
Abstract
Background
After adrenalectomy, urinary fractionated metanephrine concentrations are expected to be reduced. However, there are few studies suggesting cut-offs for adrenalectomy patients.
Methods
Urinary metanephrine and normetanephrine concentrations in adrenalectomy patients and two controls were compared and hormonal concentrations were evaluated via time intervals after surgery.
Results
The median urinary metanephrine level after unilateral adrenalectomy was lower than that of the non-pheochromocytoma controls but comparable to healthy controls. Urinary normetanephrine concentrations did not differ between adrenalectomy patients and non-pheochromocytoma controls, although both group had levels higher than those of healthy controls. The median urinary normetanephrine level in the immediate postoperative period was higher than in the later period.
Conclusions
Urinary metanephrine concentrations were lower after adrenalectomy, but urinary normetanephrine concentrations were not changed compared with the non-pheochromocytoma controls. However, urinary normetanephrine concentrations in the patient group were higher than levels in the heathy controls.
Introduction
Pheochromocytomas can be fatal due to cardiovascular deterioration. Clinical suspicion and biochemical testing are crucial for the detection of pheochromocytomas. However, studies suggesting reference intervals for adrenalectomy patients have been limited, and most institutions have used references derived from healthy subjects to assess for recurrences of pheochromocytoma.
Recently, Osinga et al 1 . suggested adjusted references in patients for pheochromocytoma based on the hypothesis that production of epinephrine will decrease after adrenalectomy; urine metanephrine (MN) was lower and urine normetanephrine (NM) was higher in adrenalectomy patients than in the healthy controls.
However, NM concentrations are affected by aging, comorbidities such as hypertension and stressful conditions. 2 As with previous literatures, we reported lower urinary NMs in healthy volunteers than in separate controls consisting of elderly hypertensive subjects.2–4 The study from Osinga et al. 1 used healthy controls without any cardiovascular disease, and hormonal concentrations were not assessed in the immediate postoperative period when higher NM concentrations are expected. 1
Our aim was to analyse the urinary fractionated metanephrine concentrations in subjects with adrenalectomy for pheochromocytoma compared with non-pheochromocytoma controls and healthy volunteers, according to time intervals after adrenalectomy.
Methods
Subjects
Subjects who underwent unilateral adrenalectomy for pheochromocytoma between 2004 and 2014 at our institution were enrolled. Patients with partial or incomplete adrenalectomy, extra-adrenal or recurrent pheochromocytoma and no postoperative biochemical tests were excluded (n = 42). A total of 82 patients were eligible for this study.
Controls consisted of patients who had been confirmed as not having pheochromocytoma after adrenal surgery or had no adrenal lesion upon adrenal imaging and had been followed up more than two years or healthy normotensive individuals, as previously described. 3
Laboratory tests
For patients, urinary fractionated metanephrine concentrations were determined at pre- and postoperative periods. For non-pheochromocytoma controls with adrenal surgery, hormone concentrations measured before adrenalectomy were used.
The 24-h urinary fractionated metanephrines were measured by an Agilent 1200 HPLC system with electrochemical detector (Agilent Technologies, Santa Clara, CA, USA) using commercially available HPLC kits (Bio-Rad Laboratories, Hercules, CA, USA). Our institution used diagnostic cut-offs of urinary metanephrines for pheochromocytomas determined in Korean non-pheochromocytoma controls. 3
Results
Comparison of urinary fractionated metanephrines in the adrenalectomy group and the control groups.
