
Abstract
Obesity, defined as a body mass index over 30 kg/m2 for adults, poses a major healthcare challenge with important economic, personal and social consequences. Although public health measures, lifestyle change and pharmacological therapies have an important role in the management of obesity, patients with established morbid obesity (body mass index over 40 kg/m2) may also require bariatric surgery. Bariatric or metabolic surgery is associated with effective and enduring weight loss but is also known to improve glucose homeostasis, blood pressure and dyslipidaemia. Patients who have bariatric surgery need lifelong clinical follow-up to identify and prevent nutritional deficiencies and other complications. Clinical biochemistry laboratories have an important role in the nutritional assessment of obese patients and in the identification of complications following bariatric surgery. The aim of this article is to review the different bariatric procedures available and to summarize their complications, especially nutrient deficiencies and those of particular relevance to clinical biochemistry laboratories.
Keywords
Background
The global increase in prevalence rates for obesity, defined as a body mass index (BMI) over 30 kg/m2 for adults, poses a major challenge for healthcare in the 21st century. 1 In 2010, around 25% of adults in the United Kingdom (UK) were obese and the prevalence of obesity in the UK was among the highest in Europe. 2 The current economic cost to UK society is estimated to be over £4 billion per year. 3 A ‘Westernized’ lifestyle with readily available, calorie-dense food and low levels of physical activity fuel this epidemic, by increasing the risk of obesity in genetically susceptible individuals. Unfortunately, limited therapeutic options are available to promote clinically significant and long-lasting weight loss. Effectively reducing the economic, personal and social costs of obesity will require the development of novel therapeutic options coupled with public health measures to address the obesogenic environment.
The most effective treatment currently available for patients with morbid obesity (defined as a BMI above 40 kg/m2) is bariatric surgery. A number of different surgical procedures are used which can promote weight loss, remission of type 2 diabetes and may reduce long-term healthcare costs.4,5 In the UK, the National Institute for Clinical Excellence (NICE) recommends bariatric surgery for patients with a BMI>35 kg/m2 with co-morbidities or BMI > 40 kg/m.2,6 Before considering surgery, patients should be given opportunities to achieve sustained weight reductions using non-surgical measures. In addition, NICE recommends bariatric surgery as a first-line treatment option for patients with a BMI > 50 kg/m2. Some guidelines suggest that in certain patient groups, bariatric surgery may be desirable at lower BMIs (e.g. BMI > 30–35 kg/m2) in patients with significant insulin resistance or resistant type 2 diabetes.7,8 All patients who have bariatric surgery must have access to long-term follow up in specialist clinics with a multidisciplinary team. 6
One of the particular challenges in reducing obesity is that while many patients can achieve weight loss with pharmacological or lifestyle interventions, it is difficult to maintain this weight reduction long term. Bariatric surgery remains the gold-standard treatment to enable patients to achieve and maintain clinically significant weight loss. 4 There is some evidence (most notably from the Swedish Obese Subjects study) that while some regain in weight can occur, most patients maintain a significantly lower weight over significant periods of time compared to patients who do not have bariatric surgery. 9 This long-term weight maintenance is likely to be responsible, at least in part, for some of the other beneficial consequences of bariatric surgery, including reduced overall mortality, reduced co-morbidities such as type 2 diabetes and reduced cancer incidence.10–12
Meanwhile, efforts to find a pharmacological treatment for obesity have proved disappointing due to the risk of side effects and the inability to provide equally successful long-term weight reduction and lifestyle change.13–15 In the UK the number of bariatric procedures remains relatively small, but it continues to rise substantially year by year. In 2003–4 the bariatric surgery rate for England was 1.1 per 100,000 population which had risen to 12.3 per 100,000 population by 2009–10. 16
The aim of this article is to review the use of bariatric surgery in the management of obese patients and to discuss the role of the clinical biochemistry laboratory in the management and monitoring of this patient group.
Normal gut physiology
Anatomically the gastrointestinal (GI) tract includes the mouth, oesophagus, stomach, duodenum, jejunum and ileum, caecum and colon. The liver, gallbladder and pancreas also have important roles in GI function. In normal physiology, the stomach stores the ingested food, mixes it with acid and enzymes and releases the chyme gradually into the small intestine. Hydrochloric acid (HCl) and pepsinogen are produced by parietal and chief cells in the stomach wall. The HCl activates the pepsinogen by converting it to pepsin which initiates protein digestion. The stomach is also responsible for the production and secretion of intrinsic factor which is required for absorption of vitamin B12 in the terminal ileum. Gastric HCl also reduces dietary iron to Fe2+ to facilitate its absorption in the small intestine.
