
Abstract
Background
Urine metanephrines are used to screen for phaeochromocytoma or paraganglioma (PPGL). Current reference intervals (RI) derived in healthy individuals are not age or sex-stratified, and lower than in hypertensive patients, leading to high false positive rates. This study aims to determine age and sex-stratified RI from a contingent screening population.
Methods
Patients with 24-h deconjugated urine metanephrines from 3/6/2010 to 27/8/2022 were included (2936 males, 5285 females), initially by liquid chromatography-electrochemical detection (LC-ECD) then liquid chromatography-tandem mass spectrometry (LC-MS/MS). Bhattacharya analysis was used after log transformation to determine age and sex-stratified RI for metanephrine excretion, normetanephrine excretion, metanephrine/creatinine and normetanephrine/creatinine ratios.
Results
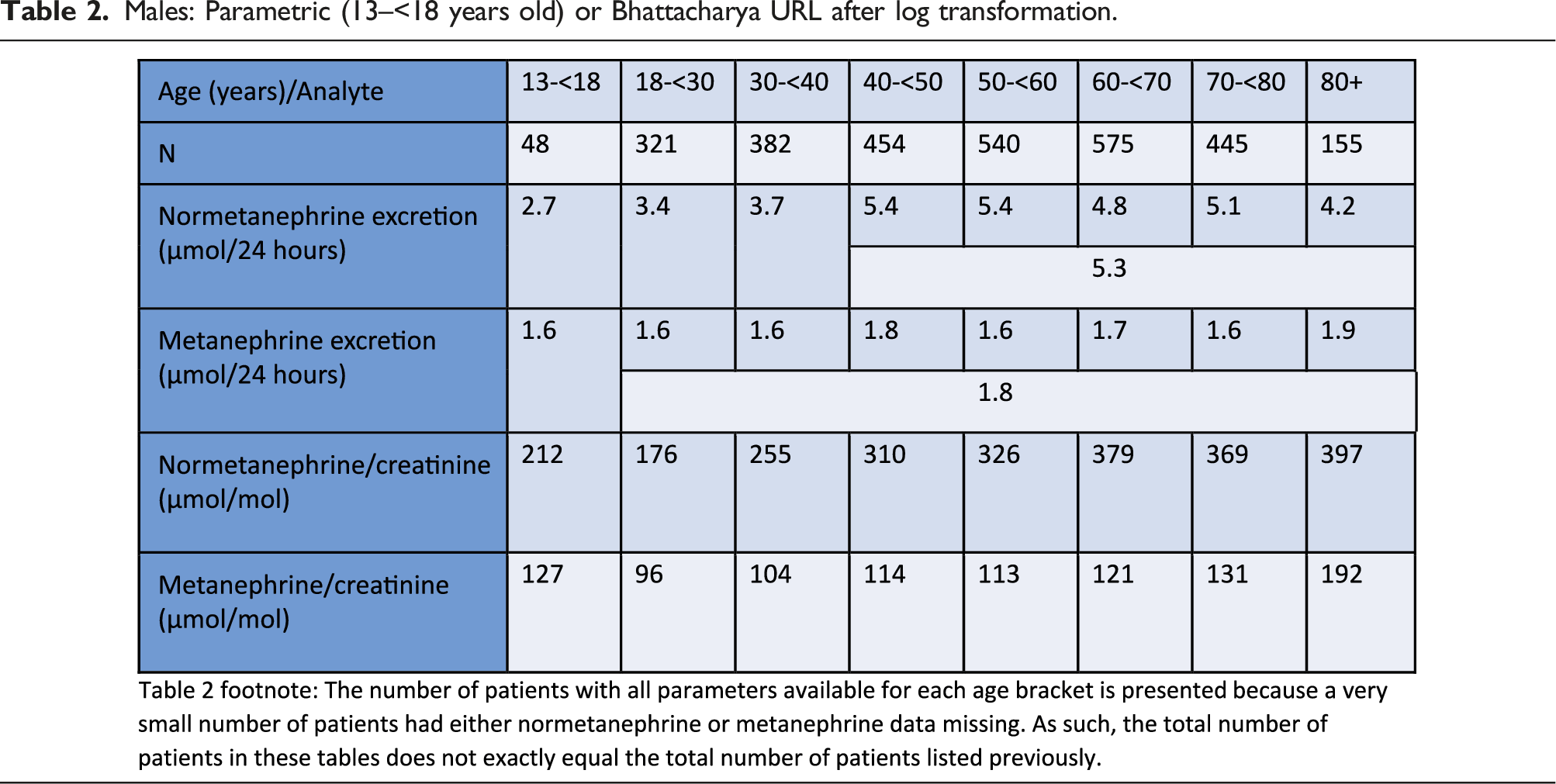
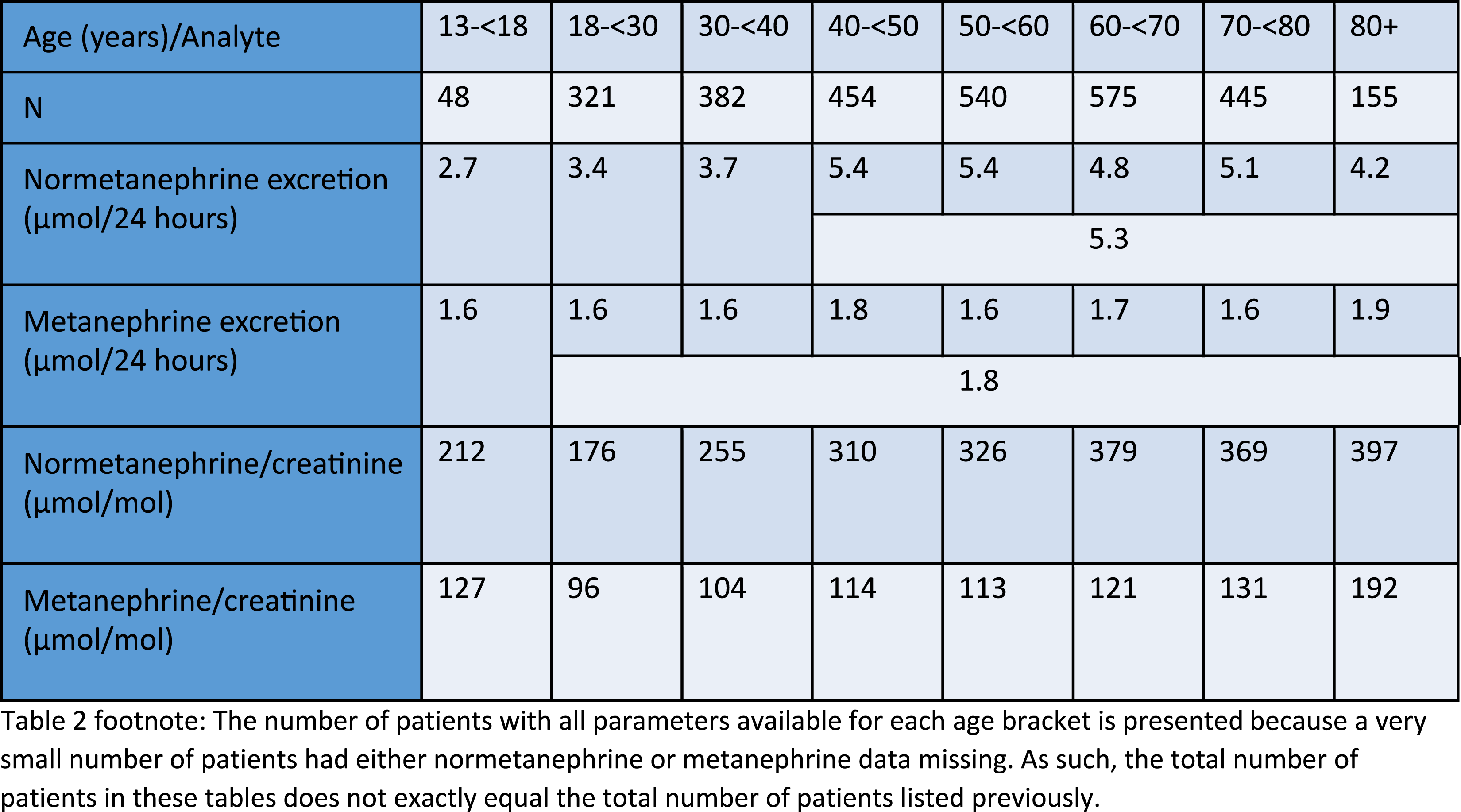
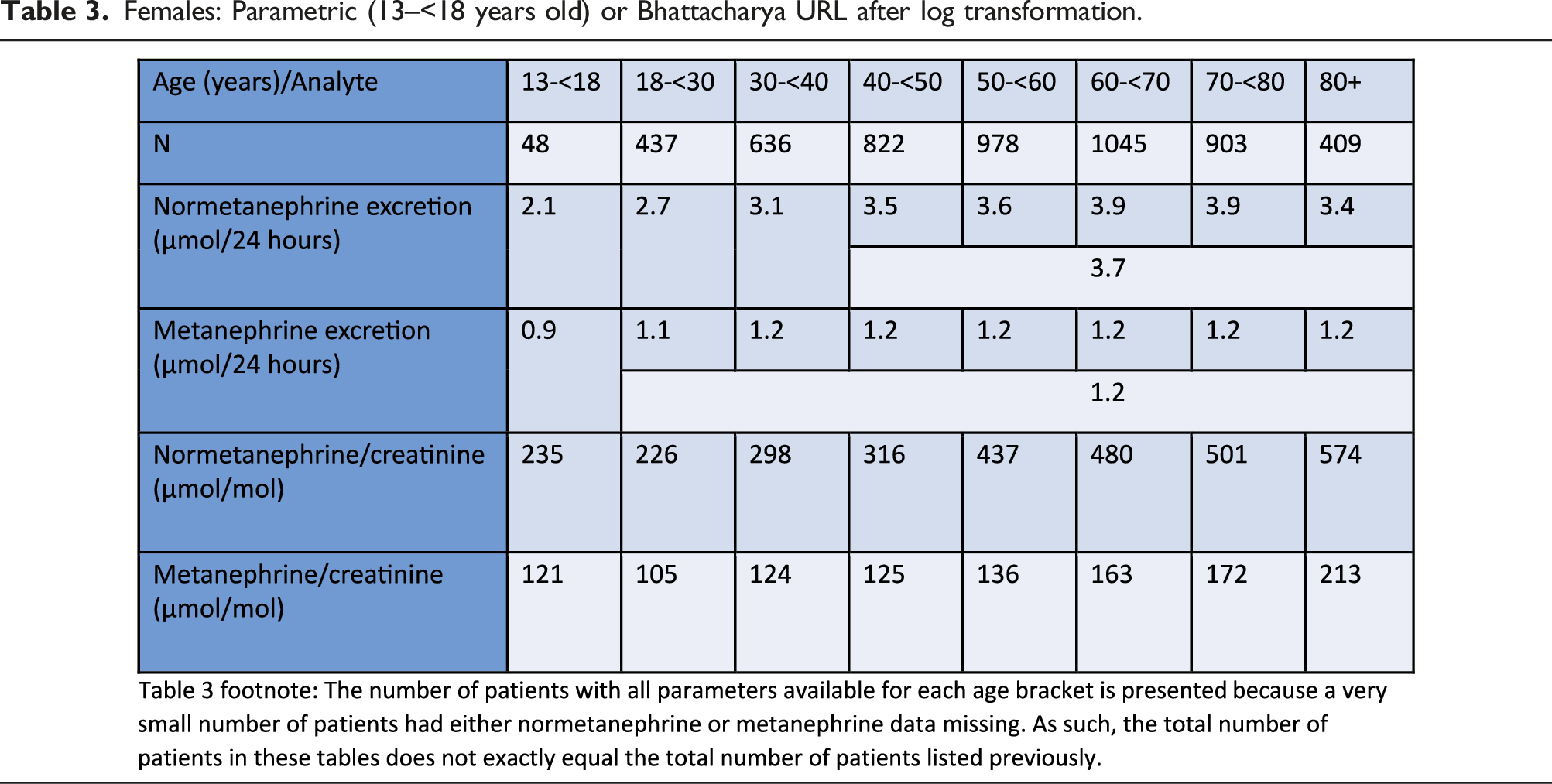
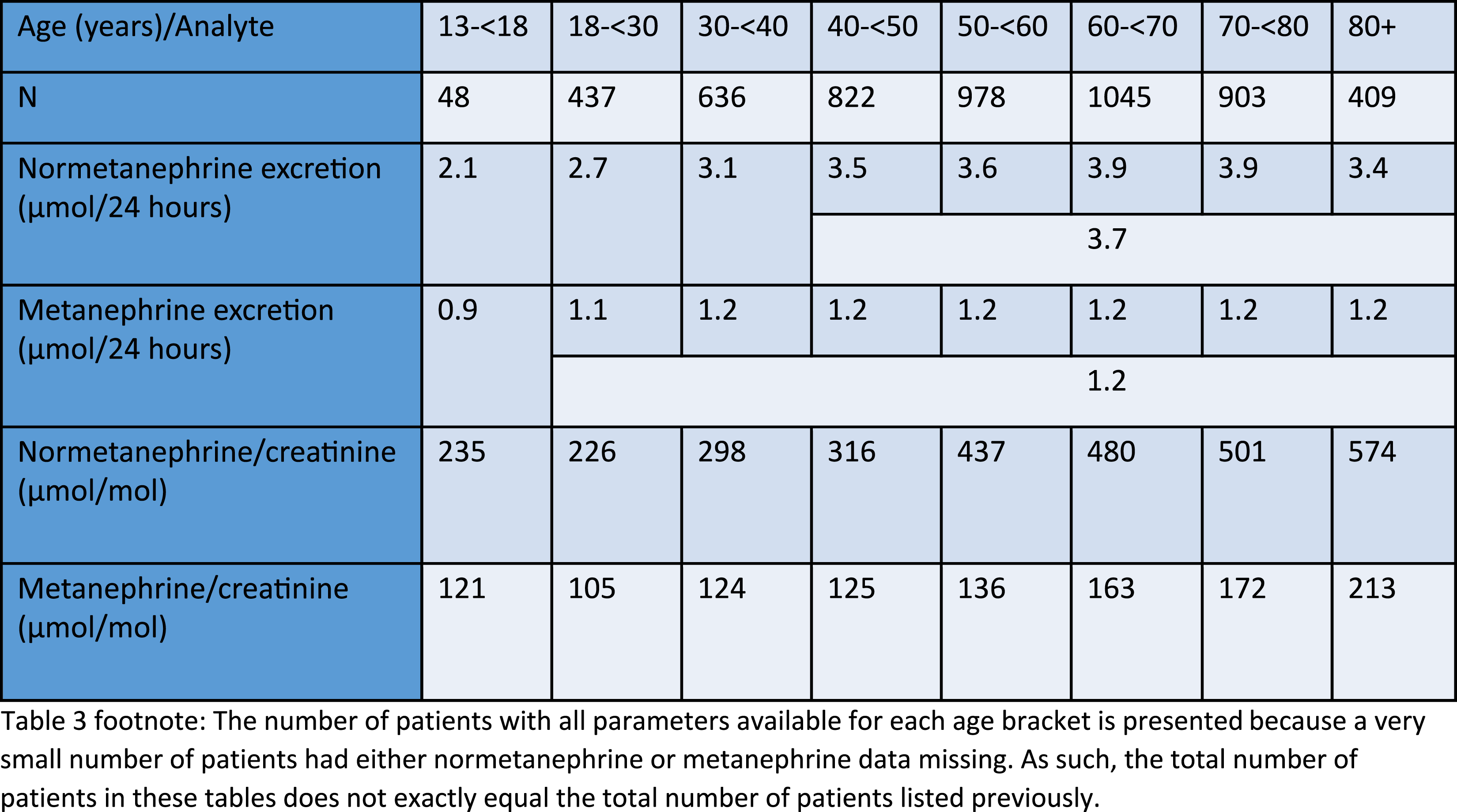
Normetanephrine excretion increases with age (RI: males: 18–<30 years: <3.4 µmol/24 h, 30–<40 years: <3.7 µmol/24 h, 40+ years: <5.3 µmol/24 h; females: 18–<30 years: <2.7 µmol/24 h, 30–<40 years: <3.1 µmol/24 h, 40+ years: <3.7 µmol/24 h), while metanephrine excretion was consistent across adulthood (RI: males: 18+ years: <1.8 µmol/24 h; females: 18+ years: <1.2 µmol/24 h). However, normetanephrine/creatinine and metanephrine/creatinine increase steadily with age after early adulthood, likely due to a decrease in muscle mass, with females having higher normetanephrine/creatinine and metanephrine/creatinine ratios.
Conclusions
Age and sex-stratified RI were derived for metanephrine excretion, normetanephrine excretion, metanephrine/creatinine and normetanephrine/creatinine ratios. This is expected to reduce false positives while flagging most PPGL.