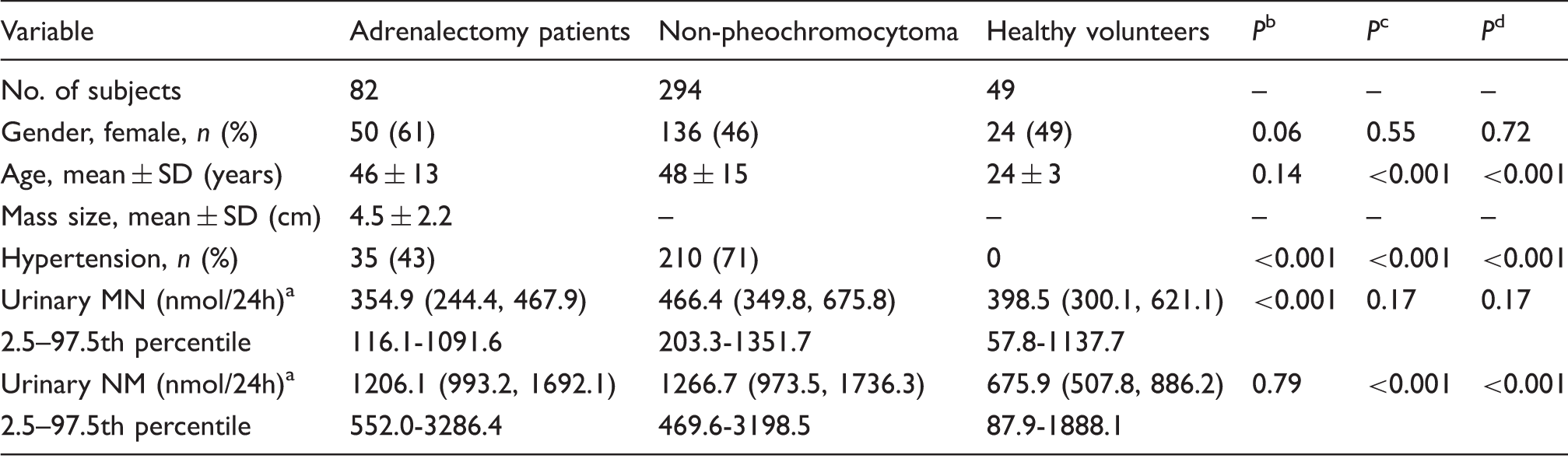
MN: metanephrine; NM: normetanephrine.
Variables with a normal distribution, such as age and mass size, were presented as the mean ± SD, and other nonparametric variables, urine MN and urine NM were presented as median and interquartile ranges. One-way ANOVA was used for comparison of parametric variables, and the Kruskall–Wallis test was used for non-parametric variables.
Adrenalectomy patients underwent unilateral adrenalectomy for pheochromocytoma and urine metanephrines were determined after adrenal surgery.
Non-pheochromocytoma group consisted of patients who had been confirmed as not having pheochromocytoma after adrenal surgery or had no adrenal lesion upon adrenal imaging and had been followed up more than two years, as described in a prior study. 3
Health volunteers were healthy normotensive individuals, as described in a prior study. 3
Reference intervals of urine metanephrines were described as ranges from 2.5 to 97.5 percentiles.
Data are presented as the median (interquartile ranges). The median value was used in each patient with multiple measurements of hormones.
Comparison between adrenalectomy patients and non-pheochromocytoma controls.
Comparison between adrenalectomy patients and healthy volunteers.
Comparison between non-pheochromocytoma controls and healthy volunteers.