In the duodenum, nutrients from food are mixed with bile from the liver and gallbladder and bicarbonate and enzymes from the pancreas. Bile is required for the emulsification of dietary fats and fat-soluble vitamins to facilitate their digestion by lipases. Pancreatic enzymes such as lipases, proteases and amylases are responsible for the digestion of dietary fat, protein and carbohydrates, respectively. Once the macronutrients have been digested, they are absorbed by the small intestine. Many vitamins and minerals are absorbed in the jejunum but vitamin B12 is uniquely absorbed in the terminal ileum.
Bariatric surgery procedures and their efficacy
Bariatric surgery is a general term for weight loss surgery. The term bariatric surgery covers a wide range of procedures with different mechanisms (see Figure 1). Historically, procedures have been classified according to their primary mechanism as restrictive, malabsorptive or both. Restrictive procedures work by reducing stomach size. Eating a small meal produces distension within the gastric pouch and promotes a feeling of fullness.
17
Malabsorptive procedures bypass portions of the small intestine reducing the opportunity for nutrient absorption. However, malabsorptive procedures have multiple side effects and can lead to chronic malnutrition. They have largely been superseded by procedures with a mixed restrictive and malabsorptive mechanism of action (see Figure 1).
Description of different bariatric procedures and their complications.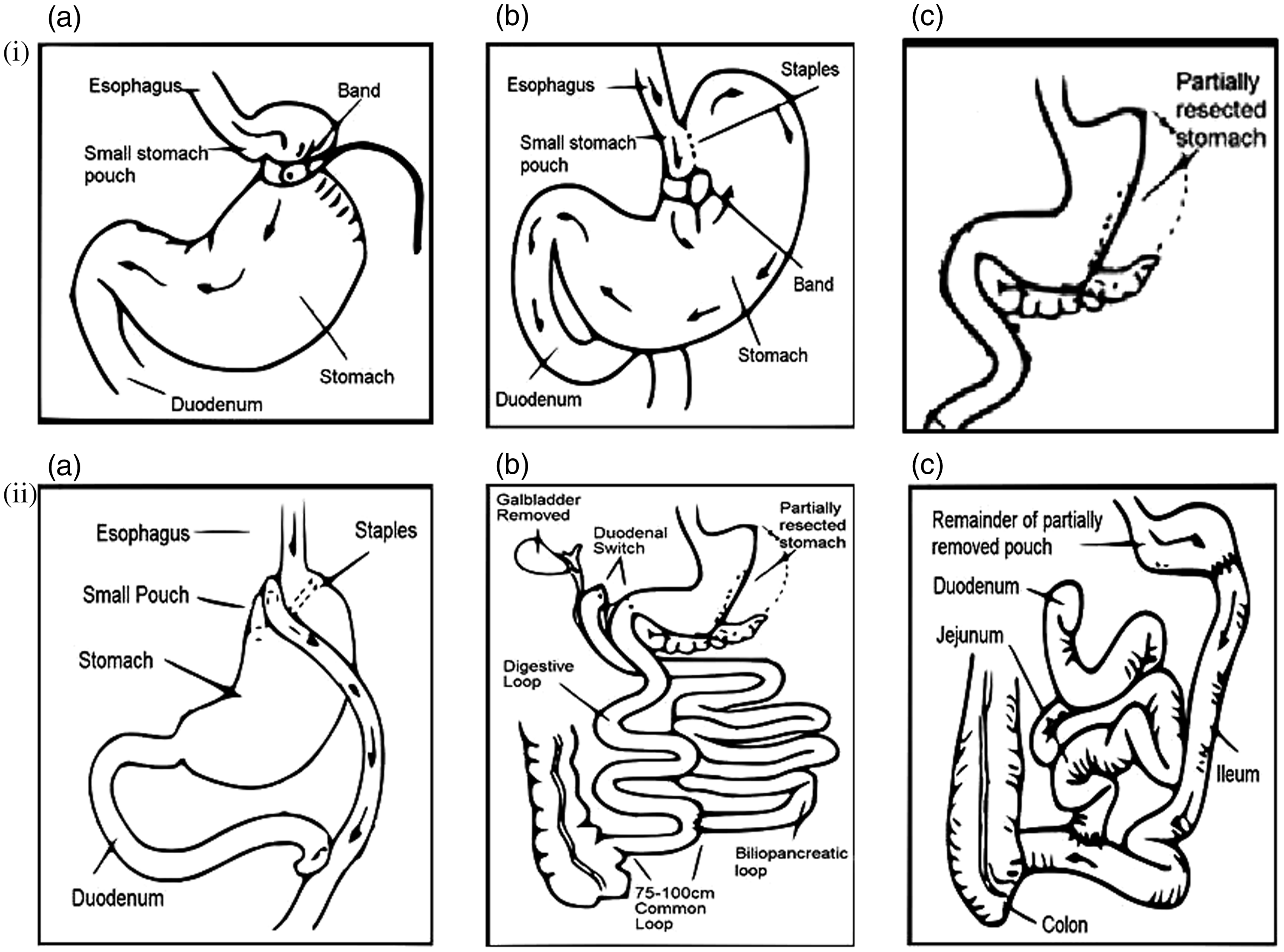
In the UK, the most commonly used bariatric surgery procedures are the gastric band, the Roux-en-Y gastric bypass and increasingly the sleeve gastrectomy. In order to compare treatment efficacy in patients with a wide range of initial weights, the success of these procedures is usually measured as the percentage of excess body weight (EBW) which patients have lost and maintained. The EBW is the amount of weight which is in excess of the patient’s ideal body weight or a BMI of 25 kg/m2.
The laparoscopic gastric band
This is a restrictive procedure in which an adjustable band is placed laparoscopically around the neck of the stomach. This restricts the capacity of the stomach and thus the amount of food that can enter it. There is evidence that the band also acts on vagal efferent nerve fibres to suppress appetite centrally. 18 The amount of weight loss generally experienced after insertion of a gastric band is about 50–60% of EBW. 19
The Roux-en-Y gastric bypass