Introduction
Urine metanephrines are used to screen for phaeochromocytoma or paraganglioma (PPGL), estimated to affect less than 0.3% of hypertensive patients. While hypertension is common in the community, PPGL is relatively rare, with a peak incidence in the third to fifth decade of life.1,2 However, there is clear evidence of differences in 24-h urine metanephrine and normetanephrine excretion by age and sex, as well as metanephrine/creatinine and normetanephrine/creatinine ratios.3–7 Current reference intervals (RI) in many laboratories were derived in younger, healthy individuals, are not age or sex-stratified, and lower than hypertensive patients, leading to high false positive rates. 3
RI for urine metanephrines proposed in the literature varies widely depending on methodology and patient cohort.3–6 Eisenhofer et al 2019 derived RI using direct RI techniques from healthy populations, with a higher male RI than female. 3 However, while direct RI techniques are generally considered gold standard, Clinical & Laboratory Standards Institute (CLSI) guidelines for determining reference intervals (C28-A3) recommend at least 120 healthy subjects in each partition for a non-parametric RI. 8 It is difficult and costly to get sufficient reference individuals in each partition for measurands which have clear changes by age and sex, and therefore direct RI studies often do not have enough participants to stratify further by age in a satisfactory manner. Furthermore, determining RI in truly healthy participants rather than hypertensive cohorts without PPGL results in higher false positive rates in hypertensive cohorts who have higher urine metanephrines.3,4,9
Kline et al 2020 derived RI for 24-h urine normetanephrine excretion from laboratory data, with age stratification, using a parametric RI approach. 4 The RI derived were higher than RI previously used by the laboratory and resulted in lower flagging, while still identifying all the patients with PPGL as the previous lower RI when the urine metanephrine RI was kept the same. However, while males have higher 24-h urine normetanephrine excretion, these RI were not stratified by sex. Furthermore, since 24-h urine normetanephrine excretion does not follow a Gaussian distribution, the use of mean +2 standard deviations to define the upper reference limit (URL) is likely to be an underestimate for the true URL.
Doyle and Frank 2021 found the URL for normetanephrine to vary substantially between Hoffmann, maximum likelihood estimation (MLE) and gamma mixture model, depending on the technique applied. 5 However, given that PPGL is rare, the lower estimates of URL based on some models are still implausibly low and would be expected to flag a high proportion of patients without PPGL.
Due to the wide variation between RI quoted in the literature and questions regarding the applicability of quoted RI in our local population, this study aimed to determine age and sex-stratified indirect RI from a contingent screening population using Bhattacharya analysis.
Methods
Patients with 24-h deconjugated urine metanephrines from 3/6/2010 to 27/8/2022 at Canterbury Health Laboratories, Christchurch, New Zealand, a tertiary referral hospital laboratory, were considered for inclusion (n = 10,866). Exclusion criteria were those with unknown date of birth (DOB) (n = 32), unknown urine volume or untimed specimens (n = 632), and any evidence of under-collection, over-collection, extremes of body mass and unspecified gender through a range of metrics (urine volume <500 mL in patient ≥18 years old (n = 137), collection duration <20 h (n = 49), collection duration >28 h (n = 9), no urine creatinine concentration (n = 9), unknown collection duration (n = 15), male with creatinine excretion >24.0 mmol/24 h (n = 230), female with creatinine excretion >17.0 mmol/24 h (n = 120), male ≥18 years old with creatinine excretion <7.0 mmol/24 h (n = 141), female ≥18 years old with creatinine excretion <4.0 mmol/24 h (n = 176), no gender specified (n = 4)). Urine creatinine excretion exclusion criteria for adults were based on RI from LabPlus, Auckland, New Zealand, which were slightly wider than our laboratory's RI. 10
Since patients with repeated testing were more likely to be abnormal, results after the initial request were excluded. Requests without National Health Identifier (NHI) were deleted if both sex and DOB matched another patient in the dataset (n = 11), and second and subsequent results for a given NHI were excluded (n = 1080). 2936 males and 5285 females remained after all exclusions.
Deconjugated urine metanephrines are stable in both acidified and unacidified state, frozen, refrigerated or ambient, for at least 4 weeks. 11 As such, both acidified and unacidified 24 h urine collections were accepted, and samples could be received in the laboratory either frozen, refrigerated or ambient. Samples are batched and analysed approximately once a week.
Normetanephrine and metanephrine analysis was performed after hydrolysis of sample and resin extraction by liquid chromatography-electrochemical detection (LC-ECD) at the start of the observed period, then liquid chromatography-tandem mass spectrometry (LC-MS/MS) from June 2013 onwards (i.e. the majority of the analysis period). The methods were comparable in the concentrations measured and the RI analysis pooled data from both methods together. Between run coefficient of variation (CV) for the LC-MS/MS assay for urine metanephrine concentration was 10.1% at 0.55 µmol/L and 8.2% at 3.00 µmol/L. For urine normetanephrine concentration, the between run CV was 10.2% at 1.80 µmol/L and 7.6% at 8.1 µmol/L. The assays were enrolled in the Royal College of Pathologists Australasia Quality Assurance Program (RCPAQAP) for urine metanephrines and a good agreement was achieved with other laboratories in this program over time.
Urine creatinine was measured by methods traceable to isotope dilution mass spectrometry, initially on Abbott ARCHITECT c16000 using a kinetic Jaffe method for most of the study, then Beckman Coulter AU5822 using an enzymatic creatininase and creatinase method from August 2021 onwards. Agreement between the two creatinine methods was good with minimal differences on method comparison, and both demonstrated good performance in the RCPAQAP general chemistry program.
Normetanephrine/creatinine and metanephrine/creatinine ratios were calculated automatically. Normetanephrine and metanephrine excretion was calculated by multiplying the concentration with volume of collection. Patients with a collection duration within 20–28 h but not exactly 24 h had normetanephrine or metanephrine excretion corrected to 24 h by multiplying excretion observed by 24 and dividing by collection duration in hours. Data was first inspected visually to determine the overall relationship between age and sex with the four calculated parameters. Plots of these parameters by age and sex were generated on R version 4.1.2.