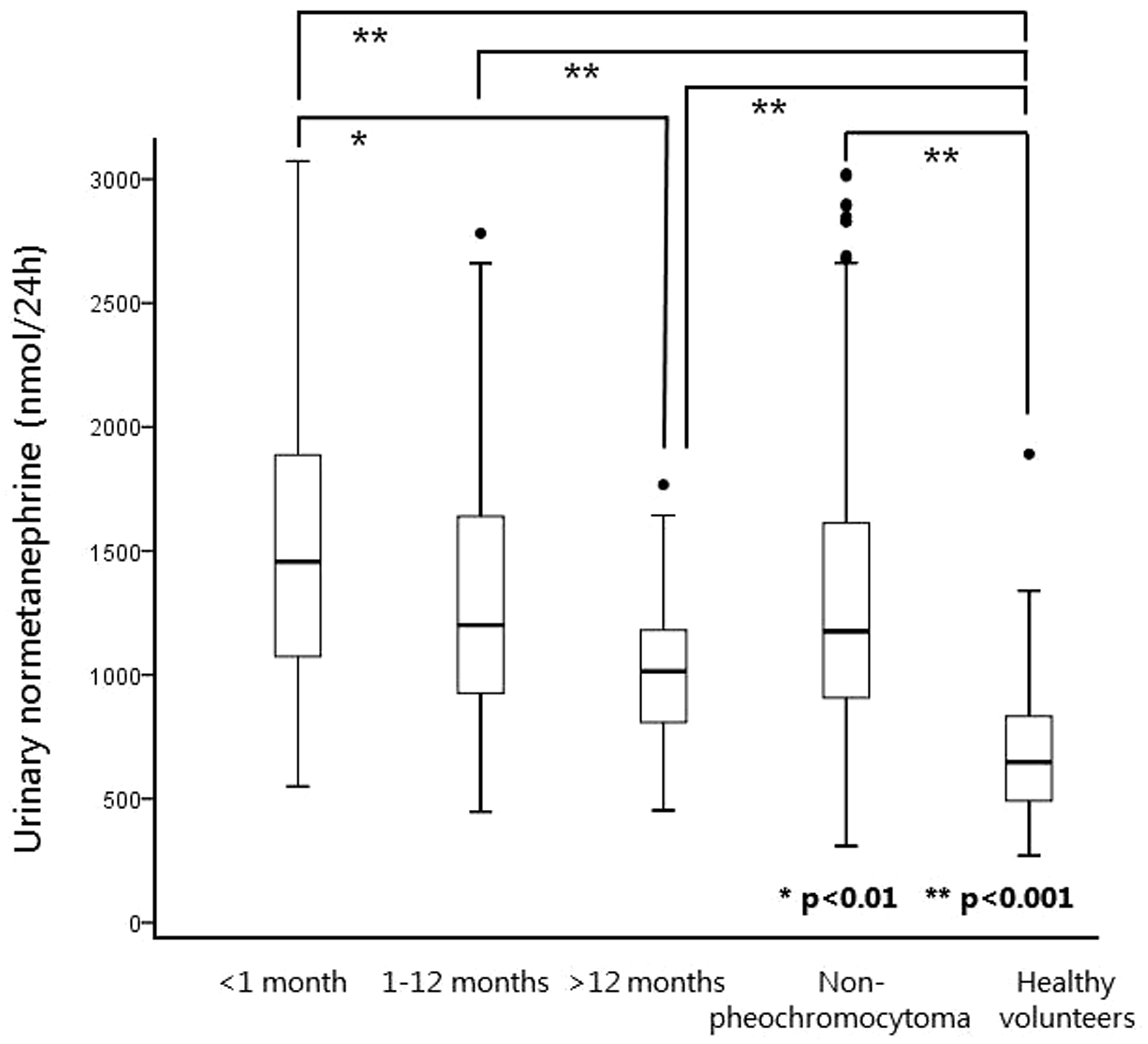
The urine MN concentrations in adrenalectomy patients did not differ in any postoperative period; these values were lower compared with the non-pheochromocytoma controls, but were similar to the healthy controls (Table 2, Figure 1). The urine NM concentrations of patients during each period were significantly higher than those of the healthy volunteers, although similar to those of the non-pheochromocytoma controls. The urine NM level in the immediate postoperative period (<1 month) was higher than that in the later period (>12 months) (Table 2, Figure 2).
