
Abstract
Objectives
Glucose is one of the most frequently measured analytes in laboratories. Most recent studies on glucose stabilities confirm that the sodium fluoride/potassium oxalate (NaF/KOx) tube is far from the gold standard. Citrate tubes have been suggested as the preferred tube type by many institutions. Greiner has introduced a glucose-specific tube (Glucomedics) containing NaF/KOx, citrate, and EDTA to minimise glycolysis. The aim was to determine which tube would be the most suitable for accurate glucose estimation in a routine laboratory setting.
Design and methods
The study process involved three experiments: (a) participant comparison using lithium heparin plasma as the comparative sample; (b) stability study (0, 1, 2 and 4 h); and (c) minimal fill volume for the citrate and the Glucomedics tubes.
Results
The patient comparison study of lithium heparin plasma showed that EDTA, NaF/KOx, and both citrate and Glucomedics if corrected for dilutional factors produced acceptable results. The stability study up to 4 h showed that the Glucomedics tube was most effective in preventing clinically significant change in glucose concentration at a room temperature. Both citrate and Glucomedics need to be filled within 0.5 mL of the recommended fill volume for acceptable results.
Conclusion
The Glucomedics tube is the most suitable for minimising glycolysis. Further improvements to it (use of correct dilutional factor and the addition of gel separator) would make this tube the benchmark for the most accurate estimation, best diagnosis and patient care decisions.
Keywords
Introduction
Debate about the suitability of the blood collection tube for the stabilisation of glucose, that is, the ability to prevent glycolysis and so to allow accurate glucose estimation, continues to receive publicity. Current blood collection tubes (lithium heparin, serum or sodium fluoride/potassium oxalate, NaF/KOx) do not immediately prevent clinically significant glycolysis, and thus, glucose consumption continues by the different blood cells (red, white and platelets). Cellular metabolism is exacerbated by prolonged contact with the cells and storage temperature. The so-called gold standard tube NaF/KOx anticoagulant is reported to be ineffective in inhibiting glycolysis as is blood without it, 1 specifically in the first 3–4 h. 2
Studies have shown that both serum and lithium heparin plasma have higher glucose concentrations than NaF/KOx plasma. Gambino 3 showed that serum separator tubes in 61% of the serum samples had greater concentration than the paired plasma samples from NaF/KOx samples, and 11.3% of the serum samples had higher glucose by >0.55 mmol/L. Shi et al. 4 reported that lithium heparin plasma samples gave 0.39 mmol/L higher results compared with NaF/KOx plasma samples. In contrast, a different study using lithium heparin plasma and serum showed no difference in glucose concentration when stored for 30 min at the same temperature. 3
Uchida et al. 5 were the first group to show that acidification of blood, pH 5.3–5.9, was a more effective inhibitor than NaF/KOx. Recently, a number of publications have advocated the use of citrate plasma as the sample of choice.1,6 This has led to several European countries (Finland, Sweden, Denmark and Poland) as well as different health facilities in other countries introducing citrate as the sample of choice rather than NaF/KOx. 6 The most recent guidelines by the American Diabetes Association and the American Association of Clinical Chemists recommend that lithium heparin plasma samples should be stored on ice slurry and plasma should be separated within 30 min or tubes with citrate buffer should be used. 7 Some have advocated the use of a combined anticoagulant tube (NaF/KOx, EDTA and citrate) as the tube of choice.1,8
Inaccurate glucose estimations lead to errors in the diagnosis/classification, treatment and assessment of the risk of developing diabetes. Furthermore, it also introduces noise in epidemiological data. 2
Greiner have recently introduced a specific blood collection tube Glucomedics for glucose estimation, which contains a combination of anticoagulants, NaF, EDTA and citrate (Greiner Bio-one, Kremsmuster, Austria). The aim of this study was to determine which tube would be the most suitable for accurate glucose estimation in a routine laboratory under the same conditions.
