
Abstract
Introduction:
Insulin resistance is a frequent abnormality in chronic kidney disease (CKD) appearing in early stages. Factors known to promote insulin resistance in CKD patients include disorders of ion and acid–base equilibrium and circulating uremia toxins. Recent research has focused on the central nervous system as the source of the brain-derived neurotrophic factor (BDNF). The aim of our work was to study plasma BDNF concentrations in stage 3 and 4 CKD patients in relationship with insulin resistance and distribution of adipose tissue.
Method:
Plasma BDNF concentrations were measured in a study group of 31 patients, including a subgroup of 20 non-diabetic subjects. Additionally dual-energy X-ray absorptiometry (DXA) was performed. Homeostatic model assessment of insulin resistance (HOMA-IR) and homeostatic model assessment of B-cell function (HOMA-beta) indices were calculated.
Results:
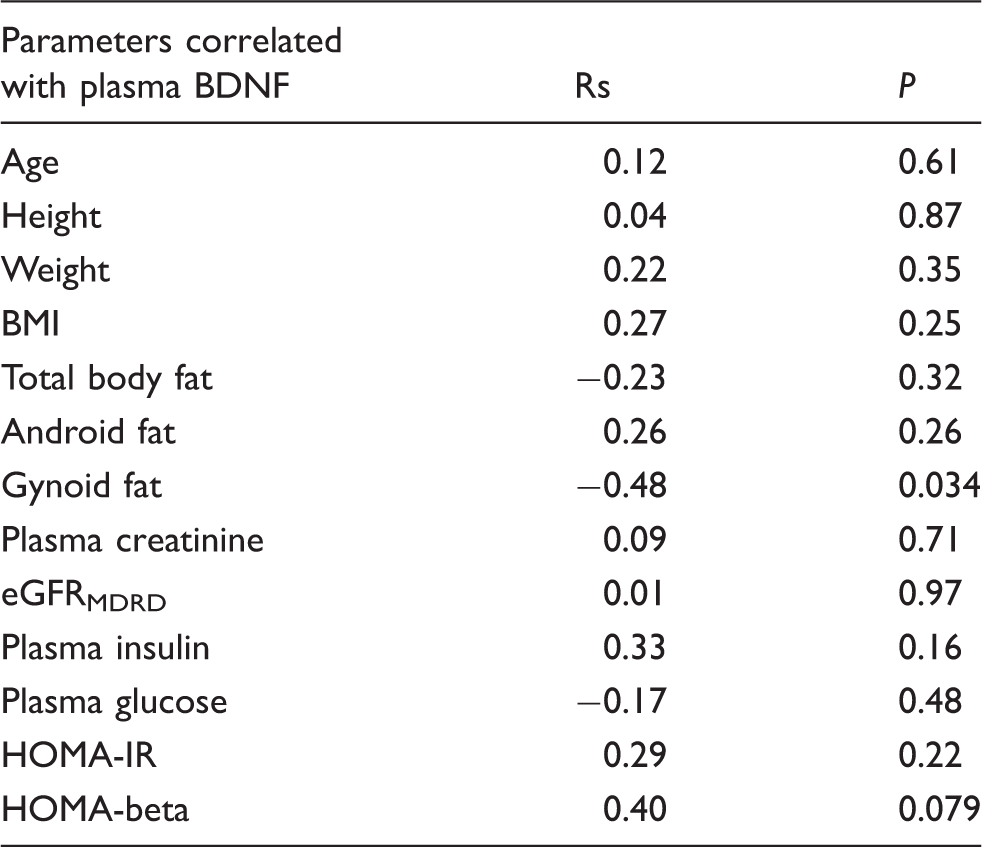
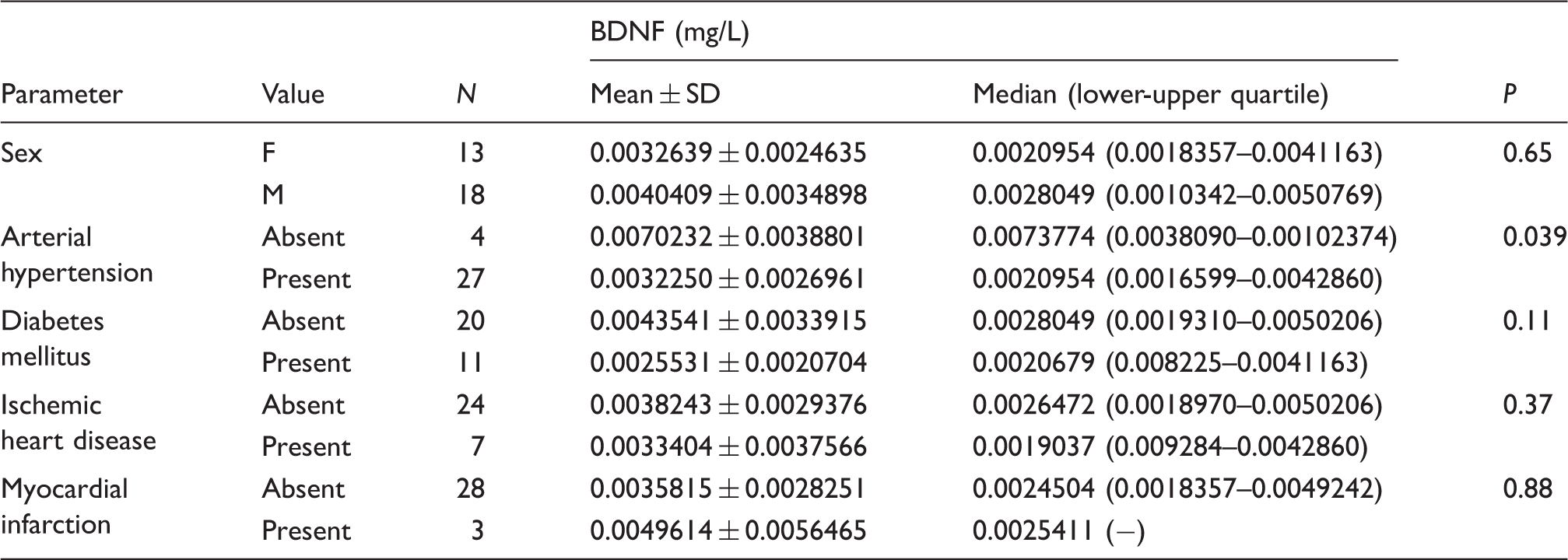
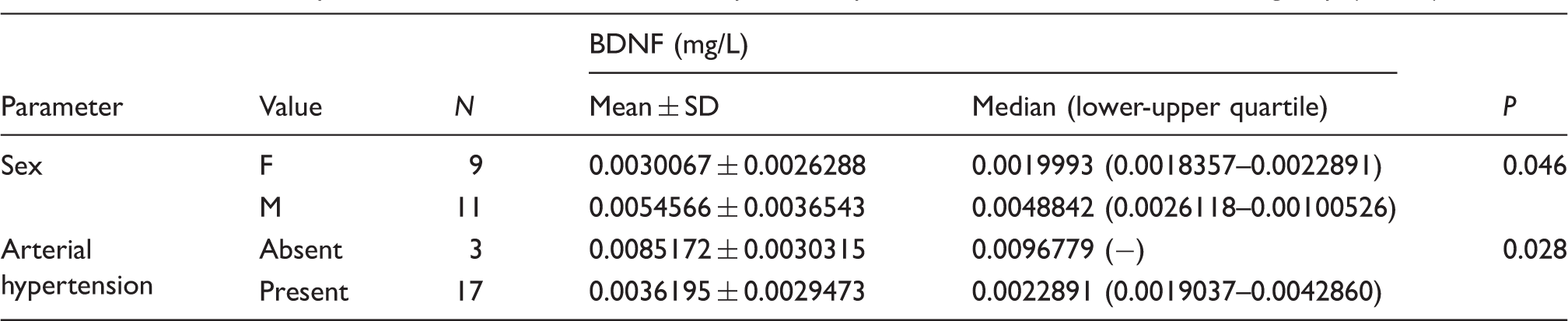
Two separate analyses were performed. In the first analysis performed in all 31 CKD patients, there were no correlations between BDNF and: body mass index (BMI), android, gynoid fat distribution, HOMA-IR and HOMA-beta. In the second analysis performed in 20 CKD patients without diabetes, BDNF was negatively related to gynoid fat (Rs = −0.47, P = 0.034) and women revealed significantly lower levels of BDNF than men (P = 0.046). Normotensive patients disclosed significantly higher BDNF levels than hypertensive patients in the whole CKD group (P = 0.039) and in the non-diabetic subgroup (P = 0.028). No correlations between BDNF and eGFR were found.
