
Abstract
Background
Zinc-induced copper deficiency is a condition whose diagnosis is often delayed allowing severe and usually irreversible neurology symptoms to develop. Plasma copper concentrations are usually low and plasma zinc concentrations high. The aim of this study was to measure the predictive value of this combination of results as a means of facilitating its early diagnosis.
Methods
Low plasma copper (≤6 µmol/L) and high plasma zinc results (>18 µmol/L) were retrieved from the laboratory database from 2000 to 2014. Medical records and laboratory notes of the corresponding 20 patients found were accessed to determine which were likely to have zinc-induced copper deficiency.
Results
Fifteen (75%) patients were diagnosed with zinc-induced copper deficiency which was symptomatic in 13. Of the five remaining patients, two were treated with zinc because of Wilson’s disease which was the cause of hypocupraemia, two were treated parenterally with zinc, and insufficient information was available in the final patient.
Conclusions
The combination of a low plasma copper and high plasma zinc is strongly predictive for the diagnosis of zinc-induced copper deficiency. There is the therefore an opportunity for the reporting biochemist to facilitate in its earlier diagnosis so enabling treatment to be implemented before the condition deteriorates.
Introduction
Copper deficiency is a rare but debilitating and potentially lethal diagnosis 1 that is frequently missed.2,3 The cause may be secondary to excessive ingestion of zinc usually in the form of supplements or zinc-containing dental fixatives.3–5 In zinc-induced copper deficiency (ZICD), metallothionein production in enterocytes is induced and zinc homeostasis is achieved by zinc binding to metallothionein which is subsequently lost when the cells are sloughed off into the gut lumen. However, metallothionein also avidly binds copper 6 potentially resulting in copper malabsorption and, if sustained for long enough, copper deficiency. The development of copper deficiency can occur over months or even years. Although mild cases may cause anaemia and neutropenia which respond well to stopping zinc ingestion, the diagnosis is often not made until the development of neurological symptoms that are usually irreversible and cause significant morbidity.2,3,7
Clinical laboratories increasingly measure trace elements by inductively coupled plasma mass spectrometry which allows them to be analysed simultaneously. For reasons of efficiency, laboratories may opt to measure both copper and zinc and report only the element(s) requested. This has been the approach taken in our laboratory with plasma zinc being reported only if an individual plasma copper request is low or conversely plasma copper being reported if a plasma zinc request is high. The finding of a low copper and high zinc concentration can alert the requesting clinician to the possibility of ZICD before it has been suspected clinically.3,8 The objective of this study was to determine the reliability of this technique in the diagnosis of ZICD.
Method
A search of our laboratory database was performed, covering January 2000 to March 2014, to retrieve plasma copper and zinc results from adult patients in whom both were measured. Of 8521 such patient samples referred to our laboratory from across Scotland, 252 (3.0%) had a plasma copper concentration of 6.0 µmol/L or less. This concentration was chosen as a cut-off since in our experience and review of the literature, symptoms of copper deficiency are not usually manifest above this concentration. 8 Of these low plasma copper results, 26 (0.3% of all patients) had a plasma zinc concentration over our upper reference interval of 18 µmol/L. Six of these patients (23%) had a single isolated plasma zinc concentration of over 18 µmol/L. These were excluded since a high plasma zinc is commonly caused by contamination, usually because plasma is separated into a container which has a zinc-containing O-ring in the lid 9 or because of delay in separation of blood. 10 Consequently, the remaining 20 patients included in the study had more than one high plasma zinc concentration indicating that the results were not artefactual. All 20 patients also had at least two low copper results confirming hypocupraemia.
Medical records of these 20 patients and informal notes made in the laboratory at the time of sample analysis were accessed to determine if the patients suffered the haematological signs and neurological symptoms typically associated with ZICD.
This study was a retrospective review of clinical practice, and ethical approval was not considered necessary by the local medical ethics committee.