For adults, Bhattacharya analysis was performed on Bellview version 1.2.6 after log transformation to determine age and sex-stratified URL based on expected 97.5th percentile of the ‘underlying distribution’ for metanephrine excretion, normetanephrine excretion, metanephrine/creatinine and normetanephrine/creatinine ratios. 12 The lower reference limits are not considered clinically important and are not presented. A pragmatic approach was undertaken to initially partition data into groups spanning 10 years of age, except for the 18–<30 year and 80+ year age groups. Where the URL of adjacent age groups for metanephrine and normetanephrine excretion was considered to be similar, these were subsequently reanalysed as a combined RI. These RI by Bhattacharya analysis were compared with the 97.5th percentile after excluding patients with results more than three times the current URL (current RI: normetanephrine excretion <2.9 µmol/24 h, metanephrine excretion <1.5 µmol/24 h, normetanephrine/creatinine ratio <260 µmol/mol, metanephrine/creatinine ratio <99 µmol/mol).
For the 13–<18 year age group, due to more limited data precluding the use of Bhattacharya analysis, parametric URL was generated after exclusion of results more than three times the current URL and log transformation (one male excluded). The limited data for 24-h urine metanephrines for patients under 13 years old (n = 19) precluded generation of RI for these patients.
p-values for differences between variables for males and females were calculated using a Wilcoxon rank sum test for continuous variables. A two-sided p-value <0.05 was considered statistically significant.
This study is considered to be a laboratory quality assurance activity, with results presented in a de-identified manner. As such, it was exempt from requiring ethics committee approval according to local guidelines.
Results
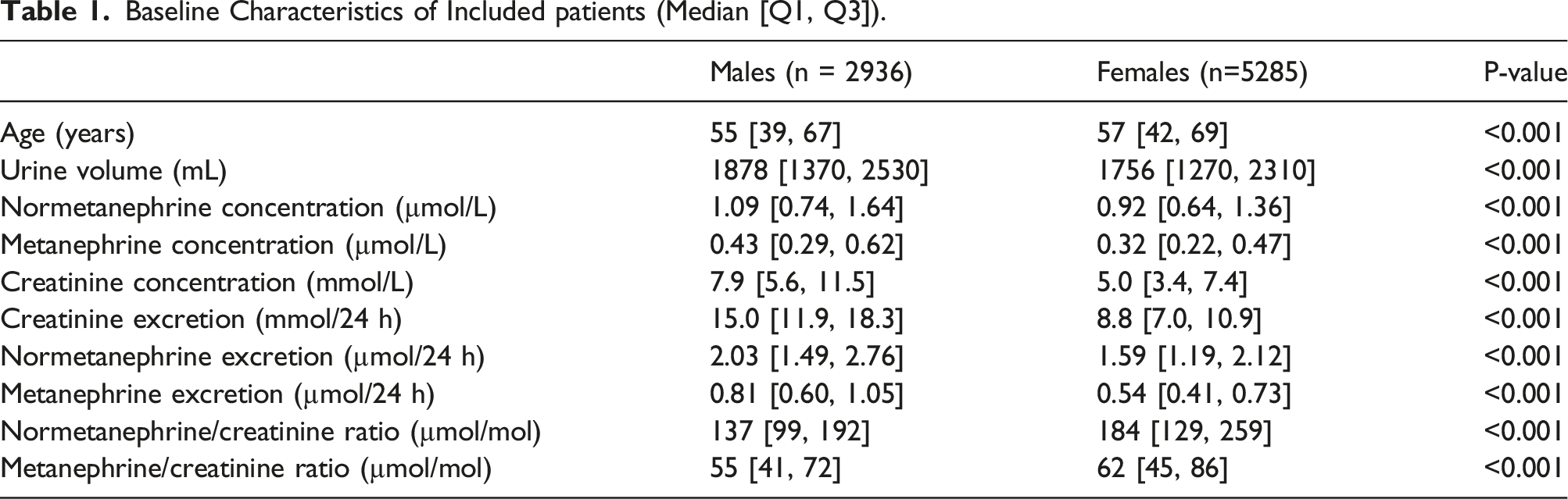
Baseline Characteristics of Included patients (Median [Q1, Q3]).
Males: Parametric (13–<18 years old) or Bhattacharya URL after log transformation.
Females: Parametric (13–<18 years old) or Bhattacharya URL after log transformation.