In this procedure, a small stomach pouch is created and connected directly to the small intestine (alimentary or digestive limb) to bypass around 100–150 cm of the duodenum and jejunum (biliopancreatic limb). The bile and pancreatic secretions still flow along the bypassed part of the small intestine which joins the alimentary limb to allow mixing of secretions and nutrients. Although part of the intestine is bypassed, there are still several metres of small intestine for nutrient absorption. The Roux-en-Y gastric bypass is a procedure with both restrictive and malabsorptive aspects which results in a loss of around 60–75% of EBW. 4
Interestingly, the Roux-en-Y gastric bypass procedure appears to have particular efficacy in inducing remission in patients with type 2 diabetes. 20 Although the precise mechanisms for this are unclear, this phenomenon may be related to increased secretion of anorectic peptides PeptideYY3–36 (PYY) and glucagon-like peptide 1 (GLP-1). 18 These peptides are released from specialized enteroendocrine cells (L-cells) in the small intestine following nutrient ingestion. The delivery of nutrients to lower portions of the small intestine may be responsible for the increased PYY and GLP-1 concentrations seen in patients following Roux-en-Y surgery. 21 GLP-1 is thought to be required for the incretin effect (the pronounced increase in secreted insulin following the administration of ingested, not intravenous, glucose) and is thought to have beneficial effects on glucose tolerance and satiety. 22
Sleeve gastrectomy
The sleeve gastrectomy is becoming increasingly popular in clinical practice and provides comparable weight loss to the Roux-en-Y gastric bypass although long-term follow-up data are awaited. 4 The efficacy of the procedure was initially attributed to the restrictive effects of the sleeve, but there is increasing evidence that the procedure is accompanied by significant changes in the gut hormone profile.17,23,24 Sleeve gastrectomy has reasonable efficacy at promoting diabetes remission although it is slightly less effective than the Roux-en-Y gastric bypass. It is often used as the first stage of a two-step procedure in patients with a BMI > 50 kg/m2 and is sometimes combined with another operation to create a duodenal switch (Figure 1).
Other bariatric surgery procedures
Malabsorptive procedures such as biliopancreatic diversion and duodenal switch can promote more weight loss but involve bypassing large portions of the small intestine which carries an increased risk of complications. These patients are at particular risk of malabsorption and vitamin deficiency and need intensive lifelong monitoring.
