
Abstract
Adequate iodine intake is important during pregnancy as it is a component of the thyroid hormones that are crucial for fetal brain and neurological development. While randomized controlled trials in severe iodine deficiency have shown that iodine deficiency in pregnancy causes impaired offspring cognition, less is known of the effects in regions of mild/mild-to-moderate deficiency. The United Kingdom is now classified as mildly iodine deficient by the World Health Organization, based on a 2011 national study of 14–15-year-old schoolgirls. As pregnancy is the most critical time for brain development, we evaluated iodine status in pregnant women in Surrey (n = 100) and Oxford (n = 230). The median urinary iodine concentration was 85.3 μg/L in Surrey women, considerably lower than the WHO/United Nations Children’s Fund/International Council for the Control of Iodine Deficiency Disorders cut-off of 150 μg/L. Oxford women had similarly low status. We investigated whether that level of iodine deficiency was associated with adverse child cognitive effects using stored samples and data from the Avon Longitudinal Study of Parents and Children cohort. In adjusted analyses, we found a significant association between low maternal iodine status in early pregnancy (urinary iodine-to-creatinine ratio <150 μg/g) such that children had an approximately 60% greater risk of being in the bottom quartile of scores for verbal intelligence quotient, reading accuracy and comprehension. UK women who might become pregnant should ensure they have adequate iodine status to avoid compromising their children’s brain development.
Role of iodine and importance in pregnancy
Adequate iodine intake is important during pregnancy and early life as it is a component of the thyroid hormones, thyroxine and triiodothyronine, which are crucial for fetal brain and neurological development. 1 The World Health Organization (WHO) considers iodine deficiency to be the single most important preventable cause of brain damage worldwide. 2 It is also accepted that the so-called ‘Iodine Deficiency Disorders’ that include goitre, cretinism and endemic retardation, are largely the result of inadequate thyroid hormone production owing to inadequate iodine intake. 1
According to WHO/United Nations Children’s Fund (UNICEF)/International Council for the Control of Iodine Deficiency Disorders (ICCIDD), the recommended iodine intake for adults (>12 years) is 150 μg/day but this rises to 250 μg/day in pregnancy. 2 This higher recommendation in pregnancy is to facilitate the 50% surge in thyroid hormone production that occurs during early pregnancy, to cover increased renal loss of iodine and to supply iodine to the fetus for its own thyroid hormone production from mid-gestation. 1
Iodine status measurement
Iodine status in a population is measured by urinary iodine concentration in a spot-urine sample, based on the fact that 90% of iodine intake is believed to be excreted in urine. 1 For an individual, owing to variable daily intake and hydration status, spot-urine samples are not accurate. Hydration status can be corrected for to some extent by measuring urinary creatinine and computing the iodine-to-creatinine ratio (μg iodine/g creatinine). 3 For a population, median urinary iodine concentration in adults should be 100–199 μg/L while in pregnant women, the concentration should be in the range 150–249 μg/L. 2
Historical picture of iodine deficiency in Britain
Historically, iodine deficiency was widespread in Britain with high rates of goitre and even of cretinism in some regions. Indeed, goitre was still present in many areas until the 1960s. 3 Farmers began iodine supplementation of their livestock to improve reproductive performance and lactation in the 1930s and iodine-containing disinfectants (iodophors) were introduced for teat dipping and cleaning of dairy equipment. Hence, milk became an excellent iodine source. Not long afterwards, milk consumption increased owing to the provision of free school milk and successful advertising by the Milk Marketing Board. As a consequence, a three-fold increase in iodine intake occurred between the 1950s and the 1980s and overt goitre disappeared. 3 In the years that followed goitre eradication, there were no surveys of UK population iodine status and indeed until 2011, the UK was one of the few countries worldwide that was classified by WHO as having ‘no data’.
Re-emergence of iodine deficiency
In 2011, the first national survey of iodine status for more 60 years was published based on spot-urine samples from over 737 girls of 14–15 years from nine locations across the UK. 4 The median urinary iodine concentration (UIC), at 80.1 μg/L, revealed mild iodine deficiency in the cohort on the basis of the WHO cut-off for adequacy in adults of 100 μg/L. 2 Concern began to be expressed that iodine status in the UK was no longer adequate.
