
Abstract
Background
Metabolic syndrome is defined by a clustering of cardiovascular risk factors and is associated with a heightened inflammatory state. A raised serum high-sensitivity C-reactive protein, a marker of inflammation, is also known to associate with cardiovascular risk. We have investigated the relationship between the presence of metabolic syndrome and serum high-sensitivity C-reactive protein concentration in a large representative Persian population cohort without a history of cardiovascular disease.
Methods
The MASHAD study population cohort comprised 9778 subjects, who were recruited from the city of Mashhad, Iran, between 2007 and 2008. Several cardiovascular risk factors were measured in this population without cardiovascular disease. Individuals were categorized into quartiles of serum high-sensitivity C-reactive protein concentration: first quartile – 0.72 (0.59–0.85) (median [range]) mg/L, second quartile – 1.30 (1.14–1.4) mg/L, third quartile – 2.29 (1.92–2.81) mg/L and fourth quartile – 6.63 (4.61–11.95) mg/L, respectively. The prevalence of metabolic syndrome in each quartile was determined using either International Diabetes Federation or Adult Treatment Panel III criteria.
Results
The prevalence of metabolic syndrome was highest in the fourth quartile for serum high-sensitivity C-reactive protein (1220 subjects [50.0%]), and significantly higher than that in the first quartile (reference group) (634 subjects [25.9%]) (P < 0.001). A positive smoking habit (OR, 1.47 [1.26–1.70], P < 0.001) and the presence of either metabolic syndrome-International Diabetes Federation (OR, 1.35 [1.18–1.55], P < 0.001) or metabolic syndrome-ATPIII (OR, 1.40 [1.18–1.50], P < 0.001) were strong predictors of a fourth quartile for serum high-sensitivity C-reactive protein concentration.
Conclusions
There was a significant association between high concentrations of serum high-sensitivity C-reactive protein and the presence of metabolic syndrome among individuals without a history of cardiovascular disease in our Persian cohort.
Introduction
Metabolic syndrome (MetS) is defined by a clustering of several known cardiovascular (CV) risk factors. 1 These include obesity, dyslipidaemia and impaired glucose tolerance, and the presence of MetS is therefore associated with a high risk of subsequent CV disease (CVD). 2 MetS has a high prevalence3–5 and is a serious public health concern in Iran.
High sensitivity C-reactive protein (hs-CRP) is an indicator of a heightened inflammatory state and also appears to be a useful biomarker of CVD risk in both Western6,7 and Iranian societies.8,9 There have been strong recommendations to use serum hs-CRP in CVD risk assessments.10,11
The inflammatory state associated with MetS may contribute to the atherosclerotic process and the use of serum hs-CRP in individuals with MetS has been discussed previously. 12 We wished to determine whether, in individuals without a history of CVD, serum hs-CRP was a discriminant for the presence of MetS.
Material and methods
Subjects
The study population was recruited between 2007 and 2008 using a stratified-cluster method and derived from an ongoing cohort named ‘Mashhad stroke and heart atherosclerosis disorder’ (MASHAD) study, Mashhad, Iran. The minimum and maximum age of the subjects was 35 and 64 years, respectively. The main inclusion criterion for this study was the absence of a history of a CV event (unstable angina, myocardial infarction and stroke), heart failure, peripheral vascular diseases including transient ischaemic attack or amaurosis fugax, or a history of CV interventions or surgery; however, the presence of traditional CV risk factors including dyslipidaemia, diabetes mellitus and hypertension were not used as exclusion criteria for the study. Individuals with any major co-morbidities such as cancer, autoimmune diseases (e.g. systemic lupus erythematous, rheumatoid arthritis and multiple sclerosis), overt acute or chronic infectious disease, and inflammatory diseases at the time of recruitment were excluded. Each subject gave informed written consent to participate in the study, which was approved by the Mashhad University of Medical Science Ethics Committee.
For all subjects, clinical data were collected from their available records, questionnaires and face-to-face interview. Anthropometric measurements and standard blood pressure assessment were performed as previously described. 4
Biochemical analysis
Plasma and serum were collected following a 12 h fast and stored at −80℃. A fasting blood glucose (FBG) and full lipid profile were measured using enzymatic methods (Pars Azmun, Karaj, Iran). Serum hs-CRP concentration was measured by immunoturbidity with detection limit of 0.06 mg/L (Pars Azmun, Karaj, Iran).