Nutritional assessment before bariatric surgery
To be considered for bariatric surgery in the UK, patients have to have appropriate assessment and management by a medical clinic with specialist services (tier 3) and appropriate multidisciplinary team (MDT) input. 6 Such medical MDTs should typically include dedicated physicians, psychologists, nurses and dieticians. Patients who require bariatric surgery are referred to commissioned bariatric surgical centres, where further assessment of the patient is performed. Surgical interventions occur only after medical MDT approval.
Patients referred for bariatric surgery may have a pre-existing nutritional deficiency. For example, in a study of 232 morbidly obese subjects there was a high prevalence of deficiency of zinc, selenium, B12 and 25-OH vitamin D and secondary hyperparathyroidism was common. 25 Although a sedentary lifestyle and lack of exposure to sunlight may contribute to vitamin D deficiency, studies have also suggested that 25-hydroxylation and 1-alpha hydroxylation are impaired in obesity. 26 Some guidelines recommend thorough preoperative nutritional evaluation including selective micronutrient measurements which gives the opportunity to correct any deficiencies prior to surgery. 27
Nutritional support postbariatric surgery
Successful long-term outcomes following bariatric surgery are dependent upon appropriate nutritional support and follow-up. European and American guidelines are now available to guide physicians on the monitoring, identification and treatment of complications.6,8,28
Patients with gastric bands should be advised to maintain a healthy, balanced diet and take a daily complete multivitamin supplement. Regular follow-up assessments are important for the success of this procedure, especially in the first two years. If the band is too loose, then the patient can overeat and will not benefit from the restrictive aspects of band insertion. However, if the band is too tight, patients can experience vomiting and regurgitation of food. If severe, this can paradoxically lead to weight gain as patients choose liquid nutrient sources which can easily pass through the restriction of the band. Deficiencies of vitamins and minerals can also occur as patients cannot tolerate a balanced diet.
Patients with sleeve gastrectomy or gastric bypass are at greater risk of nutritional deficiency compared to patients who have had a gastric band fitted. Close monitoring is required especially in the first two years following surgery, with annual reviews thereafter if clinically stable. Patients at review should be assessed clinically for nutritional deficiency and to evaluate their degree of weight loss. Most patients need to take a complete multivitamin preparation, with B12, calcium, vitamin D and possibly iron supplementation.
The less common procedures of duodenal-switch or biliopancreatic diversion have a much greater malabsorptive component than the Roux-en-Y gastric bypass. These patients can present with significant malabsorptive syndromes and frank malnutrition. 4
Metabolic improvements postbariatric surgery
The term ‘metabolic surgery’ is now widely used when a bariatric procedure is undertaken in a patient with diabetes, which aims to confer long-term benefits in glycaemic control in additional to weight loss. The rationale for this is related to the fact that the benefits in glycaemic control postbariatric surgery are seen several days postsurgery, before any significant weight loss has yet occurred.29,30 It has been hypothesized that the negative calorie balance during and immediately after surgery causes this but it is also possible that altered gut hormone profiles may contribute to this effect. 31
Interestingly, the different bariatric procedures have slightly different effects on the gut hormones. 21 These hormones include ghrelin, GLP-1, cholecystokinin and PYY. There are often abnormalities in these hormones prior to surgery but their contribution to the development of obesity remains unclear. 23 It is thought that both duodenal exclusion (foregut hypothesis) and rapid exposure of the distal ileum to undigested nutrients (hind gut hypothesis) are mechanisms that may lead to the improvement in glycaemic control. 32 The American Diabetes Association now has criteria for assessment of the effects of bariatric surgery on optimization of metabolic status. 33 For type 2 diabetes, complete remission is defined as plasma glucose concentrations in the normoglycaemic range for at least one year, with no active pharmacological therapy or ongoing procedures. After five years, it is considered prolonged remission. Partial remission is defined as plasma glucose concentrations in the hyperglycaemic range but below the diagnostic threshold for diabetes. 33
Other metabolic effects associated with bariatric procedures include improvements in the lipid profile and blood pressure. 34 In female of child-bearing age, fertility can be substantially increased – an effect which is evident quite soon after surgery. 35
Complications of bariatric surgery
These can be classified into early and late complications.