Iodine status of UK pregnant women
As pregnancy is the most critical time to have an adequate iodine status, we evaluated iodine status in pregnant women in both Surrey 5 and Oxford. 6 In Surrey, we recruited 100 first-trimester pregnant women during the summer months. The median UIC (85.3 μg/L) was considerably lower than the WHO/UNICEF/ICCIDD cut-off, 2 as was the iodine-to-creatinine ratio (122.9 μg/g), suggesting deficiency; women who were not taking an iodine-containing prenatal supplement (58%) had significantly lower iodine status than those taking such a supplement. 5 In Oxford, 230 women recruited to a selenium and pre-eclampsia trial provided urine samples at 12, 20 and 35 weeks of gestation. 6 Only 2% of the women were taking an iodine-containing supplement. The median UICs were 42.0, 52.0 and 69.4 μg/L, respectively, suggesting mild-to-moderate deficiency. 6 The corresponding median iodine:creatinine ratios were 102.5, 120.0 and 126.0 μg/g, respectively.
Effect of mild-to-moderate iodine deficiency in pregnancy on cognitive outcomes in the offspring
While studies in regions of severe iodine deficiency have shown that prenatal iodine deficiency causes impaired cognition, much less is known of the effects in regions of mild or mild-to-moderate deficiency. There are very few studies and no randomized controlled trials in such areas. While some studies found a benefit of higher status or supplementation in pregnancy, not all were positive. We wanted to know whether the level of iodine deficiency in pregnancy that exists in the UK, i.e. mild-to-moderate, had adverse cognitive outcomes for the children.
We investigated the association of iodine status in pregnancy and cognitive outcomes in the children in pregnant women of the Avon Longitudinal Study of Parents and Children (ALSPAC) cohort. 3 ALSPAC enrolled a total of 14,541 pregnant women in the early 1990s and collected biological samples, including urine. Data have been collected on the health and development of their children ever since. In stored spot-urine samples, we measured urinary iodine and creatinine concentrations. Data were available on the children’s intelligence quotient (IQ) at age 8 years and reading ability at age 9 years.
The women were classified as mildly-to-moderately iodine deficient (median UIC 91.1 μg/L; median iodine:creatinine 110 μg/g). We defined the women as being deficient if their urinary iodine was <150 μg iodine/g creatinine; 67% fell into that group. 3