Conclusions:
Female sex and arterial hypertension are associated with lower BDNF plasma concentration in CKD patients.
Introduction
Insulin resistance (IR) is a disorder of glucose homeostasis notable for reduced sensitivity of target tissues to insulin, while insulin levels tend to be normal or elevated. The hyperinsulinemic euglycemic clamp is the gold standard for IR confirmation but routine practice often relies on simpler tests, like homeostatic model assessment of insulin resistance (HOMA-IR). Contributory factors include sedentary lifestyle, obesity, overweight, waist circumference in women/men >80 cm/>94 cm, respectively, arterial hypertension, hypertriglyceridemia, and reduced high-density lipoprotein (HDL) concentration in serum. IR is often a predecessor of the metabolic syndrome, diabetes mellitus type 2, cardiovascular disease, obstructive sleep apnea, and the polycystic ovary syndrome. 1 Moreover, IR is a frequent finding in patients with chronic kidney disease (CKD), 2 appearing at an early stage, progressing in proportion to the decreasing glomerular filtration rate (GFR), and demonstrating features of postreceptor IR. 3 Factors known to promote IR in CKD patients include disorders of ion and acid–base equilibrium, as well as uremia toxins circulating in the bloodstream. Considering the fact that the survival of CKD patients is markedly shorter because of accompanying cardiovascular comorbidities, it is important to search for risk factors of atherosclerosis beyond the scope of factors typical and specific for a CKD. In this connection, the role of IR in shorter survival times of CKD patients needs careful consideration. It is worth adding that recent research has focused on the central nervous system as the source of the brain-derived neurotrophic factor (BDNF).
BDNF is a growth and differentiation factor for neurons participating in cognitive and memory processes. 4 BDNF receptors are located throughout the central nervous system (CNS) in centers controlling body mass, and peripherally in the adipose tissue, liver, smooth, and striated muscles. It is believed that BDNF is a regulatory factor in energy homeostasis. 5 Animal experiments revealed that BDNF introduced into cerebral ventricles of mice inhibited food intake and body weight gain. 6 Intravenous BDNF in obese diabetic mice reduced food intake and blood glycemia levels with a consequential alleviation of IR. 7 A study performed in a group of Wilms tumor, aniridia, genitourinary anomalies, and mental retardation (WAGR) syndrome subjects (a genetic defect associated with WAGR) revealed in several cases co-existing symptoms such as hiperphagia and obesity. WAGR syndrome is described as a “gene deletion syndrome” as the PAX6 and WT1 genes are always deleted on the short arm of chromosome 11p13 in humans with the typical signs and symptoms of this disorder. The BDNF gene is localized on the chromosome 11p11.1 being one of the neighboring genes and in 58% of people with WAGR syndrome the deletion includes this nearby BDNF gene region. Higher levels of body mass index (BMI) were observed in subjects with WAGR syndrome including the deletion in chromosome 11p11.1 comparison to the subjects without this deletion. 8 Low BDNF levels have been observed in CNS degenerative processes, among them Alzheimer’s, Huntington’s, and Parkinson’s disease. 9 Type 2 diabetes patients have lower levels of BDNF irrespective of coexisting obesity. 10
In CKD patients, IR is an independent cardiovascular mortality risk factor. 11 Here, the mechanism of IR differs from type 2 diabetes: hepatic glucose uptake and synthesis in the liver are not impaired. 2 The aim of our present work was to study circulating plasma BDNF concentrations in stage 3 and 4 CKD patients in relationship with IR and distribution of adipose tissue.