Early complications
In the perioperative period a variety of complications can occur. The most common complications include pulmonary emboli, haemorrhage, chest infections and wound infections. In patients with a gastric band, infection of the gastric band or port site can occur. 4 In patients with sleeve gastrectomy, Roux-en-Y gastric bypass, duodenal switch or biliopancreatic diversion, there is also a risk of anastomatic leakage. 4 These conditions may be hard to diagnose, so a high index of suspicion is required to appropriately identify these complications and arrange radiological and laparoscopic investigations if required. All patients with significant postoperative vomiting may be at risk of acute thiamine deficiency and neurological sequelae.
Patients on antihypertensive and antidiabetic medications may need dramatic down-titration of their medication to prevent postural hypotension and hypoglycaemia, respectively, due to the almost instantaneous improvements of the metabolic status of these patients.
Late complications
Late complications for gastric banding include gastric band slippage, gastric band erosion, band leakage and infection. Roux-en-Y gastric bypass can be complicated by stenoses and internal herniations. 4 From a biochemical perspective, nutritional deficiencies are the most important complication to consider.
Nutrient deficiencies encountered postbariatric surgery
The gastric band is a restrictive procedure which reduces the quantity of nutrients eaten, but provided the quality of the diet is adequate, micronutrient deficiency is uncommon. However, if there is maladaptive eating, especially in the context of an over-tight band or band slippage, nutritional intake may be suboptimal. Patients may be only able to tolerate liquids or solids that quickly liquefy (e.g. ice cream) and the over-reliance on relatively few food types increases the risk of micronutrient deficiency.
In Roux-en-Y gastric bypass, duodenal switch or biliopancreatic diversion, nutrient absorption takes place in the common limb (after the jejunoenteric anastomosis). Thus, the risk of malabsorption is inversely related to the length of the intestine remaining between this anastomosis and the ileocaecal valve. Malabsorption is more common after duodenal switch or biliopancreatic diversion and is uncommon after the Roux-en-Y gastric bypass, unless the common limb is less than 120 cm in length. A study compared outcomes in patients with distal (short limb) Roux-en-Y bypass and long limb Roux-en-Y bypass, which is associated with a longer bypassed section and a shorter common limb. Patients with the shorter common limb had superior weight loss but experienced severe metabolic derangements and required more frequent surgical revisions for protein calorie malnutrition. 36
Macronutrient deficiencies
Protein
Protein deficiency is uncommon with the gastric band or gastric bypass and it is usually seen when combined with poor nutritional intake. Patients may find high protein foods such as meat difficult to swallow. Vegan patients can find it particularly difficult to find appropriate and palatable sources of dietary protein.
Protein deficiency may present with hair loss, loss of muscle mass and oedema. Hypoalbuminaemia is rarely seen but does occur. It is important to exclude other causes of hypoalbuminaemia such as an acute phase reaction and nephrotic syndrome. Nephrotic range proteinuria can occur with obesity-related glomerulopathy (ORG) which has a histological appearance of focal segmental glomerulosclerosis. 37 Although there have been cases showing reversal of ORG following bariatric surgery, it is worth excluding this condition as it may not have been diagnosed prior to surgery. 38
Prealbumin or transthyretin is a transport protein running just before albumin on electrophoresis. It has a relatively short half-life and is sometimes used as an indicator of protein ingestion. However, as with albumin, it is affected by the acute phase response and a C-reactive protein should be measured concomitantly if it is to be used as a nutritional indicator.
Treating patients with protein deficiency requires oral protein supplementation although total parenteral nutrition can be considered in cases where GI function is insufficient to permit normal protein absorption. Revisional bariatric surgery may be required to prevent long-term sequelae. The Endocrine Society recommends a daily protein intake of 60–120 g after bariatric surgery. 39 The American Association of Clinical Endocrinologists (AACE) recommends a minimum daily intake of 60 g up to a maximum of 1.5 g/kg of ideal body weight in the early postoperative period. 28
Micronutrients, vitamins and minerals
Micronutrients are substances that are required in very small quantities for normal functioning of the body. A healthy balanced diet normally provides sufficient quantities of these micronutrients. However, after bariatric surgery, micronutrient deficiencies can occur due to alterations in the diet and malabsorption in the GI tract. Supplementation with a complete multivitamin and mineral preparation is likely to be sufficient in the majority of cases but monitoring of these concentrations may be necessary, particularly in procedures that have a malabsorptive component. The interpretation of micronutrient profiles is not straightforward after bariatric surgery and is affected by a number of factors including the acute phase response.