For cognitive outcomes, the adjusted (21 confounders) odds ratio for a child being in the bottom quartile of IQ or reading ability if the mother’s UIC was <150 rather than ≥150 μg/g creatinine were as follows.
3
Verbal IQ (OR 1.58, 95% CI 1.09 to 2.30). Reading accuracy (OR 1.69, 95% CI 1.15 to 2.49). Reading comprehension (OR 1.54, 95% CI 1.06 to 2.23).
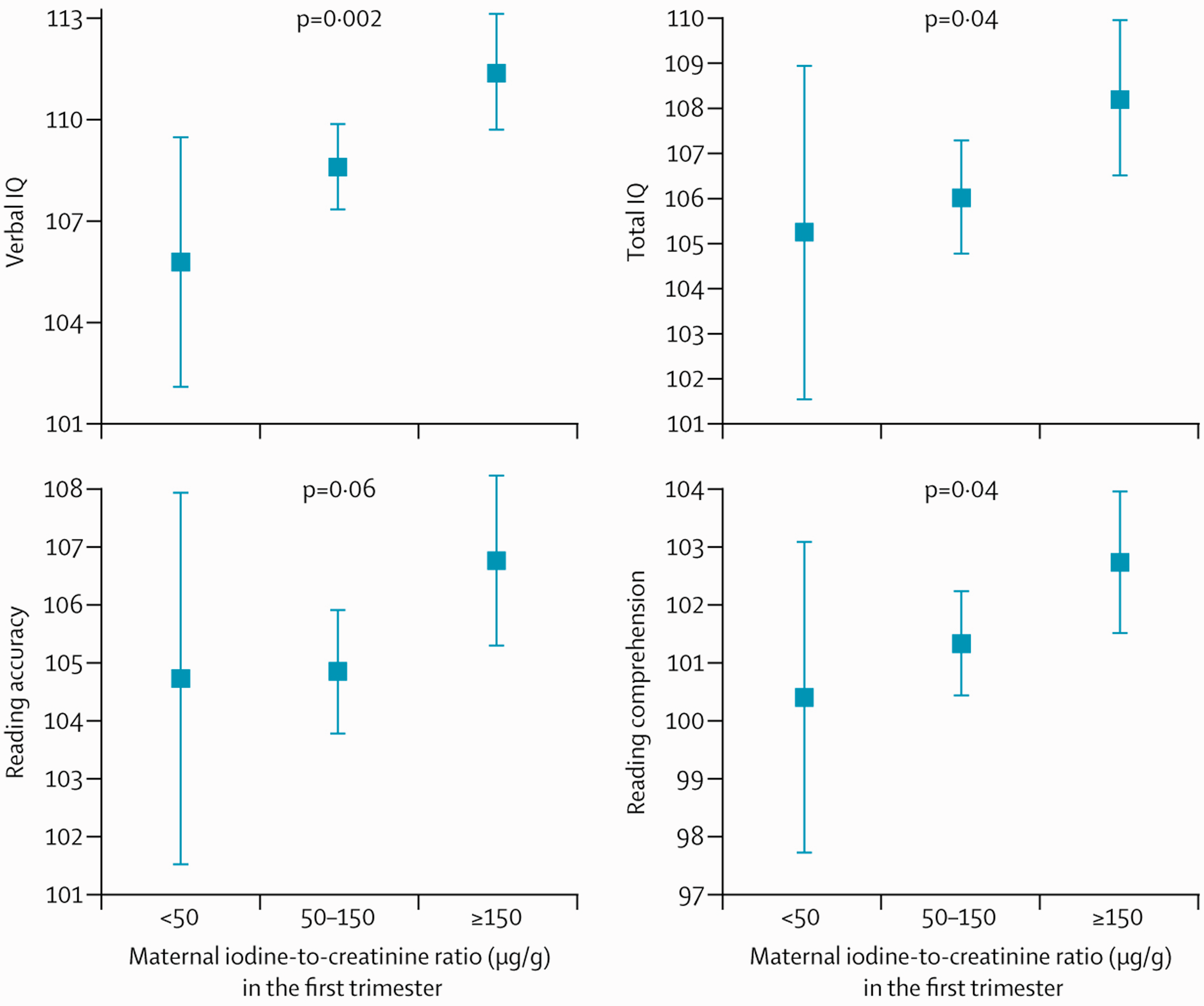
When we sub-divided the deficient category into mildly-to-moderately deficient (50–150 μg/g) and severely deficient (<50 μg/g) categories, we found a significant trend to worsening effects on verbal IQ, total IQ and reading comprehension the more severe the level of iodine deficiency (Figure 1).
Mean (95% CI) scores for child cognitive outcomes according to maternal iodine status in the first trimester (urinary iodine/creatinine ratio), categorized as <50 μg/g and 50–150 μg/g and ≥150 μg/g. Values are adjusted for the effect of confounders. Child verbal and total IQ were assessed at age 8 years, reading accuracy and comprehension at age 9 years. (Reproduced with permission from Bath et al.
3
)
To conclude, our study in the ALSPAC cohort showed that mild-to-moderate iodine deficiency in pregnancy is sufficient to have an adverse effect on childhood brain development, as shown by significantly lower verbal IQ at age 8 years and significantly lower reading accuracy and comprehension at age 9 years and that, furthermore, the adverse effects increase, the greater the level of deficiency.
UK women of childbearing age and pregnant women need to be informed of the consequences of poor iodine intake in pregnancy for any children they may bear. They should be advised to increase their iodine status, preferably prior to pregnancy. Though the richest source of iodine is fish and seafood, the major contributor to iodine status is dairy products, especially milk. 5 Health professionals can direct women to our ‘Iodine food-fact sheet’, endorsed by the British Dietetic Association (https://www.bda.uk.com/foodfacts/Iodine.pdf, accessed 29 June 2015) to help them increase their iodine intake.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All work reported in this review article had full ethical approval – refer to original papers for details.
Guarantor
MPR.
Contributorship
MPR wrote the paper and SCB critically revised it.