MetS
Both the International Diabetes Federation (IDF) and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III [ATP III]) definitions of MetS were used in our data analysis as previously described. 4 IDF-MetS was defined by the presence of three or more of the following components: fasting plasma glucose ≥6.1 mmol/L; systolic or diastolic blood pressure ≥130 or ≥85 mmHg; high-density lipoprotein cholesterol (HDL-C) < 1.29 mmol/L for females or < 1.03 mmol/L for males; triglyceride ≥1.70 mmol/L and waist circumference ≥80 cm for females or ≥94 cm for males. ATPIII-MetS was defined as being present, when three of the following criteria were met:
Increased waist circumference: >102 cm for males and >90 cm for females; plasma concentration of HDL-C < 1.03 mmol/L for males and < 1.29 mmol/L for females; raised values for plasma triglycerides: ≥1.70 mmol/L; systolic or diastolic blood pressure ≥130 or ≥85 mmHg; FBG ≥6.1 mmol/L.
Statistical analysis
Statistical analysis was performed using SPSS version 23 (SPSS Inc., Chicago, IL, USA). Data were evaluated for normality using the Kolmogorov-Smirnov test. Student t-tests and Mann-Whitney tests were used to compare means or medians of variables with or without normal distribution, respectively. Chi-square tests were used to compare the qualitative variables. Serum hs-CRP concentration distribution was divided into quartiles and patients in the first quartile (lowest concentration of hs-CRP) were considered as a reference group. Nominal regression analysis was used to predict whether serum hs-CRP was related to metabolic and traditional CV risk factors. Odds ratios (ORs) with 95% confidence intervals were obtained using regression analysis.
Results
Demographic and biochemical characteristics of individuals in quartiles of hs-CRP.
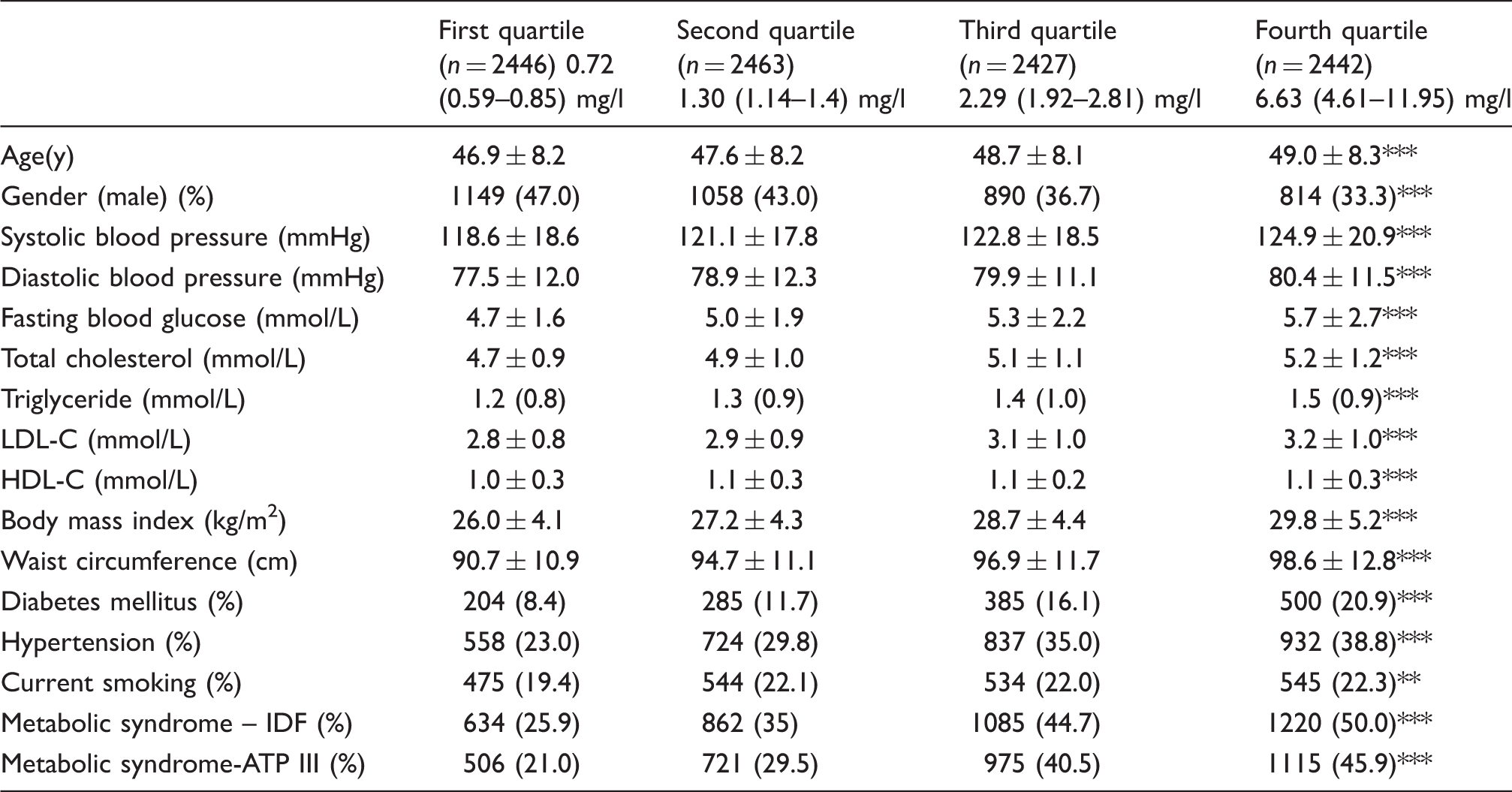
Note: Values expressed as mean ± SD for variables with normal distribution, and median and interquartile range for non-normally distributed data.
HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol.
P < 0.01; **P < 0.05; ***P < 0.001.
In all our univariate and multivariate analyses, the first quartile served as a reference group. Subjects in the fourth quartile were significantly older than those in the first quartile (49.0 ± 8.3 y vs. 46.9 ± 8.2 y; P < 0.0.001, Table 1). Several risk factors, including: blood pressure, lipid profile, body mass index and waist circumference, history of diabetes mellitus, hypertension, and current smoking status, showed increased with quartile (Table 1). The percentage of male participants was significantly lower in the fourth quartile (33.3%) compared with other quartiles, with the first quartile (47.0%) containing the highest % of male subjects (P < 0.001).
The percentage of patients with IDF-MetS in the first, second, third and fourth quartiles were 25.9%, 35.0%, 44.7% and 50.0% respectively (P < 0.001). Moreover, based on ATP-III criteria, the percentage of MetS in each quartile was found to be 21.0%, 29.5%, 40.5% and 45.9%, respectively (P < 0.001).
The relative risk of being within second, third and fourth quartile of hs-CRP associated with risk factors and metabolic syndrome.
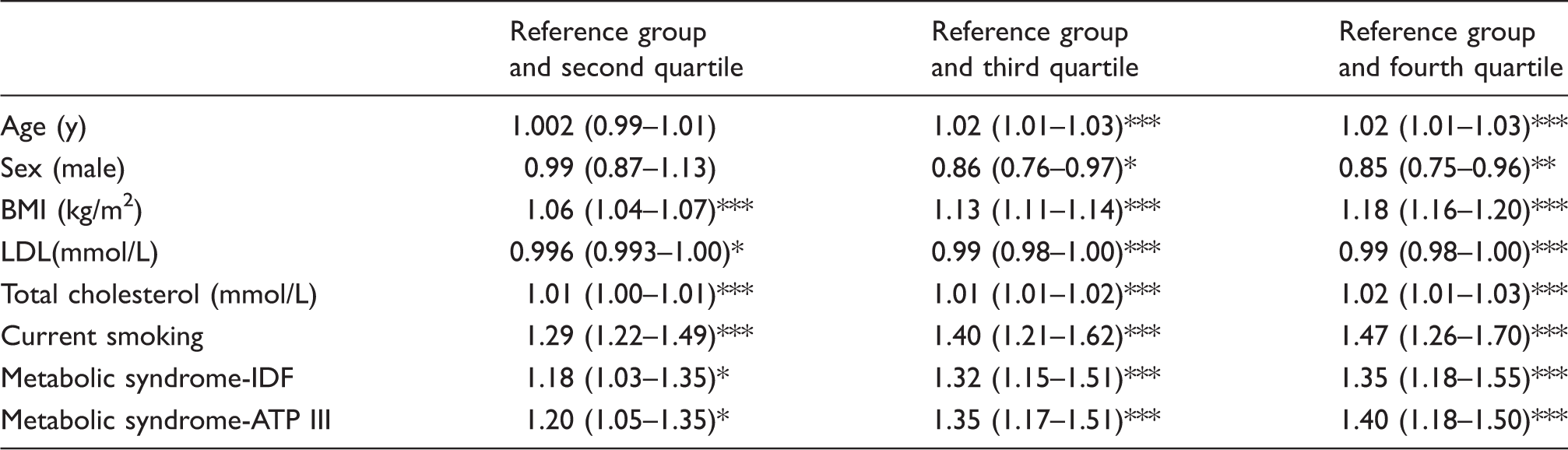
Note: Adjusted odds ratios with 95% confidence intervals (95% CI) obtained from multiple logistic regression tests.
BMI: body mass index.
P < 0.01; **P < 0.05; ***P < 0.001.