Vitamin D
Calcium and vitamin D deficiency may occur after all types of bariatric surgery but has the highest incidence after the malabsorptive procedures compared to the restrictive procedures. Calcium and magnesium absorption occur in the proximal small bowel in the duodenum and ileum. There is some evidence that calcium and magnesium absorption may be impaired by reduced contact with gastric acid. This has led to suggestions that calcium citrate rather than calcium carbonate supplements should be used as they are thought to be absorbed more effectively.40,41 In patients who have lost weight, there are other possible mechanisms of decreased calcium absorption including increased production of cortisol and insulin-like growth factor-1 and changes in gut hormones such as ghrelin, leptin and glucagon-like peptide 2. In light of this, consideration should be given to providing higher than the normal recommended daily intake of calcium. 41
Vitamin D is a fat-soluble vitamin which is present in the diet and can be made in the skin under the influence of sunlight. Vitamin D deficiency is common in obese patients. 42 Most guidelines suggest monitoring of calcium, vitamin D concentrations and sometimes parathyroid hormone. Routine postoperative supplementation of calcium and vitamin D is recommended to attain vitamin D target concentrations of around 30μg/L (75 nmol/L). Regular bone density measurements are recommended every 2–5 years. 27
Iron
Iron deficiency is common as exclusion of the stomach prevents the reduction of dietary iron to Fe2+ which is more readily absorbed. Most guidelines recommend monitoring the full blood count and ferritin. An acute phase response makes interpretation more difficult. Prophylactic iron supplementation is recommended in all premenopausal females and in iron-deficient postmenopausal females and males. Iron absorption may be inhibited and enhanced by a number of factors. For example, calcium can reduce iron absorption so the timing of supplementation is crucial to its success. In addition, vitamin C encourages absorption and some preparations even contain both iron and vitamin C in combination. It is helpful to have preoperative iron indices measured to exclude pre-existing iron deficiency, iron overload and haemochromatosis.
Vitamin B12
Vitamin B12 deficiency is likely to occur at some stage in procedures where there is exclusion of the lower part of the stomach which is required for production of intrinsic factor. However, it may occur with other procedures such as gastric banding if there is a low intake of meat or dairy products.
To prevent vitamin B12 deficiency most guidelines suggest giving vitamin B12 prophylactically. 27 Intramuscular or oral preparations can be used. If coagulation is impaired, or there is concomitant vitamin K deficiency, oral, intranasal or sublingual vitamin B12 preparations should be considered.
Folate
As patients are advised to take a multivitamin supplement, it is rare to see folate deficiency. When it occurs it may suggest lack of compliance with the multivitamin preparation. Higher doses and specific supplements, however, will be required in pregnancy for the avoidance of neural tube defects. High concentrations of folate may be suggestive of bacterial overgrowth. 43
Thiamine
Thiamine is primarily absorbed in the jejunum and is required for normal carbohydrate metabolism. Refeeding a malnourished patient can precipitate thiamine deficiency, particularly if carbohydrate-rich foodstuffs are used. Consider thiamine deficiency in patients with intractable vomiting and in those with unexplained cardiological or neurological symptoms. The prevalence of thiamine deficiency in patients with bariatric procedure is low in patients already on a complete multivitamin and mineral supplement, but non-compliant patients will be at risk. There should be a low index of suspicion for this condition, as it is easily overlooked, easily treated and untreated can result in severe and irreversible consequences. Acute deficiency should be treated with specific parenteral thiamine supplementation before any administration of glucose. Oral supplements are suitable for maintenance therapy. 44
Vitamin A
This is a fat-soluble vitamin and deficiency may cause night blindness. Assessment of vitamin A status is particularly important after biliopancreatic diversion and duodenal switch operations where the common limb is short with reduced opportunity for absorption of fat-soluble vitamins. If symptoms are present, vitamin A may need to be specifically replenished.45–47
Vitamin K
Vitamin K is a fat-soluble vitamin which is required for normal function of clotting factors II, VII, IX and X. If clotting function, particularly the prothrombin time (PT) is normal, further assessment of vitamin K status is not usually required, unless there are additional risk factors. If the PT is abnormal or if vitamin K deficiency is specifically suspected, a PIVKA test (protein induced by vitamin K absence) may be done which will look at the functional aspect of the deficiency. If there is evidence of vitamin K deficiency, specific replenishment of vitamin K stores with supplementation will be required. The AACE guidelines recommend measurement of PIVKA in patients who have a coagulopathy, osteoporosis or liver disease only. 28
Selenium
A case report has highlighted the risk of selenium-deficient cardiomyopathy following biliopancreatic diversion. 48 Although most guidelines currently recommend optional monitoring of selenium, it should be considered in patients who have had a malabsorptive procedure and have unexplained anaemia, fatigue, diarrhoea, cardiomyopathy or metabolic bone disease.