Materials and methods
The evaluation was in three parts: patient comparison study, stability study and dilution effect study.
For the patient comparison study, in total 42 healthy adult participants were recruited with consent which was approved by the Princess Alexandra Hospital ethics committee. The samples were collected in the following Greiner Vacutainer tubes (#catalogue number): Lithium heparin – #456083; EDTA – # 454023; NaF/KOx – #454061; Serum – #456071; Citrate – #454327; and Glucomedics – #454347 (Greiner Bio-one, Kremsmunster, Austria). The order of draw was citrate, serum, lithium heparin, EDTA, NaF/KOx and Glucomedics. The samples were collected by a phlebotomist and centrifuged at 3000 g for 10 min at 20℃. The serum was allowed to clot for 30 min before centrifugation. All anticoagulated tubes were processed in <30 min and the serum tubes were processed in <45 min from collection to aliquoting of the plasma or serum. Post centrifugation, the plasma or serum samples were then immediately transferred into a clean aliquot tube to prevent further cell contact. The aliquot tubes were stored at a room temperature until analysed. All the aliquots were analysed in triplicate on one analyser, and for each participant, different samples were analysed at the same time. No out-of-control diabetic participants were recruited, as the most significant effect on glucose is at around the diagnostically important cut-off values. 2
The analysis was performed on a Beckman DxC800 analyser (glucose oxidase method; Beckman Coulter, Brea, CA, USA). The glucose method coefficient of variations (CVs) of the two internal controls are level 1 – mean 4.55 mmol/L, %CV 2.54% and level 2 – mean 15.6 mmol/L, %CV 1.36%. The CV of the lower level control was used to determine if results from the different blood collection tubes were considered outside the analytical error (>2.5%) and if so were considered to be due to glycolysis. Lithium heparin plasma was used as the reference sample as recommended,7,9 but with the exception that lithium heparin tubes were not placed in ice slurry.
For various reasons, blood tubes vary in the time taken to be centrifuged, and hence, it is essential that glucose stability should be established under normal laboratory conditions. For the stability study, samples were collected from two volunteers in different tubes. The uncentrifuged tubes set from the two volunteers were allowed to stand for 1, 2 and 4 h. These times were selected based on local data where it is rare to have samples sit unanalysed for >4 h even from our external referral healthcare facilities. This was to observe the degree of change at each storage time mimicking the time taken for arrival of samples and processing before being analysed. The samples were processed and analysed in triplicate as outlined in the participant comparison study.
Blood tubes often arrive without being filled to the recommended fill mark or volume. The citrate and Glucomedics tubes are the only tubes used for glucose estimation that contain liquid anticoagulant which if underfilled can lead to a dilutional effect. It is important to determine acceptable fill volumes for the citrate or Glucomedics tubes which will not be always filled to the recommended fill volume of 3.5 and 2.0 mL, respectively. Samples were collected from two volunteers into the citrate and Glucomedics tubes and filled to different volumes. The samples were processed and analysed in triplicate as outlined in the participant comparison study.
Statistical analysis was performed using the Microsoft Excel and Analyse-It statistical add-on for Microsoft Excel (Analyse-It, Leeds, UK). The patient-specimen comparisons were assessed by Passing Bablok Regression correlation equations versus lithium heparin plasma samples.
Results
Patient comparison study
Results of the participant (n = 42 healthy adults) comparison study in the different Greiner tubes.