Material and methods
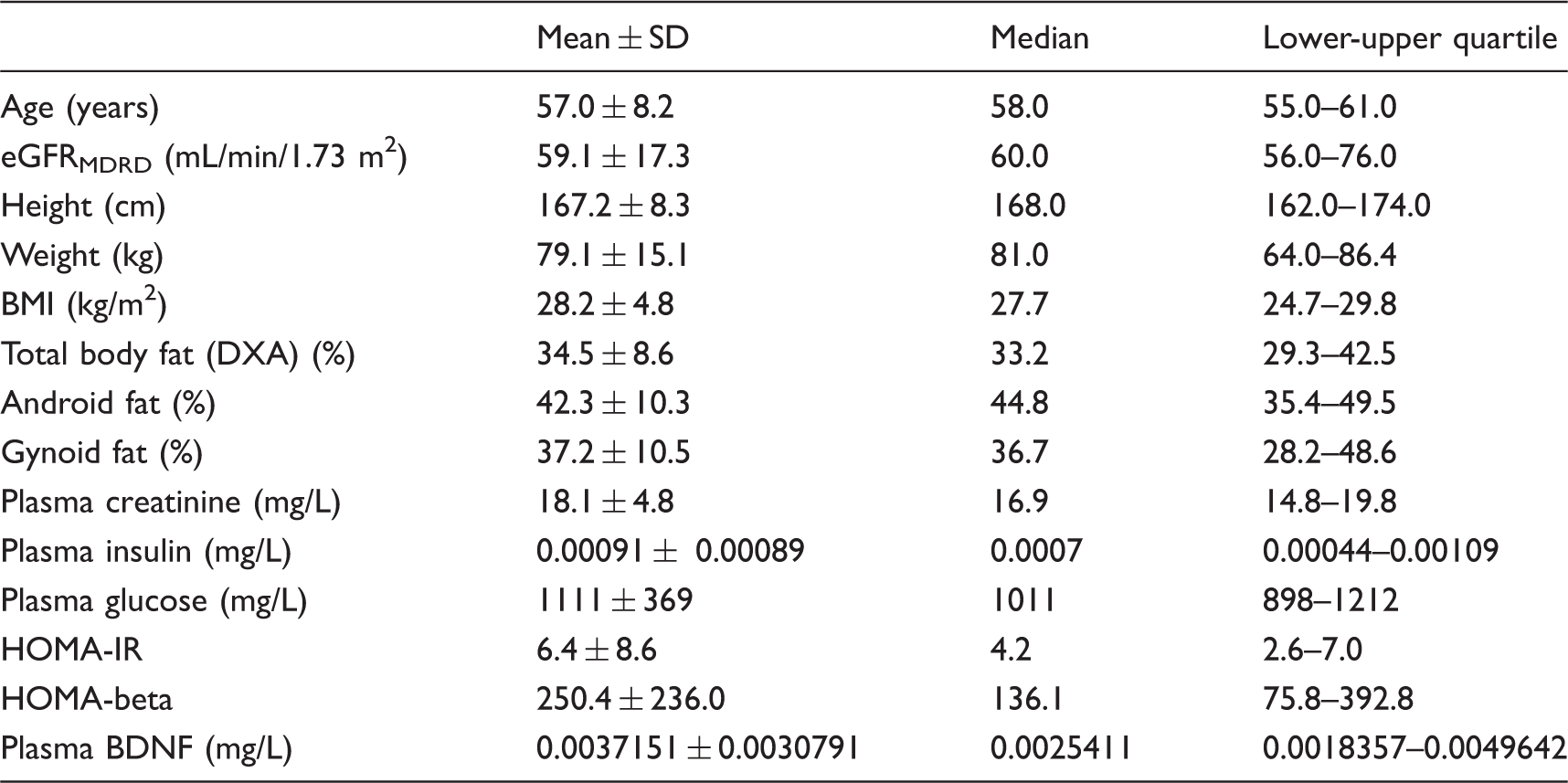
Characteristics of the whole study group (n = 31).