Zinc
The AACE guidelines recommend screening for zinc deficiency in all patients who have had a malabsorptive procedure. 28 Zinc deficiency should be particularly considered in patients with pica, an altered sense of taste and males with hypogonadism or erectile dysfunction. There have been case reports of patients who have developed acrodermatitis following zinc deficiency caused by bariatric surgery.49,50
Copper
Copper is widely available in the diet but absorption occurs in the stomach and proximal duodenum and thus deficiency can occur in bariatric procedures such as a gastric bypass. Its absorption is also inhibited by high concentrations of zinc. Copper is required for iron absorption. It converts Fe2+ to Fe3+ which is required for haemoglobin formation and binding to transferrin. Thus, deficiency of copper may result in an iron deficiency which is refractory to iron therapy. In addition, there have been case reports of copper deficiency causing myelodysplasia in a patient following bariatric surgery which improved on replacement with copper. 51 Copper is also involved in other redox reactions and deficiency also results in myelopathy as has been seen in a patient following a duodenal switch operation. 52
There is usually sufficient copper in a complete multivitamin and mineral supplement to prevent deficiency. However, different preparations contain varying amounts of micronutrients and if an isolated deficiency occurs the vitamin and mineral content of the formulation should be reviewed. Due to the use of common gut transport systems, elevated concentrations of one micronutrient may have effects on other dietary components. For example chronically high concentrations of zinc may result in copper deficiency. The AACE guidelines have suggested that patients being treated for zinc deficiency should receive 1 mg of copper for each 8–15 mg of zinc being replaced. 28
Other complications and management issues
Gout
Rapid weight loss can precipitate gout. Patients with a history of gout should be on gout prophylaxis prior to surgery where possible. In one study a third of patients with a previous diagnosis of gout had an acute attack postoperatively. 53
Gall stones
This is a complication of rapid weight loss. For some procedures, such as the Roux-en-Y gastric bypass, a prophylactic cholecystectomy may be considered or postoperative supplementation with oral ursodeoxycholic acid. 54
Enteric hyperoxaluria and renal stones
Malabsorptive procedures may lead to an enteric hyperoxaluria through an abnormal delivery of fat to the colon. The aim of treatment is to reduce the amount of oxalate entering the blood stream by increasing the intracolonic calcium concentration which acts as an oxalate binder. This can be achieved by giving very high doses of oral calcium. 55 However, it is important to exclude hypercalciuria before treatment which would encourage renal calcium stone formation and nephrocalcinosis. Further therapeutic measures include increasing fluid intake and altering urinary pH, for example, with the use of potassium citrate. The AACE guidelines recommend a low oxalate meal plan (although there is little evidence to support this) and probiotics containing Oxalobacter formigenes may be used.
Bacterial overgrowth
Some of the malabsorptive procedures have blind ending loops which may lead to bacterial overgrowth. 56 This may cause the recirculation of bile acids, leading to fat malabsorption and malnutrition. Thiamine deficiency may also be exacerbated by bacterial overgrowth. 43 Traditionally, bacterial overgrowth is investigated using a hydrogen breath test. However, this procedure may precipitate dumping in the postbariatric patient and should be used with caution. False positive results may occur due to the rapid GI transit in patients following gastric bypass. A raised folate concentration can be indicative of bacterial overgrowth. Once the diagnosis has been confirmed, treatment should be initiated with cyclical antibiotics which can result in an improvement in symptoms.
Dumping and postprandial hypoglycaemia
Dumping usually occurs 30–60 min after eating and presents with symptoms of bloating, flushing, diarrhoea and light-headedness. It is usually precipitated by eating highly refined foods. It occurs as undigested calorie-dense liquids and foods cause hyperosmolarity of the intestinal contents causing fluid to be drawn into the intestinal lumen leading to intestinal distension, fluid sequestration, decreased intravascular volume and hypotension. Patients are usually able to recognize the symptoms and alter their eating behaviour accordingly.