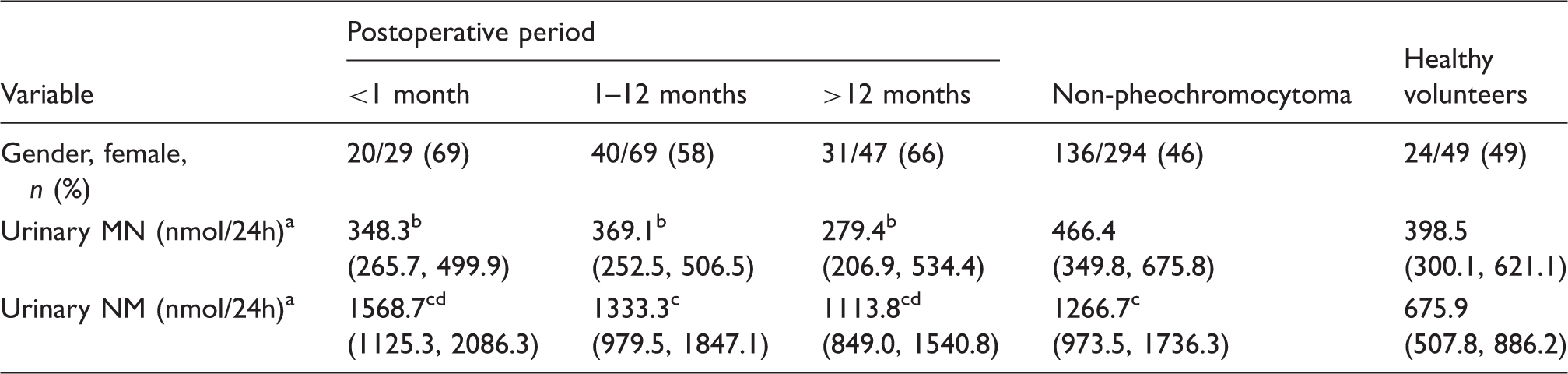
Postoperative urine metanephrine according to the time period. Postoperative urine normetanephrine according to the time period. Postoperative urinary fractionated metanephrines according to the time period. MN: metanephrine; NM: normetanephrine. The Kruskall–Wallis test was used for comparison of urine metanephrines. Adrenalectomy patients underwent unilateral adrenalectomy for pheochromocytoma and urine metanephrines were categorized by the postoperative period; <1 month, 1–12 months and >12 months. Non-pheochromocytoma group consisted of patients who had been confirmed as not having pheochromocytoma after adrenal surgery or had no adrenal lesion upon adrenal imaging and had been followed up more than two years, as described in a prior study.