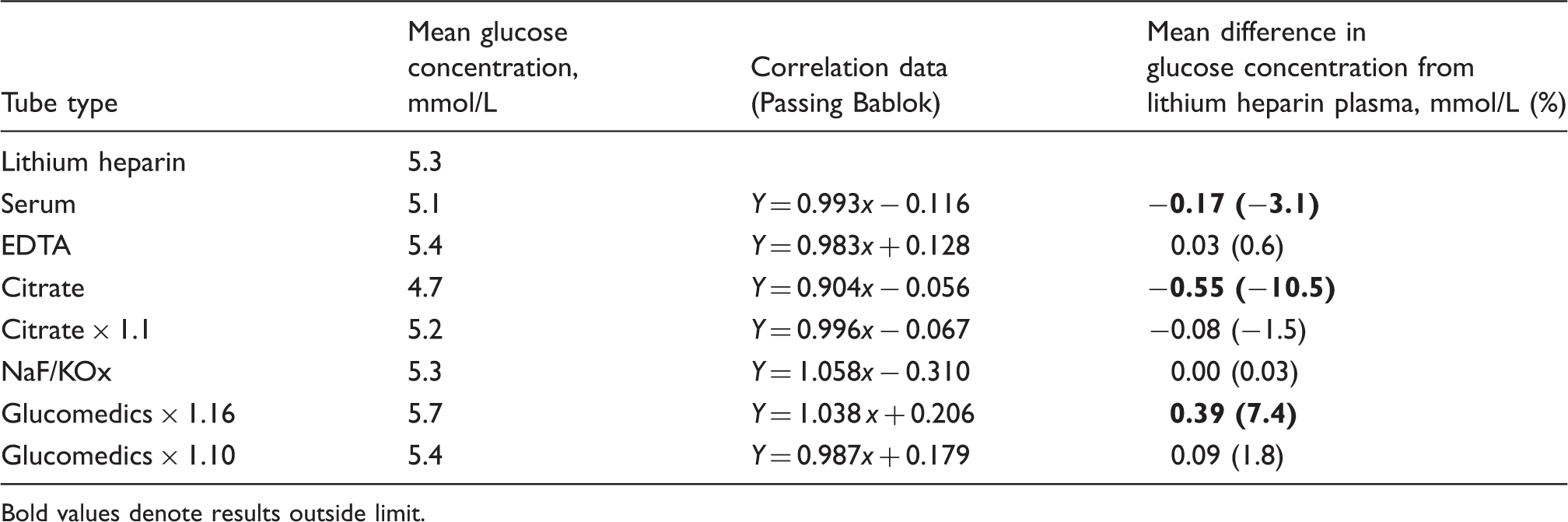
Bold values denote results outside limit.
Stability study
Stability of glucose in the various Greiner tubes when stored at RT for 1, 2 and 4 h before centrifugation.
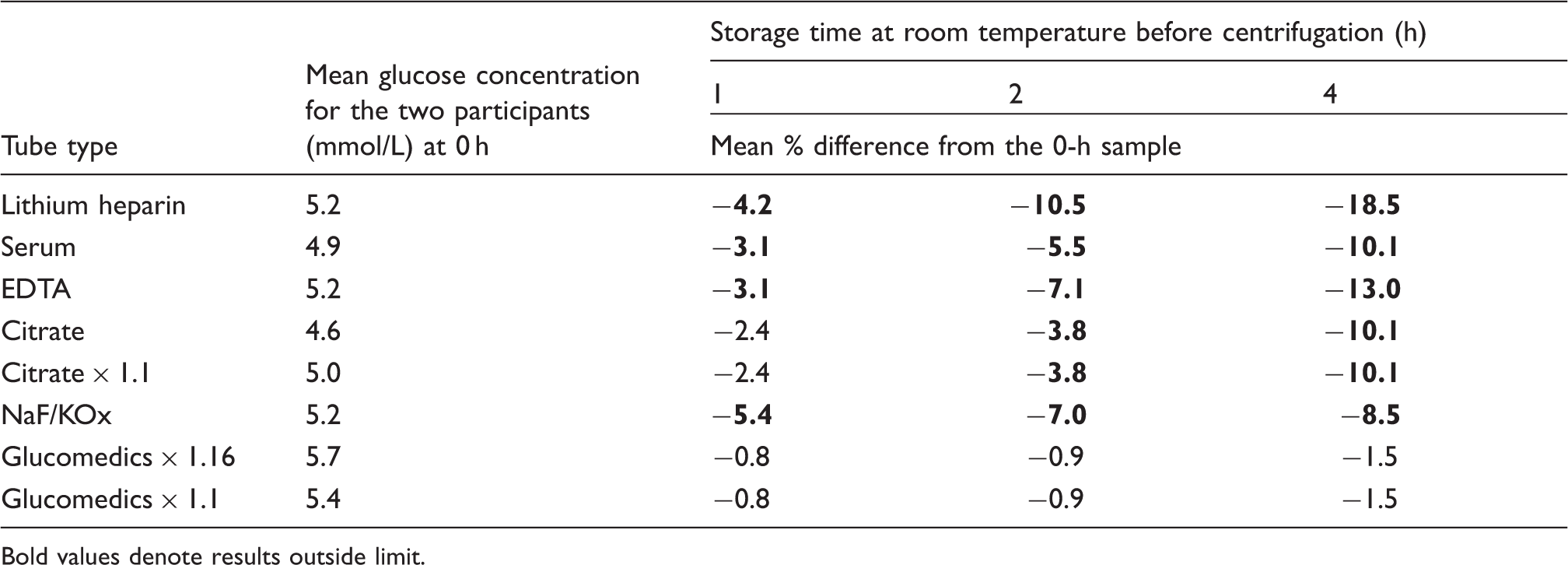
Bold values denote results outside limit.
Effect on glucose estimation from differing volume fill in citrate and Glucomedics tubes study
Effect of fill volume on the accuracy of glucose estimation due to dilutional effect.
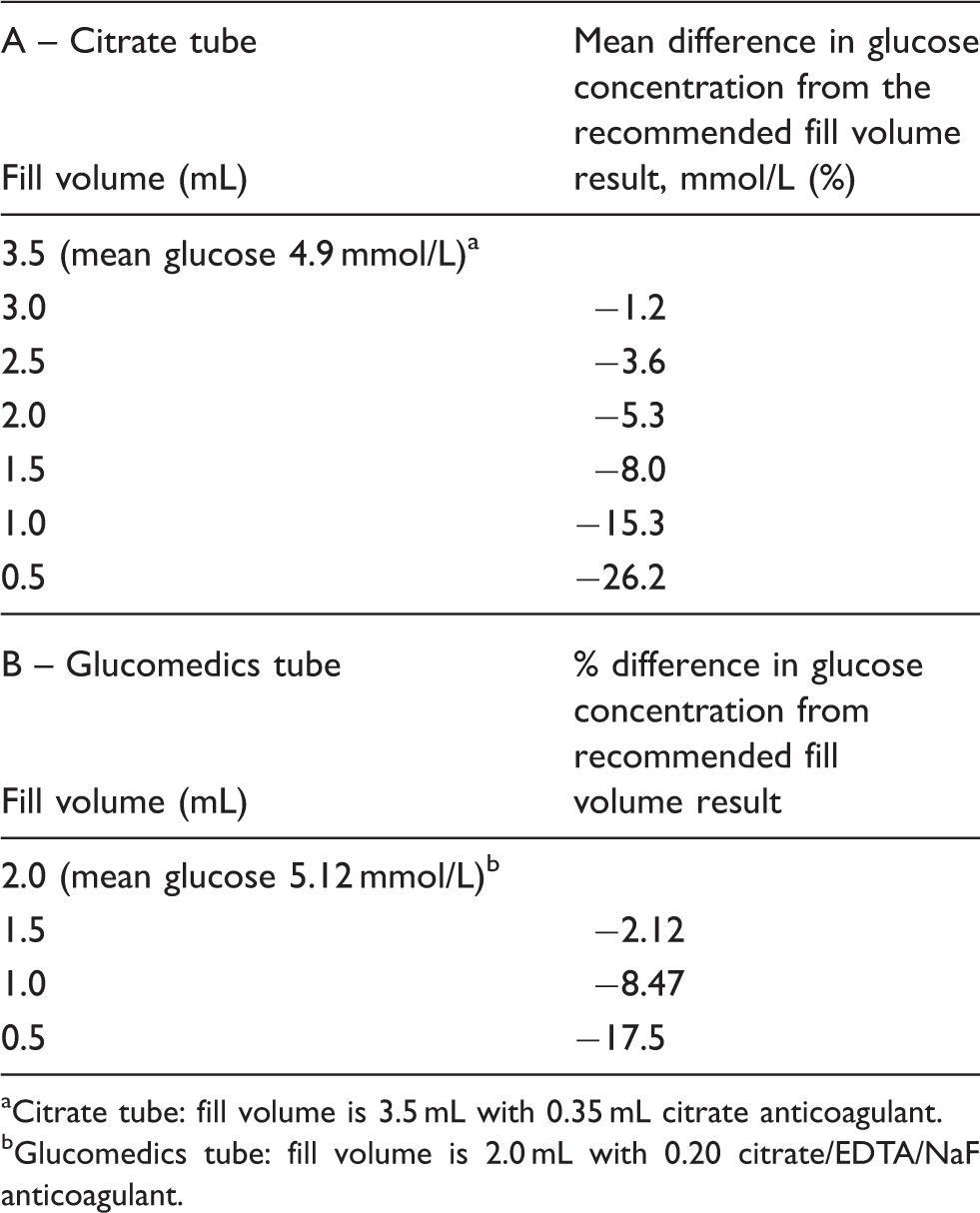
Citrate tube: fill volume is 3.5 mL with 0.35 mL citrate anticoagulant.
Glucomedics tube: fill volume is 2.0 mL with 0.20 citrate/EDTA/NaF anticoagulant.
Discussion
This study provides useful data on the most suitable tube/inhibitor of glycolysis. The results convincingly showed that the Glucomedics tube produces comparative glucose results to lithium heparin plasma in normal participants, provided the multiplication factor of 1.16 as recommended by Greiner is adjusted to reflect the dilutional ratio between anticoagulant volume and final fill volume, a factor of 1.10. In this study, lithium heparin tubes were not placed on ice post collection as recommended but were processed at a room