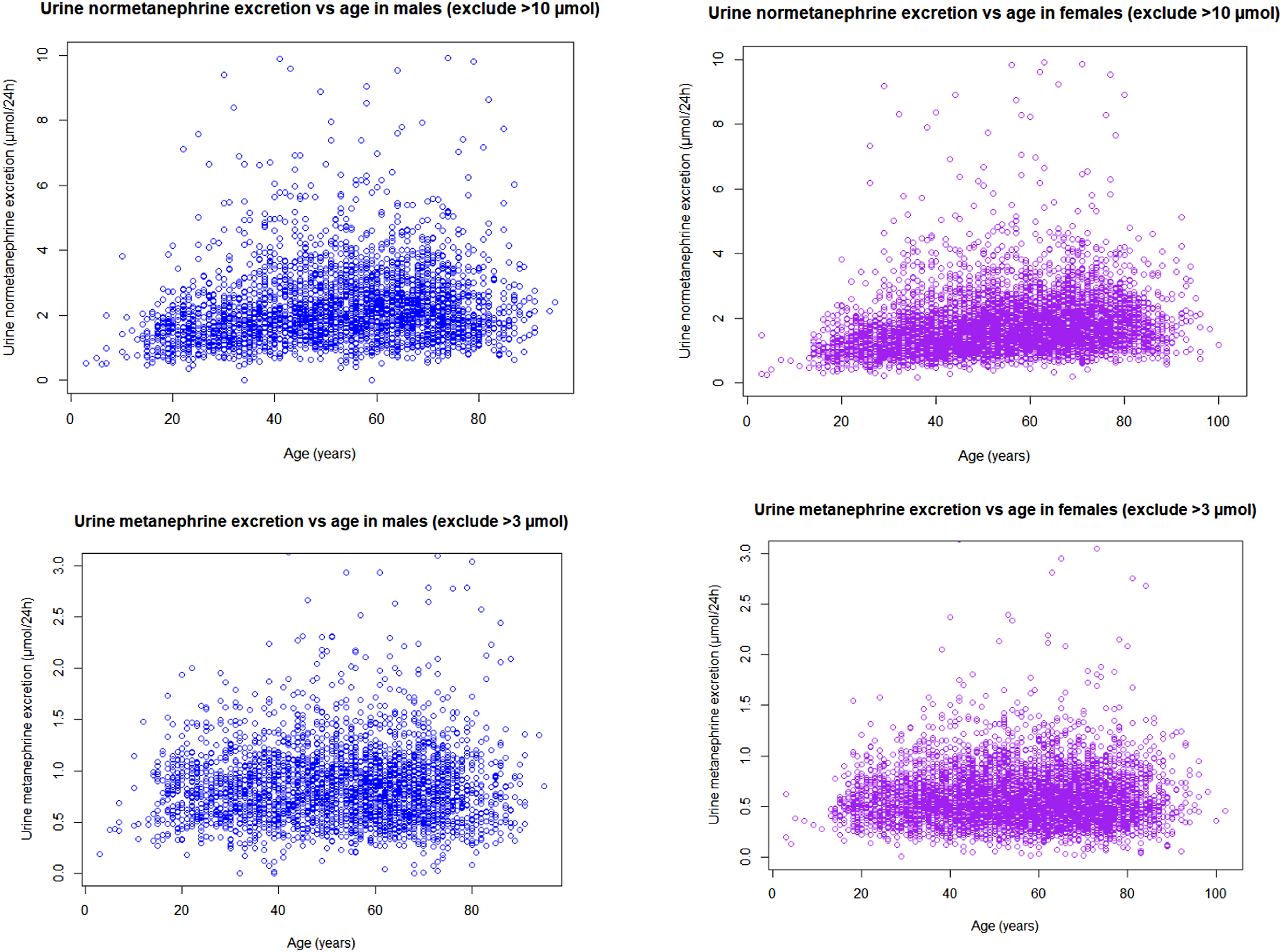
Urine normetanephrine and metanephrine 24-h excretion versus age in males and females.
However, normetanephrine/creatinine and metanephrine/creatinine increase steadily with age after early adulthood, with a more dramatic increase with age seen for normetanephrine/creatinine ratio, with females having higher normetanephrine/creatinine and metanephrine/creatinine ratios (Tables 2 and 3, Figures 2 and 3). Urine normetanephrine/creatinine and metanephrine/creatinine ratios versus age in males and females. Example Bhattacharya analysis histogram and log differences plot with fitted regression line for female 60–<70 years old ln(metanephrine/creatinine ratio).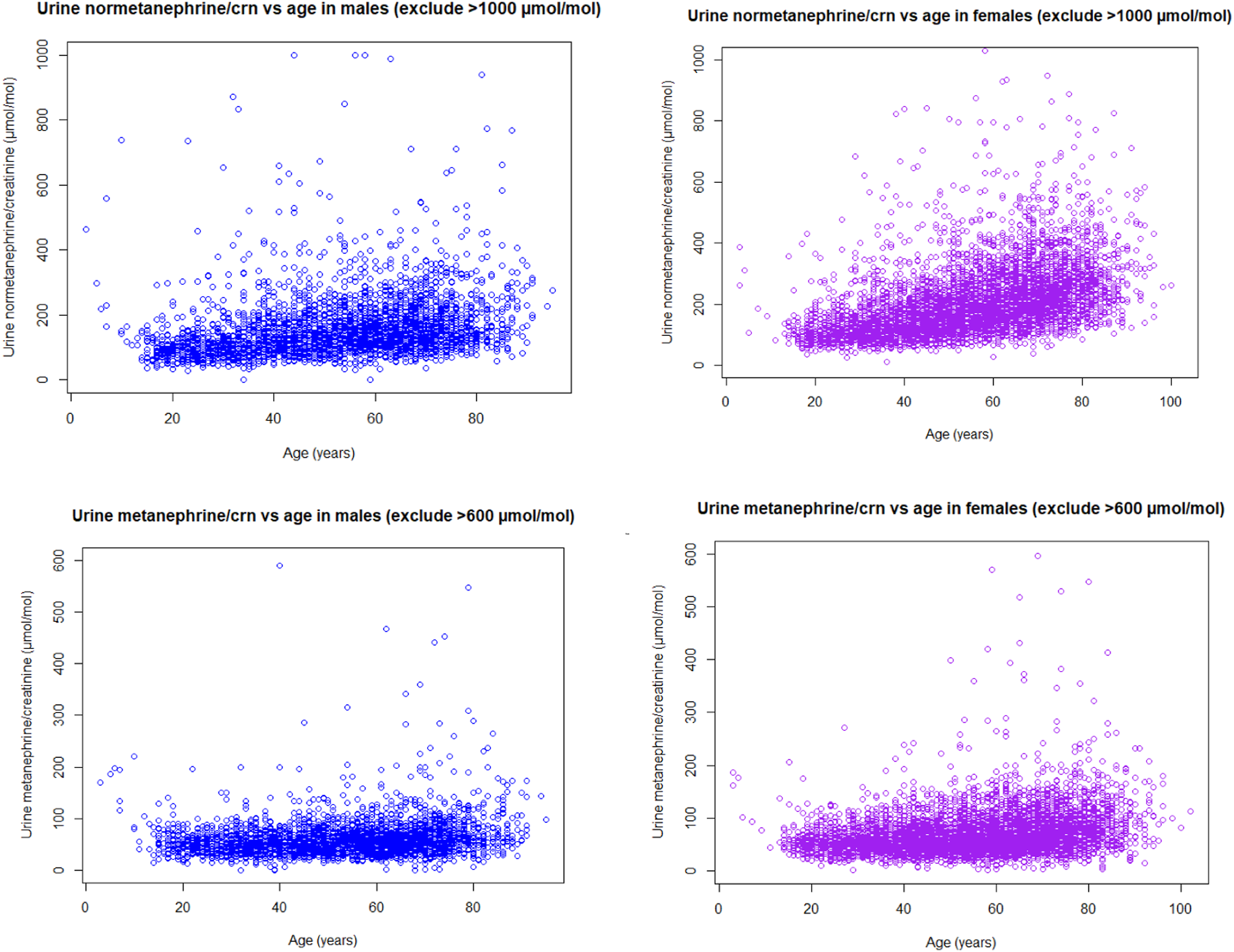
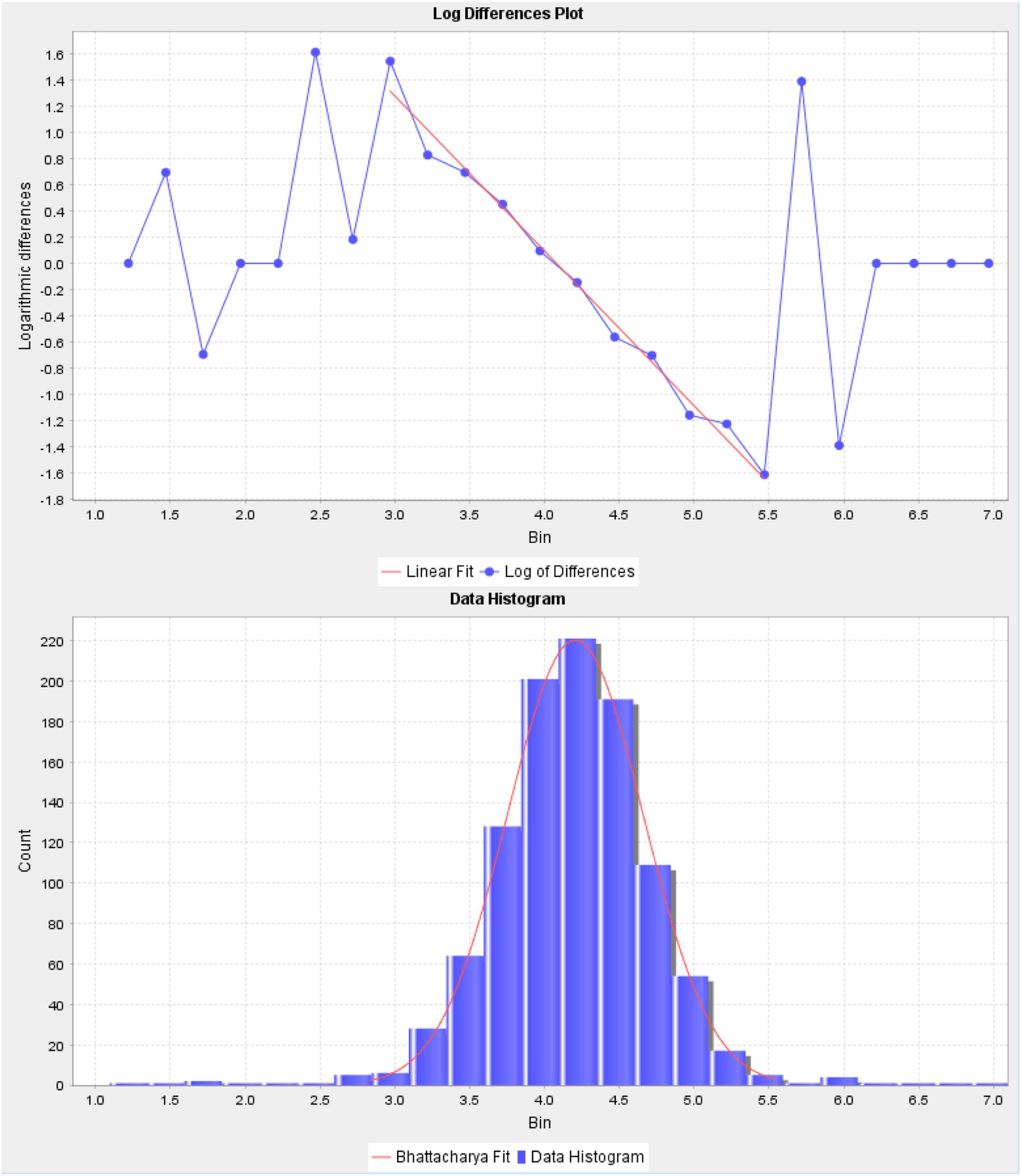
Log transformation was successful in bringing the calculated parameters into a normal distribution, especially for the age and sex brackets with the largest number of patients, as evidenced by a bell shaped curve on the data histogram and straight line encompassing most of the data on the log differences plots (Figure 3, Supplemental Figure 1). The URL obtained by Bhattacharya analysis was slightly lower in most age groups than those by a non-parametric approach after exclusion of results more than three times the current URL (data not shown).
Discussion
Age and sex-stratified RI were derived for metanephrine excretion, normetanephrine excretion, metanephrine/creatinine and normetanephrine/creatinine ratios. These are similar to RI from Lam et al 2017, 6 though slightly lower, likely due to use of Bhattacharya analysis in this study enabled by larger sample sizes instead of non-parametric methods. However, they vary more significantly from other studies with varying age representation and statistical methods.3–5
Consistent with other studies, males have higher 24-h urine metanephrine and normetanephrine excretion. The reason for this is unclear but for normetanephrine excretion is partially explained by a higher body surface area in males. 3 In addition, a negative relationship between plasma metanephrine and whole-body fat percentage has previously been described, explaining the observation of higher plasma metanephrine in males than females, which may explain the higher 24-h urine metanephrine in males than females.3,13
The observation of normetanephrine excretion peaking around middle age and tapering off whilst metanephrine excretion is relatively constant throughout adulthood is also consistent with other literature.4,6 This partially mirrors what is observed with plasma-free normetanephrine and metanephrine, but differs as plasma-free normetanephrine continues to rise into older ages instead of tapering off and decreasing. 3 The reasons for the slight difference in the relationship between urine normetanephrine and plasma-free normetanephrine with older age are unclear and outside the scope of this study.