Results
Patient details, diagnosis and haematological and neurological symptoms and outcome.
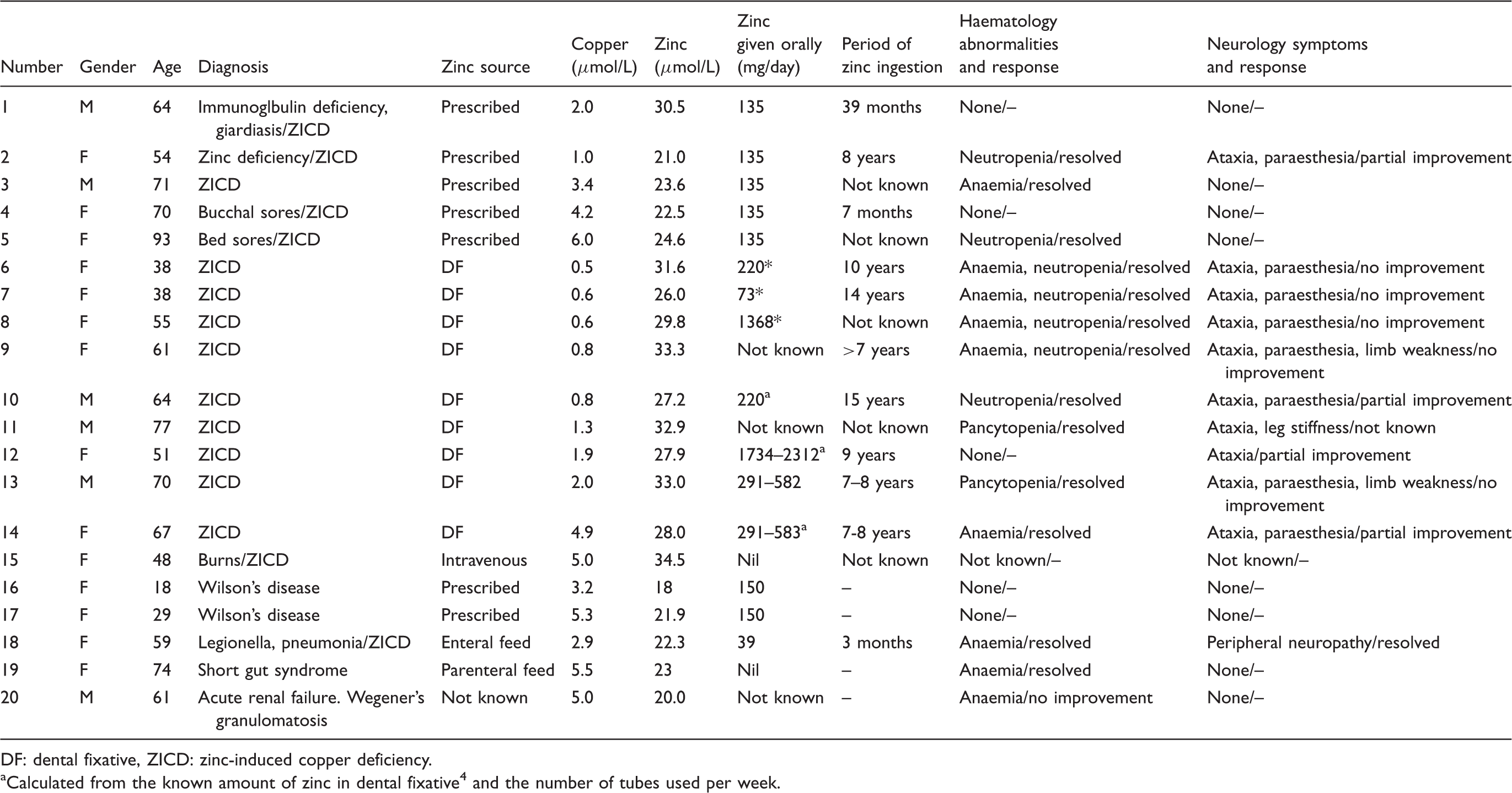
DF: dental fixative, ZICD: zinc-induced copper deficiency.