3
Health volunteers were healthy normotensive individuals, as described in a prior study.
3
Proportions of women in each group by the postoperative period and in the two controls were not different. Data are presented as the median (interquartile ranges). The median value was used in each patient with multiple measurements of hormones. P < 0.001 (vs. non-pheochromocytoma controls). P < 0.001 (vs. healthy volunteers). P < 0.01 (postoperative period <1 month vs. >12 months).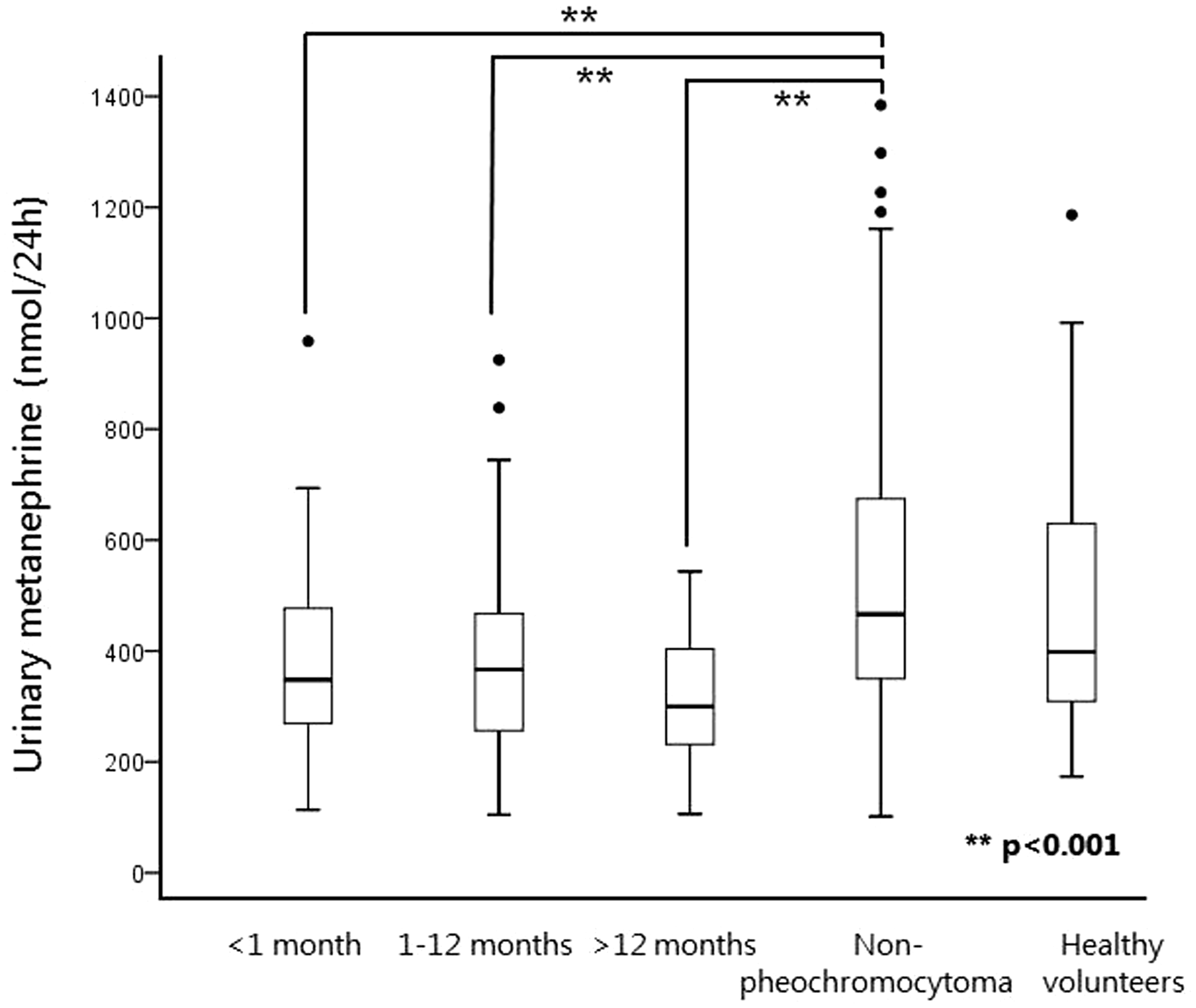
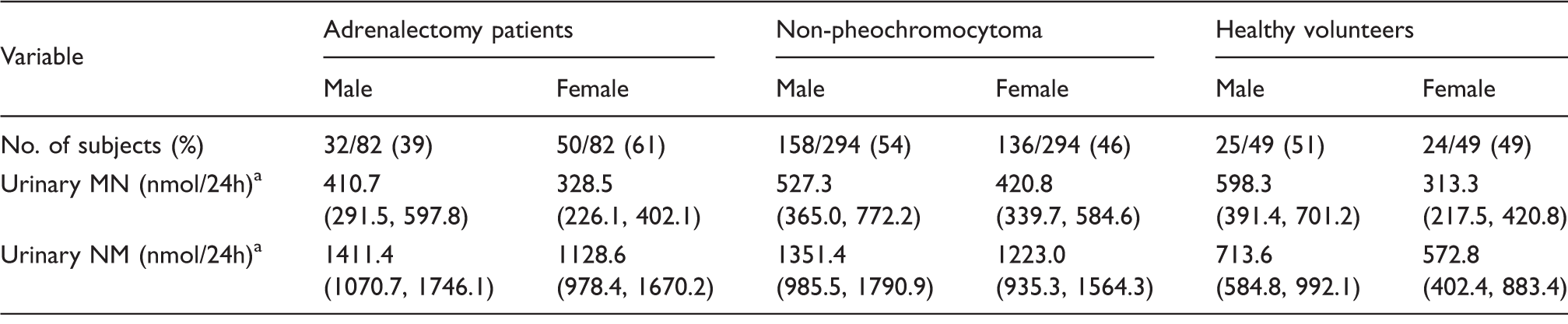
Postoperative urinary fractionated metanephrines by gender.