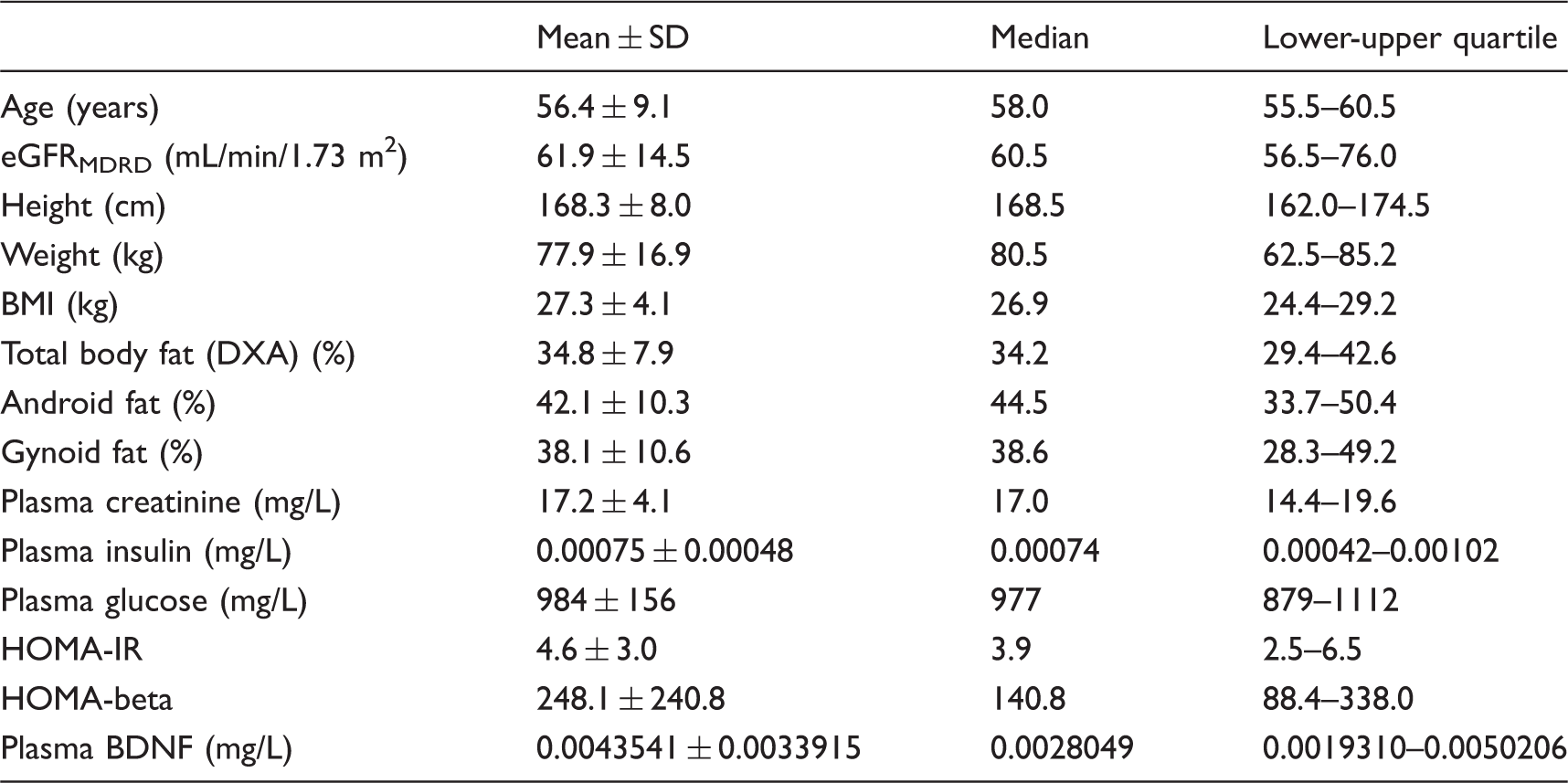
Characteristics of the non-diabetic subgroup (n = 20).
