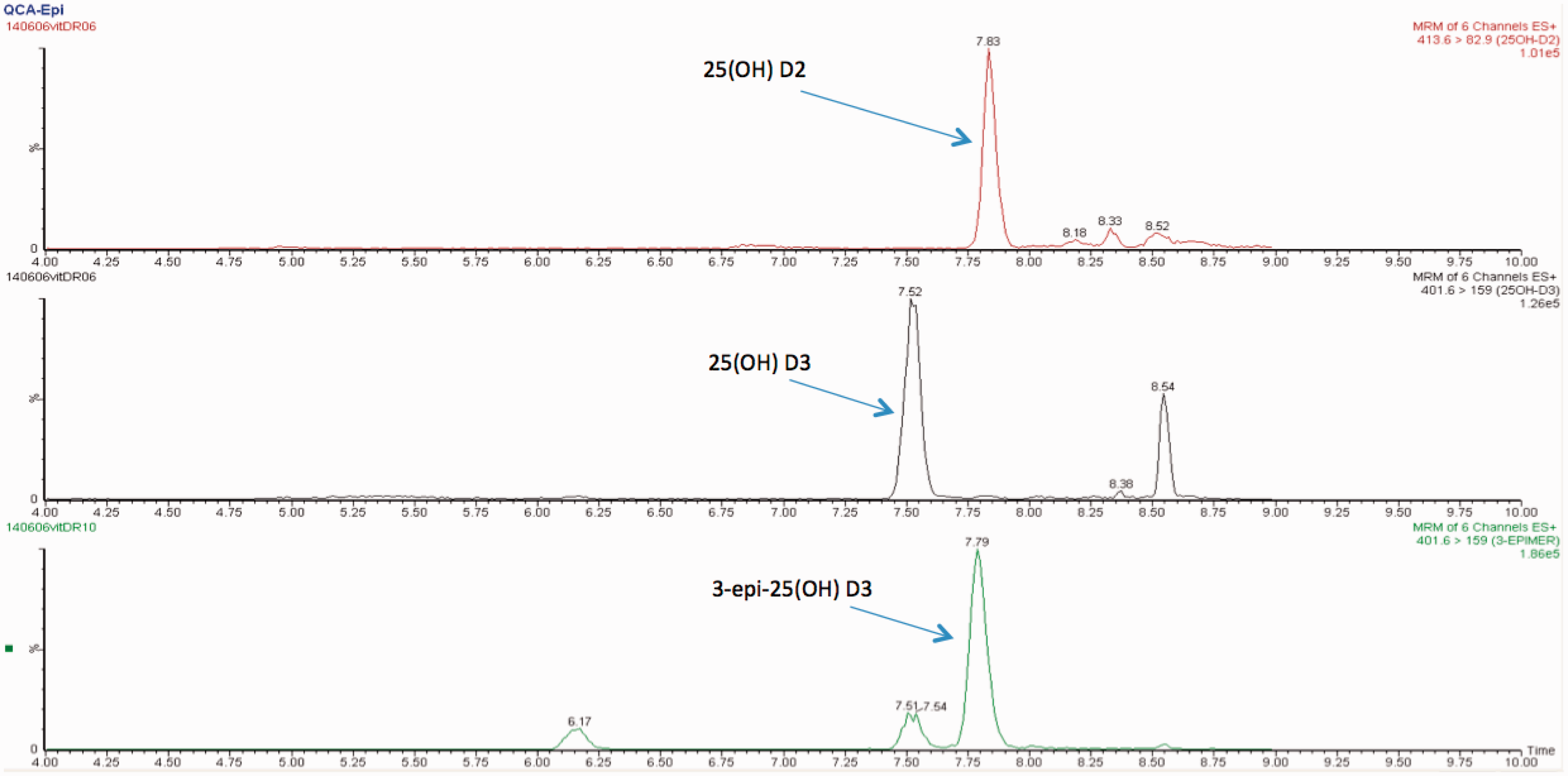
Comparison to the recent literature
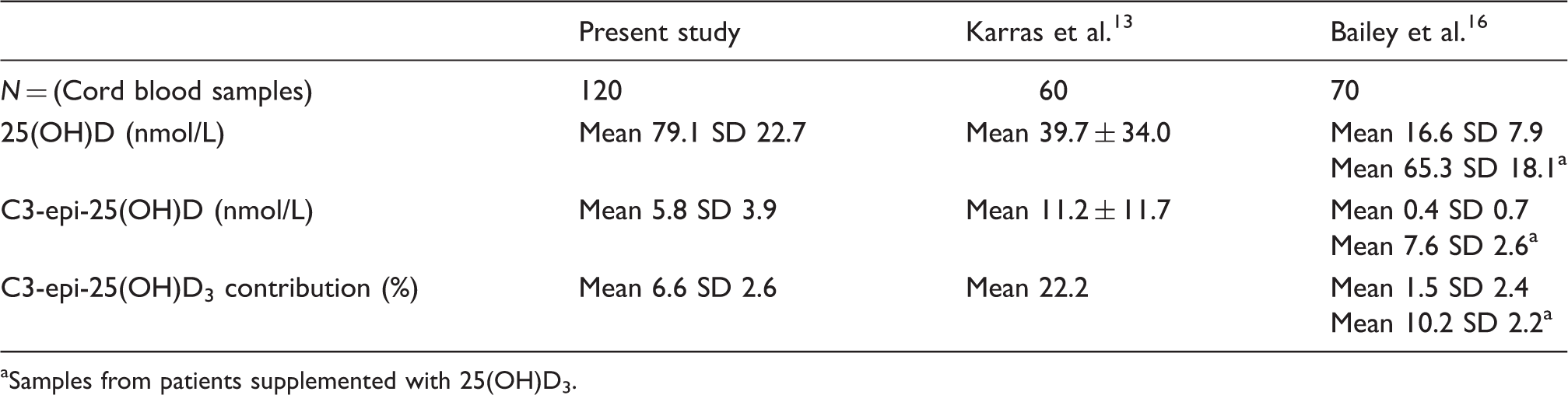
Samples from patients supplemented with 25(OH)D3.