temperature for <30 min, and therefore, there is a potential of some in vitro reduction in plasma glucose. Anecdotally, this factor would also make it much easier to manually and rapidly calculate the final glucose concentration. It is not indicated in Greiner information on how the recommended multiplication factor of 1.16 was derived. One minor problem that needs consideration is the implementation of this multiplication factor for results, and this may be accommodated on analysers or by laboratory information systems.
Citrate alone was the next best agent to limit glycolysis. Similarly, a correction is required for the anticoagulant volume to final fill volume to improve correlation. This fact has not been examined by the different publications nor has it been taken into consideration when studying its suitability to date, even though the tube has been implemented as the tube of choice by countries and individual health institutions.6,7
Serum data showed that the recommended clotting time of 30 min was sufficient to lead to significant changes and prolonged contact with cells caused glucose consumption. This simply indicates that under normal laboratory processing conditions, the standard serum tubes are not suitable for accurate glucose estimation. Gambino et al. 1 found that heparin plasma glucose was 0.9% higher than serum when stored under same conditions which they attribute to the clotting processes consuming glucose. Yet our results shower higher difference, 3.1%.
One point that needs further attention is that serum is the sample of choice for most biochemical analysis in laboratories across the world. The new Rapid Serum Tube from BD which only requires 5 min clotting time showed that glucose results were much closer to lithium heparin plasma, only slightly lower, −1.05% versus the standard BD serum tube which showed a mean difference of −2.26%. 10 Fernandez et al. 11 stated that their study confirmed that collection in serum tubes yielded clinically equivalent results to NaF/KOx plasma under certain set of conditions. Both the EDTA and NaF/KOx tubes showed a significant decrease in glucose concentration (>2.5%) confirming they are ineffective in preventing clinically significant glycolysis even within 60 min of cellular contact. Similarly, Frank et al. 12 reported that glucose in EDTA plasma post 8-h storage showed greater decrease than serum or NaF/KOx plasma.