Patients were managed with angiotensin convertase inhibitors or angiotensin receptor blockers (n = 25), calcium channel blockers (n = 13), and beta-blockers (n = 14). This therapy was maintained for three months preceding the study. Exclusion criteria included depression (taking into account ICD 10 criteria), dementia, active inflammation, and tumors. Statistical analysis was done in the whole study group (n = 31) and in the subgroup of patients without diabetes (n = 20). The Bioethics Committee of the Pomeranian Medical University in Szczecin approved the study protocol.
Blood was collected after an overnight fast in tubes containing potassium EDTA, centrifuged at 6500 g for 15 min at 4℃ and the plasma was stored at −70℃. Glucose and creatinine concentrations were measured spectrophotometrically with commercial test kits (Aqua-med, Łódź, Poland), and insulin was determined with INSULIN ELISA test kit (Labor Diagnostika Nord).
Plasma concentrations of BDNF were measured with ELISA Quantikine test kit (R&D Systems, Minneapolis, MN) according to the manufacturer's protocol. The samples were additionally centrifuged at 10,000 g for 10 min at 4℃ before analysis. The calibration was performed with recombinant human BDNF over concentrations of 0.0000625–0.004 mg/L.
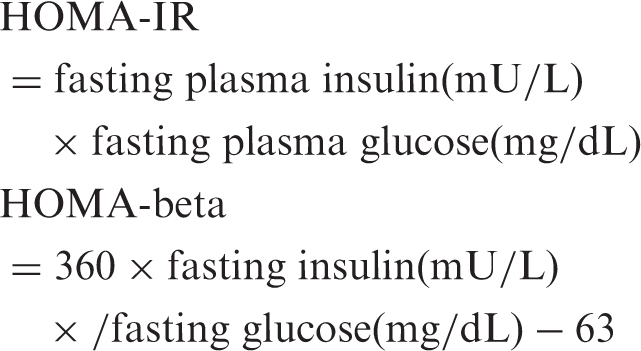
The HOMA-IR and homeostatic model assessment of B-cell function (HOMA-beta) were calculated from fasting insulin and glucose concentrations using the following equations:
Body composition was measured using dual-energy X-ray absorptiometry (DXA) on a Lunar Prodigy Advance instrument. Regional fat mass was obtained from total body scans. The android region has a lower boundary at the pelvis cut and the upper boundary above the pelvis cut lying 20% of the distance between the pelvis and the neck cut. The gynoid region has an upper boundary between the upper part of the greater trochanters and a lower boundary at a distance equal to twice the height of the android region. The android and gynoid fat masses were calculated from these measurements as the percent of total body fat.