In contrast to metanephrine and normetanephrine excretion, the metanephrine/creatinine and normetanephrine/creatinine ratios are higher in females than males in early adulthood and also later in life.6,14 This is likely due to females having lower muscle mass and therefore creatinine excretion than males, leading to higher creatinine adjusted ratios.
The rise in creatinine adjusted ratios with age is likely due to the combined effect of loss of muscle mass after early adulthood, along with changes in metanephrine and normetanephrine excretion as previously described. As metanephrine excretion varies little with age, the metanephrine/creatinine ratio increases slightly with age due to loss of muscle mass alone. On the other hand, the normetanephrine/creatinine ratio increases more dramatically with age, which represents effects of both increased normetanephrine excretion as well as decreased muscle mass, both acting to increase the normetanephrine/creatinine ratio with age.
Although there is some research to suggest that measurement of metanephrines on random urine samples using metanephrine/creatinine and normetanephrine/creatinine ratios has similar diagnostic discrimination to 24-h urine collections, 14 there were limited numbers of adult patients with random urine samples for urine metanephrines analysed by our laboratory. As such, reference intervals for these ratios from this study are based on 24-h urines. Random urines are likely to have a higher URL than 24-h urine collections for these ratios as random fluctuations throughout the day are not smoothed out. The derivation of age and sex-stratified URL of creatinine adjusted metanephrines for random urines using data from larger numbers of patients requires further study, and is highly recommended given the clear changes in these parameters according to age and sex. In the meantime, using the URL of these ratios derived from 24 h urines for random urine samples represents a precautionary approach.
Our generated RI are expected to reduce false positives while flagging most PPGL. Although a small number of patients with PPGL may be missed with higher URL than our currently used URL, given the low prevalence of PPGL, the number of PPGL missed is expected to be small compared to the decrease in false positives. For example, Eisenhofer et al found that using a sex-specific but not age-specific cut-off, changing the cut-off of urine deconjugated metanephrines from the 97.5th percentile to 99.5th percentile of the reference population decreased sensitivity marginally from 93.8% to 89.4%, but increased specificity from 85.4% to 95.3%. 3 We believe that using the expected 97.5th percentile of the contingent screening population, when adjusted by both age and sex, should counter the loss of sensitivity compared to using a higher age-independent cut-off in younger age groups, while decreasing false positives in older age groups.
Limitations
Although indirect RI are a pragmatic approach for determining RI from laboratory data, these are often wider than direct RI from preselected healthy populations. Whilst this is a theoretical limitation, it is recognized that hypertensive patients have higher urine metanephrines than non-hypertensive patients. As such, indirect RI from predominantly hypertensive populations based on laboratory data likely better reflect expected values for this population than non-hypertensive subjects.
Due to the large database used and large number of requests from external laboratories where medical records were not easily visible, it was not practical to examine medical records of all cases to eliminate patients with interfering medications or known PPGL from the analysis. Nevertheless, the use of the Bhattacharya technique should be successful in eliminating most patients with abnormally high results from the analysis, if they did not fit the underlying distribution. Furthermore, the low prevalence of PPGL in screened populations results in a lower portion of truly abnormal patients for the purposes of this test, which should result in generally valid RI derived from an indirect approach.
The limited number of patients aged 13–<18 years old precluded the use of Bhattacharya analysis in this age group. The best approach given the more limited dataset was to generate parametric URL after outlier exclusion of patients with results greater than three times the current URL, a rule of thumb to indicate high likelihood of PPGL and log transformation. Despite the limitations, the 24-h urine metanephrine and normetanephrine excretion URL are equal to or lower than adults in this study, while the metanephrine/creatinine and normetanephrine/creatinine URL largely correspond to those seen by Pussard et al in a healthy population. 7 As such, it is likely that the values presented are close to the true URL.
There was a change in methodology for urine metanephrines from LC-ECD to LC-MS/MS and urine creatinine from Abbott ARCHITECT kinetic Jaffe to Beckman Coulter enzymatic during the study period, which may have added some variability to the results. However, in both cases, the methods compared well with each other and had good performance on RCPAQAP. As such, this is unlikely to have a significant effect on the results of the study.
Conclusion
Age and sex-stratified URL for 24-h urine metanephrine excretion, normetanephrine excretion, metanephrine/creatinine ratio and normetanephrine/creatinine ratio were derived by Bhattacharya analysis after log transformation from a laboratory dataset for patients aged 18 years old and above. For patients aged 13–<18 years old, due to the smaller sample size, parametric URL was derived after log transformation. By considering differences by age and sex, URL derived in this study is expected to greatly improve specificity whilst missing a minimal number of PPGL compared to using common URL regardless of age and sex, or other RI proposed in the literature.
Supplemental Material
Supplemental Material - Reference intervals for deconjugated urine metanephrines by Bhattacharya analysis
Supplemental Material for Reference intervals for deconjugated urine metanephrines by Bhattacharya analysis by Bobby Li, Richard King, Christiaan Sies, Simon Thompson and Chris Florkowski in Annals of Clinical Biochemistry
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study is considered to be a laboratory quality assurance activity, with results presented in a de-identified manner. As such, it was exempt from requiring ethics committee approval according to local guidelines.
Guarantor
BL.
Contributorship
BL researched literature, undertook data analysis, and wrote the first draft of the manuscript. All authors provided feedback regarding data analysis, reviewed, edited, and approved the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.