Calculated from the known amount of zinc in dental fixative 4 and the number of tubes used per week.
Five patients (1 to 5) were prescribed 135 mg/day zinc. Three of these patients had anaemia and/or neutropenia, both of which are in keeping with ZICD, and which resolved when zinc prescription was stopped, and two patients were symptom-free.
Nine patients (6 to 14) were over-applying dental adhesives containing high concentrations of zinc (described more fully elsewhere)3,11,12 and had haematological signs and/or neurological symptoms in keeping with ZICD. All patients showed resolution or improvement of these signs and/or symptoms on stopping the application of these dental adhesives and starting copper supplementation. Eight of the nine patients had haematological abnormalities which subsequently resolved in all. Eight of the nine patients had neurological symptoms of which only three showed some improvement on treatment.
One patient (15) had suffered severe burns, which may be associated with low plasma copper concentrations.13,14 She was treated with intravenous Decan, delivering 10 mg/day zinc (and 0.48 mg/day copper) that may have accounted for her high plasma zinc concentration.
Two patients (16 and 17) had Wilson’s disease accounting for their low plasma copper concentrations. Both were treated with 150 mg/day zinc alone.
One patient (18) with pneumonia and sepsis was enterally fed with a zinc-containing feed (Jevity, zinc composition: 23 mg/L zinc). Her daily zinc intake was calculated at 39 mg. She was anaemic and had peripheral neuropathy. Although these findings resolved when the Jevity feed was stopped, they were thought to be due to her critical illness rather than copper deficiency.
One patient (19) was fed entirely parenterally and so in the absence of oral nutrition she did not have ZICD. The period of time when her plasma copper was low and plasma zinc was high coincided with a time when her usual trace element feed, Additrace (Fresensius-Kabi, Cheshire, UK), which provided 6.5 mg/day zinc and 1.6 mg/day copper, was unavailable and her trace element supplementation was changed to a preparation with lower copper and higher zinc concentrations: Decan (Baxter Healthcare Ltd) which provided 10 mg/day zinc and 0.48 mg/day copper.
The final patient (20) was in an Intensive Care Unit undergoing treatment for renal failure associated with Wegener’s granulomatosis. At the time this patient was being treated, Intensive Care Unit patients were commonly treated with 135 mg zinc/day; however, detailed medical records were not available for this patient, and it is not clear if this would explain the high plasma zinc result.
Discussion
This study demonstrated that the combination of consistently high plasma zinc and low plasma copper concentrations is rare, occurring in less than 0.5% of patients tested in our cohort. Three of the 20 patients (15%) can be excluded from further consideration as one (15) was treated intravenously with zinc because of burns, 15 one was entirely parenterally fed (19), and high zinc intake could not be excluded in the other (20) because of a lack of available information. In the remaining 17 patients (85%), the oral intake of zinc was high.
In two of the 17 patients (15 and 16), the hypocupraemia was caused by Wilson’s disease which was treated with the recognized treatment of high-dose oral zinc. 16 Although tissue concentrations of copper are very high in Wilson’s disease, such patients are nevertheless susceptible to copper deficiency following long-term high-dose zinc treatment. 17
Of the 15 patients remaining, all were diagnosed as copper deficient secondary to the ingestion of doses of zinc significantly over the recommended nutrient intake of 5.5 to 9.5 mg/day for men or 4 to 7 mg/day for women. 18 For the cohort of patients studied here, the combination of a high plasma zinc and low plasma copper concentration is therefore 100% specific for ZICD if other causes of hypocupraemia have been excluded. This finding accords with known causes of hypocupraemia or hyperzincaemia since high oral intake of zinc is the only cause found in both: isolated hypocupraemia is associated with a high oral intake of zinc, 19 gastric surgery, 20 severe burns,19,20 untreated coeliac disease 21 and inborn errors of metabolism including Wilson’s disease, acaeruloplasminaemia and Menkes disease and its milder variants; isolated hyperzincaemia is associated with high oral intake of zinc, inappropriate sample collection and the genetic disorder hypercalprotectinaemia. 22
In 10 of these 15 patients (67%), the clinician was unaware of the possibility of ZICD until contacted by the clinical biochemist and as a result, treatment or prevention (by removing the source of zinc/replacing copper) was initiated earlier than it would otherwise have been.