Discussion
This study determined the concentration of C3-epi-25(OH)D3 in infant cord blood samples contributed a negligible amount to the total concentration of 25(OH)D. In fact, the average/mean level of C3-epi-25(OH)D3 detected in our study of 7% of the total 25(OH)D level is comparable to the magnitude of the inter-assay CV of our LC-MSMS assay. This level of C3-epi-25(OH)D3 is consequently unlikely, in the average patient, to lead to inaccurate assessment of vitamin D status.
The origin of the C3-epimer and its functional significance in neonatal vitamin D measurements by LC-MS/MS is not known. 16 One proposed hypothesis is that vitamin D metabolism by cytochrome P pathways may be immature in infants and the epimeric pathway may provide an alternative clearance pathway, hence increasing the prevalence of C3-epimer in this population. 6 However, the enzyme responsible for epimerization has not yet been identified and the physiological role of the C3-epimer has not been determined.
A recent study of maternal plus neonatal vitamin D status used paired umbilical cord neonatal blood and maternal serum samples. 13 A positive correlation between 25(OH)D concentration in mother and neonatal paired samples was reported with a weaker correlation between mother and neonatal paired levels of C3-epimer. 13 Recently, a positive correlation has been identified between C3-epi-25(OH)D and 25(OH)D levels within neonatal cord blood. 16 In this study, while C3-epi-25(OH)D was present in supplementation, this was not efficiently transferred transplacentally and C3-epimer concentrations were probably due to postnatal synthesis. 16 Bailey et al. 16 observed C3-epimer contribution of total 25(OH)D exceeding 9% in supplemented infants but only a minor percentage in non-supplemented cord blood which increased to approximately 10% in cord blood with supplementation. This is consistent with our findings and we suspect that the mothers of our study population were likely to have received vitamin D supplementation. In contrast, Karras et al. 13 observed a greater proportional contribution of the C3-epimer. However, this finding was in a smaller population who were predominantly vitamin D deficient and contrast with the sufficient 25(OH)D3 status in neonates in the present study.
This investigation demonstrated a positive correlation between the concentrations of 25(OH)D and its C3-epimer in cord blood, consistent with some but not all previous reports.13,16 The most striking difference between our results and those previously published is that our sample population included only 7 (5.8%) patients with 25(OH)D concentrations below 50 nmol/L. The majority of our sample population had 25(OH)D concentrations above this desirable limit; the results were less dispersed and this may explain our weaker correlation observed between C3-epi-25(OH)D3 and 25(OH)D3 concentrations.
Previous studies have demonstrated significantly higher C3-epimer relative concentration compared to total 25(OH)D in infants under 1 year of age 9 and it has been proposed that, although C3-epimer is present in vitamin D supplements, this is unlikely to cross the placenta. 16 While we have demonstrated the presence of the C3-epimer in cord blood the levels were found at concentrations lower than those demonstrated in young infants. Therefore, we believe this study provides evidence that supports Bailey et al. 16 model for post-natal C3-epimer synthesis.
It has been proposed that assays that do not separate the C3-epimer from other vitamin D metabolites could potentially result in over-estimations of the true vitamin D status in infants. 9 We believe that the presence of C3-epimer and the contribution to total 25(OH)D observed in this study does not warrant the separation of C3-epimer in assays used to determine the vitamin D status in neonatal cord blood routinely. Should future research identify the functional or clinical significance of C3-epimer as a biomarker, separation in addition to quantification, may be important.
A major strength of this study was the use of a fluoro-phenyl column during chromatography that allowed reliable separation and quantification of the C3-epimer. Furthermore, our study is the largest sample population of cord blood investigated for the presence and quantification of C3-epimer using LC-MS/MS analysis in the literature. However, due to the anonymous nature of the sample collection, no clinical information about the neonate or mother was available, so the relationship between C3-epimer and maternal supplementation reported by Bailey et al. 16 could not be independently verified. Moreover, very few of our samples had deficient levels of 25(OH)D, a fact that requires consideration when extrapolating these findings to the general population.
Conclusion
Utilization of an LC-MS/MS assay that separately quantifies C3-epimer from other vitamin D metabolites demonstrates that the C3-epimer contributes approximately 7% of the total 25(OH)D present in a population of Western Australian cord blood samples. Our finding is consistent with the postnatal synthesis of C3-epimer and suggests that assays that do not separately quantify C3-epimers are unlikely to significantly overestimate 25(OH)D levels in the average neonatal sample.
Footnotes
Acknowledgements
DC would like to thank the laboratory and clinical staff at the Department of Clinical Biochemistry, Pathwest Royal Perth Hospital for their ongoing support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Ethical approval
Ethics approval was exempt from RPH Human Research Ethics Committee under the provision of the National Statement (2007). Specifically, this study met the criteria for research exemption from ethical review under section 5.1.22, as it was of negligible risk (5.1.22a) and involved only non-identifiable data (5.1.22b).
Guarantor
PG.
Contributorship
All authors were involved in the design of the research. DC and BC performed laboratory analysis, collated data and wrote the first draft of manuscript. DB provided cord blood samples. All authors reviewed, edited the manuscript, analysed the data and approved the final version of the manuscript.