The stability data demonstrated that Glucomedics tube was the most effective in minimising glycolysis up to 4 h. The next best tube was citrate whereas the NaF/KOx, EDTA, serum and lithium heparin tubes exceeded the analytical error limit even at 1-h storage. What was interesting was the serum produced less change than NaF/KOx plasma in the first 2 h of storage compared with the zero time collection.
In the real world, a lot of samples in most laboratories are not processed and analysed within 1 h of collection, yet serum and lithium heparin are almost always used for routine monitoring of glucose concentration and subsequent patient management decisions. For example, in our tertiary level hospital, the mean turn-around-time for the whole facility is ∼100 min which is amongst the shortest in our organisation of 33 hospital-based laboratories. Gambino et al. found that glucose decreased in NaF/KOx tubes (BD tubes) by 4.5% at 2 h, whereas our data (Greiner tubes) showed a more significant decrease, 7% which could be influenced by storage and centrifugation temperature.
Gel separators provide a physical barrier between serum or lithium heparin plasma to prevent glycolysis by the cells which make them more robust for handling, transport and storage to maintain highest sample integrity in terms of cellular influence. Thus, consideration should be given by Greiner to re-engineer the Glucomedics tube, incorporate gel separator to provide the cleanest sample. Even though the World Health Organisation recommends lithium heparin as the reference sample,7,9 it has to be noted lithium heparin plasma samples in gel separator tubes are not free from cellular aggregates post centrifugation. 13 Such cellular aggregates would lead to decrease in glucose concentration when lithium heparin plasma is stored for prolonged periods, especially at higher temperatures. Further proof of this is provided by Li et al. 14 who found that the heparin plasma results after two days were significantly lower than serum and NaF/KOx, and it is estimated the glucose in heparin decreased at ∼0.3 mmol/L per day. However, they also report that at 4 h, the glucose concentration in serum and heparin compared with NaF/KOx tubes was statistically insignificant from one another. 14 Our results showed that serum and NaKOx were very similar at 4 h (10.1 and 8.5% decrease, respectively) whereas at the same time point the lithium heparin plasma had significantly higher decrease (18.5%) in glucose concentration.
Terumo produce similar tube (Venosafe® Glycaemia) which contains NaF, EDTA and citrate buffer that is available in Europe which was evaluated by Gambino et al. 1 , and this study reported that this speciality tube after 2 h showed a decrease of 0.3% and 1.2% after 24 h at 37℃ and in comparison glucose decreased by 4.5% after 2 h and 7% after 24 h at 37℃ in the NaF/KOx tube. 1
In summary, the combination of the different anticoagulants in the Glucomedics tube has a major advantage in preserving the glucose compared with serum, heparin, EDTA, NaF/KOx or citrate tubes alone. It is very obvious that the loss of glucose prevention will lead to patients being more accurately diagnosed and managed in timely manner which can lead to benefits, reduce risks for the patient and health care system; and equally lead to confidence in the results over prolonged periods of storage before analysis is completed. The tube needs to be filled within 0.5 mL of the recommended fill volume which may not always achievable. Finally, it is suggested that the tube be re-engineered with a gel barrier to will provide the cleanest and most stable plasma sample.
Footnotes
Acknowledgements
Greiner provided the Glucomedics tubes but had no input in any aspect of the study.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Princess Alexandra Hospital ethics committee (HREC Approval: 2009/011).
Guarantor
GD.
Contributorship
GD is the major contributor and coordinator of the project from design to final manuscript. The original idea was discussed with KSY and finalised in cooperation with NNB. The final manuscript was collaborative effort by the three authors.