MN: metanephrine; NM: normetanephrine.
The Kruskall–Wallis test was used for comparison of urine metanephrines among the patient group and two controls, and the Mann Whitney U-test was utilized for comparison in both genders in each group.
Adrenalectomy patients underwent unilateral adrenalectomy for pheochromocytoma and urine metanephrines were determined after adrenal surgery.
Non-pheochromocytoma group consisted of patients who had been confirmed as not having pheochromocytoma after adrenal surgery or had no adrenal lesion upon adrenal imaging and had been followed-up more than two years, as described in a prior study. 3
Health volunteers were healthy normotensive individuals, as described in a prior study. 3
Data are presented as the median (interquartile ranges). The median value was used in each patient with multiple measurements of hormones.
The median urine MN and urine NM in women were significantly lower than in men in all groups (P < 0.01), except the urine NM concentrations, which were not statistically different between both sexes in healthy volunteers (P = 0.07).
Discussion
We identified that urine MN concentrations were lower in patients who underwent unilateral adrenalectomy for pheochromocytoma as compared with non-pheochromocytoma controls, whereas urine NM concentrations were similar between these two groups. During the postoperative period, urine MN concentrations were constant in adrenalectomy patients, whereas urine NM concentrations in the early postoperative period were higher than those in later periods.
Most free MNs are derived from adrenal chromaffin cells (∼90%), while NMs are mainly formed from sympathetic nerves (∼75%); however, only a small fraction of them are formed via adrenal medulla. 5 Considering the compensatory production of NM from extra-adrenal sympathetic nerves, lower reference intervals of MNs are expected in adrenalectomy patients, whereas the cut-offs for NMs do not need to be modified.
Contrary to our results, a study by Osinga et al. 1 suggested higher reference values of urine NM in adrenalectomy patients. They used 60 healthy volunteers as controls; the controls had no cardiovascular diseases, while 70% of patients had hypertension. 1 Aging and hypertension can affect urine NM concentrations; we observed a two-fold higher urine NM in non-pheochromocytoma controls than in healthy volunteers. If we used healthy volunteers as the sole control group, similar conclusions to the Osinga et al.’s might be drawn, indicating the importance of defining proper controls.
Urine NM concentrations were elevated in the early postoperative period than in the later period, which may be attributed to acute stress conditions via sympathetic nerve activation. However, urine NM concentrations were not different in patients and non-pheochromocytoma controls; thus, cut-offs for urine NM do not need to be adjusted.
Gender may affect urine metanephrines. We previously presented sex-adjusted diagnostic cut-offs of urine metanephrine concentrations, with higher cut-offs determined for men than for women, to optimize diagnostic accuracy. 3
We demonstrated hormonal trends of urine metanephrines after adrenalectomy compared with the controls, promoting the need for adjusted reference intervals. Adrenalectomy patients excreted lower concentrations of urine MN compared with the non-pheochromocytoma controls, whereas urine NM did not differ between them. However, reference ranges should be established in each laboratory, owing to different kits and assays for urine metanephrines.
Footnotes
Declaration conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Institutional Review Board of Samsung Medical Center approved this study (SMC 2015-06-044).
Guarantor
JHK.
Contributorship
All authors contributed to the preparation of the manuscript. YYC, YNK, JHK, BCJ and SYL. collected samples and obtained and/or analysed the data; YYC wrote the manuscript; JHK designed the study; JHK had full access to all data in the study and takes responsibility for the integrity of the data and the accuracy of the data analyses. All authors read and approved the final manuscript.