Results
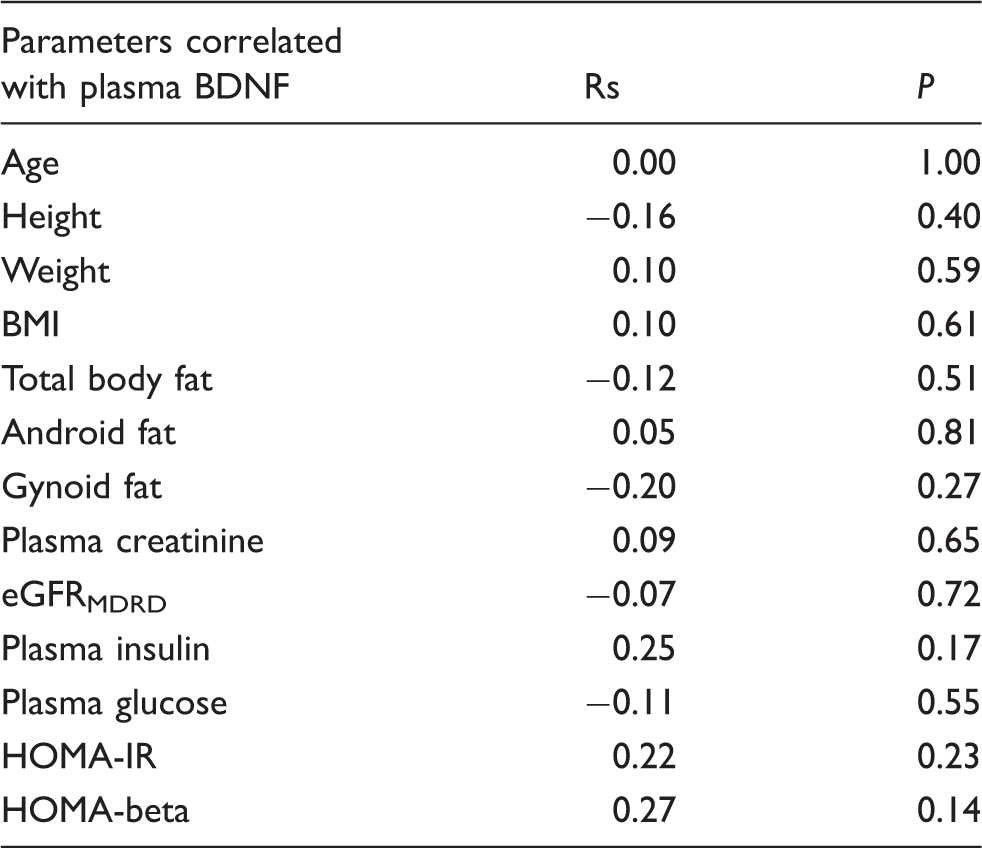
Spearman’s rank correlation coefficients (Rs) for the associations between plasma BDNF concentration and other quantitative parameters in the whole study group (n = 31).
Spearman’s rank correlation coefficients (Rs) for the associations between plasma BDNF concentration and other quantitative parameters in the non-diabetic subgroup (n = 20).
Associations of plasma BDNF concentration with qualitative parameters in the whole study group (n = 31).
Associations of plasma BDNF concentration with qualitative parameters in the non-diabetic subgroup (n = 20).
Discussion
Interrelations between metabolic and neuropsychiatric disorders are currently the object of extensive research. Animal and human studies have convincingly shown that the central nervous system and other centers participating in metabolic processes operate under a common pathophysiologic mechanism. We attempted to find out whether such interrelations exist in stage 3 and 4 CKD. IR was first linked with CKD in the 70s of the past century. However, there are no reports on changes in BDNF induced by impaired glomerular filtration and on associations with IR in CKD patients.
We were unable to disclose any correlations between BDNF and creatinine, eGFR, HOMA-IR, insulin, and glucose concentrations. BDNF correlated negatively with gynoid fat distribution in the non-diabetic subgroup, but not when men and women were analyzed separately; therefore the association seems just to reflect the fact that the women (who had lower BDNF than men) tend to have more gynoid fat than men. No correlation with android fat distribution was found and the positive correlation with HOMA-beta was of borderline significance. Golden et al. reported a positive correlation of BDNF with BMI and body fat mass in women. There is no evidence that BDNF is produced by adipocytes. 12 On the other hand, elevated BDNF concentrations in subjects with excessive fat mass have been attributed to inflammation, which accompanies obesity.