Discussion
This was a cross-sectional study with a large sample size of subjects without a history of CVD. We found a significant worsening of several conventional CV risk factors in the individuals within the fourth quartile for serum hs-CRP compared with the subjects within the first quartile. The percentage of subjects with MetS within the fourth quartile was approximately two-fold higher than the reference group. This value was slightly greater using the ATPIII definition of MetS versus the IDF definition. A high serum hs-CRP in the early phases of atherosclerosis is considered to reflect vascular inflammation, and its measurement has been advocated as an adjunct to the assessment of conventional risk factors. 13 The serum hs-CRP concentrations in asymptomatic individuals was particularly high in a proportion of individuals; around 25% of subjects who were in the fourth quartile for serum hs-CRP had serum concentrations that were greater than 11.95 mg/L. Several studies with large sample sizes from both the United States and Europe have demonstrated that serum hs-CRP is useful for the prediction of future CV events among apparently healthy males and females. 10
The association between MetS and elevated concentrations of serum hs-CRP (>3 mg/L) has been shown in non-diabetic Cuban Americans (55 males and 106 females) aged ≥30 years. 14 Serum hs-CRP was also found to be significantly higher in the patients with MetS than in those without among the diabetic patients. 15 A study of 5728 subjects with a similar mean age as that of our study showed that subjects with three, four, or five features of the MetS, had 5.1, 10.7 and 11.1 times greater odds of elevated hs-CRP (>3 mg/L) compared with subjects without any features of the MetS. 16 Our results indicate that elevated concentrations of serum hs-CRP are associated with an increased prevalence of MetS, which is a cluster of known predisposing risk factors to CV events. Our results cannot show whether an increased serum hs-CRP is a cause or consequence of MetS, but highlights the high probability of a concurrent increase in inflammatory status and MetS. According to in vitro studies as well as large sample evidence the association between hyper-inflammation (i.e. defined by increased CRP) and insulin resistance, adiposity and other features of MetS is known to be linked to further elevated risk of CV events. 17
The cut-off values of serum hs-CRP for MetS in our population differed with definition of the MetS and was 1.60 mg/L (IDF-defined sensitivity: 66.3%; specificity: 54.7%) and 1.61 mg/L (ATPIII-defined sensitivity: 67.4%; specificity 53.8%). Due to the wide range of variability of hs-CRP, even in an asymptomatic population, the specificity and sensitivity of the cut-off points are relatively weak.
Overall, the American Heart Association/Centres for Disease Control recognized that individuals with an hs-CRP > 3 mg/L are a high-risk group for CVD. 18 Among our sample population, 29.2% of subjects were found to have hs-CRP > 3 mg/L. It has been reported that 25% of the middle-aged population in the United States has serum concentrations of CRP > 3 mg/L 19 ; this was approximately 18% in a Chinese population. 20 It therefore appears that the percentage of patients with concentrations of hs-CRP above the threshold for increased risk of CVD is high in the Persian population.
We found that females in our population sample had higher concentrations of serum hs-CRP than the males, and this is consistent with previous publications.21,22 The percentage of females increased in each quartile for serum hs-CRP, with the fourth quartile containing approximately 80% females. Whether there is a gender-specific effect of hs-CRP as a risk predictor of CVDs is still subject of debate, although some studies have reported that serum hs-CRP appeared to be considerably stronger marker of CV risk in females compared to males. 23 A strong relationship between serum hs-CRP and development of coronary spasm (an ischaemia-related phenomenon, angiographically defined as a >70% methylergonovine-induced coronary artery spasm reduction in luminal diameter) was found predominantly in females. 24
We found an independent effect of smoking on serum hs-CRP concentrations. The prevalence of current smokers was significantly higher in the fourth quartile of hs-CRP. While the results of previous studies have been conflicting, smoking habit appears to be associated with increased serum hs-CRP.25,26
In conclusion, we found a significant relationship between serum hs-CRP and the presence of MetS and current smoking habit in a large Iranian cohort of subjects without a baseline history of CVD. In this population, serum hs-CRP was particularly high in females. As the MASHAD study is a prospective, longitudinal cohort, there will be opportunity to quantify the predictive value of baseline hs-CRP concentration on CV outcome.
Footnotes
Acknowledgements
The participation of the staff of Cardiovascular Research Center of the Mashhad University of Medical Science is gratefully acknowledged.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research project has been supported by the Mashhad University of Medical Science Research.
Ethical approval
This study was approved by the Mashhad University of Medical Sciences Ethics Committee; Reference number: 84135.
Guarantor
MGM.
Contributorship
SMRKB and MT contributed equally to this work including study design, data management, data analysis and interpretation and writing the drafts of this project; ME, AHB, MM and SRP: were involved in protocol development, gaining ethical approval, data collection and study conduction; HE: statistical advice; GF: data interpretation and revision of the drafts. MGM: Researched literature, conceived the study and mentored all steps of the project. All authors reviewed and edited the manuscript and approved the final version of the manuscript.