Postprandial hypoglycaemia is a relatively common complication of non-banding procedures. It again usually occurs after a highly refined carbohydrate load and can occur with dumping. Postprandial hypoglycaemia can present at any time after the surgical procedure. Some patients do not appreciate the significance of the symptoms of hypoglycaemia (particularly if they did not have diabetes before bariatric surgery). Patients can develop loss of hypoglycaemic awareness. The aetiology of postprandial hypoglycaemia is not fully understood but it is likely to be related to altered gut hormone responses, particularly GLP-1.
The first line of therapy is dietary optimization with adjustment of the eating pattern. If symptoms persist, it is important to try to determine both the severity and the timing of the hypoglycaemic episodes. Point-of-care blood glucose monitoring may provide this information, as patients can record their blood glucose concentrations when symptoms arise using a glucose meter. Continuous glucose monitoring may provide the appropriate information concerning the patient’s hypoglycaemic episodes. A key part of the subsequent investigations is to determine whether this is postprandial hypoglycaemia or fasting hypoglycaemia as an insulinoma may need to be excluded using a 72 h fast. 57 For true postprandial hypoglycaemia, a mixed meal test with measurement of glucose and insulin can be a useful preliminary investigation to confirm the diagnosis.
Postprandial hypoglycaemia can be managed using acarbose, somatostatin analogues, calcium channel antagonists and diazoxide in resistant cases. Reversal of the bariatric procedure may need to be considered if symptoms are severe. 57
Drug prescribing
Consideration of the effects of weight loss and drugs should be given prior to any bariatric intervention. Successful weight loss may result in a reduction of the doses of antidiabetic and antihypertensive medication required and alterations of the doses of these drugs should be made proactively to avoid hypoglycaemia and hypotension. Some drugs are prescribed according to weight and the doses need to be amended following weight loss. Furthermore, altered anatomy following surgery can alter drug absorption. This has been a particular issue for some oral contraceptive, anticonvulsant and immunosuppressant medications. 58
Pregnancy
Despite increased fertility following bariatric surgery, pregnancy within 18 months is not recommended due to adverse consequences affecting both the mother and the fetus. Ideally, the weight would have stabilized before pregnancy is considered.
During pregnancy, there are enhanced nutritional requirements which necessitate very close monitoring of maternal and fetal nutritional status and fetal growth. Pregnancy itself may affect micronutrient requirements as some nutrients are required in higher amounts (such as folate) while others may be toxic to the developing fetus (such as vitamin A). A multivitamin complex which is suitable for pregnant female should be used instead of a standard preparation. 59
Assessing glucose homeostasis in pregnant women following bariatric surgery can be challenging. In most procedures (except gastric banding), an oral glucose tolerance test (OGTT) can precipitate dumping and postprandial hypoglycaemia and would not be recommended. Furthermore, the use of the OGTT in patients with altered GI anatomy has not been validated. HbA1c has some value but is affected by altered red cell turnover in pregnancy and is not sensitive to acute changes in glucose homeostasis. Point-of-care glucose monitoring is probably the best option for assessing glycaemic control in these patients. 59
During lactation, nutrient requirements are often increased. Medications and supplements may need further adjustment. Breastfeeding can be particularly difficult if pregnancy has occurred prior to weight stabilization.
Summary
Bariatric surgery is an effective treatment strategy for patients with obesity which leads to weight loss and improved metabolic health in patients with weight-related co-morbidities, such as type 2 diabetes. There are a range of bariatric procedures available and their use is increasing steadily within the UK. Complications of bariatric surgery include deficiencies of macro- and micronutrients which can be treated with a healthy balanced diet and multivitamin supplementation. Biochemical monitoring of nutritional status is vital for the diagnosis and monitoring of these complications.
Footnotes
Acknowledgements
This article was prepared at the invitation of the Clinical Sciences Reviews Committee of the Association for Clinical Biochemistry and Laboratory Medicine.
Declaration of conflicting interests
None.
Funding
CLM receives salary funding from the Wellcome Trust Translational Medicine and Therapeutics Programme and the European Commission Full4Health 7th framework programme no. 266408.
Ethical Approval
Not required.
Guarantor
AP.
Contributorship
AP and AS planned and wrote the original article. CLM rewrote the article, added referencing and incorporated the reviewers’ comments.