We found differences in BDNF concentrations between women and men, corroborating the report of Pillai et al. on lower plasma levels of BDNF in women. 13 The reason for this sex difference has been ascribed to the effect of estrogens, which are known to upregulate BDNF expression. According to Komulainen et al., BDNF is a marker of cognitive and memory disorders in postmenopausal women. 14 Similar associations have not been observed in men. Low concentrations of BDNF in postmenopausal women have been implicated in depression. In contrast, animal studies have shown that high concentrations of estrogens improve memory. 15
Diabetes mellitus type 2 is a condition with a potent suppressive effect on BDNF concentrations. Krabbe et al. found that BDNF release from the central nervous system is inhibited by high concentrations of glucose. 10 Contrary to this, Suwa et al. reported that patients with freshly diagnosed type 2 diabetes have significantly higher serum BDNF levels than controls and demonstrated a positive correlation between BDNF and HOMA-IR. 16 In our CKD patients diabetes was not associated with BDNF concentration, but associations of BDNF with sex and gynoid fat were found only in the non-diabetic subgroup.
Little is known about BDNF concentrations in CKD patients prior to the first dialysis. It was recently found that a single hemodialysis procedure reduced BDNF levels in chronically hemodialyzed patients, probably due to the oxidative stress that accompanies hemodialysis. 17 Another study in 60 chronically dialyzed patients disclosed higher BDNF concentrations than in control subjects. BDNF levels in diabetic patients were higher than in non-diabetics; no effect of sex was noted. 18
We were unable to demonstrate correlations between BDNF levels and HOMA or eGFR in CKD patients. According to current knowledge, a postreceptor defect in muscles plays a leading role in the mechanism of IR. This multifactorial background may explain discrepant results in various populations of patients. Moreover, hormonal disorders are common in CKD. 19 Thus, sex should be taken into consideration when interpreting the results of research on BDNF, IR, and CKD.
Significantly lower BDNF concentrations in hypertensive subjects were found in the whole CKD group and in the non-diabetic subgroup. Expression of BDNF was upregulated by 17β-estradiol. 20 Telmisartan in hypertensive rats prevented drops in BDNF concentrations through stimulation of BDNF release and TrkB receptor activity in the hippocampus. 21 In a study performed by Prigent-Tessier et al. changes in BDNF concentrations in hypertensive rats (SHR-spontaneously hypertensive rats) and normal rats (WKY – Wistar Kyoto rats) were evaluated. BDNF concentrations were also measured in cultured endothelial cells (CECs) subjected to low and high shear stress. The study revealed that hypertension was associated with decreased expression of BDNF in the endothelium. Authors suggested new perspectives on the role of endothelial BDNF in cardiovascular health. 22
Our conclusions suffer from the small size of our study group (n = 31). The presented P values were not corrected for multiple comparisons and we could not perform reliable multivariate analysis. Nevertheless, we were able to demonstrate that female sex and arterial hypertension are associated with lower BDNF plasma concentration in CKD patients, but no association between BDNF and eGFR was found. Further research should focus on the role of proinflammatory factors and uremic toxins, as well as on the hormonal and mental status in CKD.
Footnotes
Acknowledgments
We would like to thank Barbara Dolegowska for her assistance and guidance in this research.
Declarations of conflicting interest
None.
Funding
This work was supported by National Centre of Science in Poland, grant number N402 564040.
Ethical approval
The ethics committee of the Pomeranian Medical University approved this study (KBI 2013/35).
Guarantor
MM-M.
Contributorship
MM-M and EC researched literature and conceived the study. GD and JS were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. MM-M wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.