The sensitivity of hypocupraemia and hyperzincaemia in detecting ZICD could not be determined in this study. In 8% of previously reported cases of ZICD, the plasma zinc was within reference limits suggesting a sensitivity of 92%. 8 However, from our experience in which we detected four cases where plasma zinc concentrations were normal, we would judge the sensitivity to be considerably less than this. In previously reported cases of ZICD in which urine zinc was measured, concentrations were elevated in all and so we advocate the measurement of both urine and plasma zinc. 8
In a review of previously published cases, 8 the minimum oral intake associated with ZICD was 121 mg/day, 23 although considerably higher intakes have been recorded.4,5,8 However, in our study, two patients (7 and 15) were affected with zinc intakes of considerably less than 100 mg/day (73 mg/day and 39 mg/day respectively). It is difficult to definitively calculate the upper tolerable intake limit for zinc and, in turn, the oral zinc intake below which copper deficiency can be discounted. Consequently, there is no clear consensus on the safe daily intake of zinc, with cut-offs ranging from 25 mg/day set by UK Food Standards Agency 18 and the European Commission, 24 to 40 mg/day by the US Institute of Medicine 25 and 45 mg/day by the World Health Organization, 26 to 60 mg/day by the US Environment Protection Agency. 27 Ideally, these estimates should also be corrected for weight and possibly also gender. These upper limits are likely to be further complicated by individual variations in bioavailability, sensitivity to zinc and resistance to inadequate copper provision. For example, patient 1 who was prescribed 135 mg/day zinc had developed no symptoms of copper deficiency by three years (although his compliance was not known), while the copper requirement in patient 18, who ingested 39 mg zinc/day, was likely to be higher while in the intensive care unit for treatment of sepsis and pneumonia. The length of time that patients ingested large amounts of zinc is also important as was seen in seven (64%) of the 11 patients in whom this information was known, who were over-applying dental adhesives for over seven years before symptoms developed. This finding is consistent with previous case reports.8,11,28
Severe neurological abnormalities such as peripheral neuropathy and myelodysplasia were present in 9 of 10 patients with very low copper concentrations of ≤2.0 µmol/L but only one of eight patients with copper concentrations of 2 to 6 µmol/L, suggesting the degree of copper deficiency broadly correlates with severity of symptoms. However, two patients prescribed with zinc (patients 1 and 4) with low copper concentrations (2.0 and 4.2 µmol/L) had no symptoms of copper deficiency. This may be due to the length of time of zinc treatment, differences in compliance or variations in sensitivity to hypocupraemia. There was little correlation between plasma copper and zinc concentrations (r2 = 0.23) possibly due to the limited numbers of patients or individual variations in zinc bioavailability, sensitivity, its rate of excretion and copper reserves.
In conclusion, this study found that a low plasma copper (≤6 µmol/L) in conjunction with a high plasma zinc (≥18 µmol/L) is strongly predictive for the diagnosis of ZICD. This combination of results therefore offers the reporting clinical biochemist an important opportunity in alerting the clinician to the likely diagnosis of ZICD so expediting its appropriate treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The North Glasgow Hospitals Trust Ethics Group confirmed that ethical approval was not required.
Guarantor
AD.
Contributorship
AD wrote the manuscript.
IM provided clinical overview.
DT gave statistical and general advice on content.
All authors reviewed the submitted manuscript.