
Abstract
Background:
Acute kidney injury (AKI) is frequently under-recognized and contributes to poor outcomes. Electronic alerts (e-alerts) to highlight AKI based on changes in serum creatinine may facilitate earlier recognition and treatment, and sophisticated algorithms for AKI detection have been proposed or implemented elsewhere. However, many laboratories currently lack the resources or capability to replicate these systems.
Methods:
A real-time automated delta check e-alert flags a 50% increase in creatinine to a concentration of >50 µmol/L from the most recent result within a 90-day period and automatically adds the comment ‘?AKI – creatinine increase >50% from previous’ with a link to local AKI guidelines. In addition, creatinine results >300 µmol/L are retrospectively reviewed and phoned if AKI is suspected. For each alert over a 12-day period we manually reviewed previous and subsequent creatinine results to determine baseline creatinine and stage AKI according to Acute Kidney Injury Network (AKIN) criteria.
Results:
From 11,930 creatinine requests, 63 of 90 (70%) delta check e-alerts were due to AKI, identifying 61 episodes of AKI. Thirty four of 54 (63%) creatinine results >300 µmol/L were due to AKI, identifying a further 10 episodes of AKI. The positive predictive value (PPV) for AKI of a delta check e-alert was greater when the trigger creatinine was >100 µmol/L (PPV 89%) or when the absolute change in creatinine was >50 µmol/L (PPV 93%).
Conclusion:
This study demonstrates that a simple automated delta check can detect and flag AKI in real time, continuously, at little extra cost and without manual input.
Introduction
Acute kidney injury (AKI) is a sudden decline in renal function, generally occurring over hours or days. AKI is increasingly recognized as a common and serious complication of many hospital admissions and is associated with poor outcomes such as increased mortality, 1 chronic kidney disease (CKD) progression, 2 prolonged hospital stay and increased healthcare costs. 3 Furthermore, there is evidence that AKI is frequently under-recognized; delays in recognizing and treating AKI were a major criticism in a 2009 National Confidential Enquiry into Patient Outcomes and Death report into the care of patients who died with a primary diagnosis of AKI. 4
Electronic alerts (e-alerts) to highlight possible AKI to the requesting clinician or renal team based on changes in serum creatinine are one strategy to facilitate earlier recognition and treatment of AKI. This approach has been backed by a 2012 UK Consensus Conference on AKI management hosted by the Royal College of Physicians of Edinburgh 5 as well as recent National Institute for Health and Care Excellence (NICE) guidelines on AKI. 6 This has prompted discussions between laboratory IT manufacturers, renal physicians and clinical biochemists to define IT requirements for AKI e-alert systems and develop an algorithm for generating e-alerts based on changes in serum creatinine with time. 7
Although sophisticated e-alert systems for AKI have been reported, 8 they involve manual input and sophisticated adaptation of laboratory IT systems. A National Health Service (NHS) Kidney Care survey in early 2012 suggested that more than half of NHS trusts do not have and are not planning on implementing e-alert systems. 9 Barriers to the use of e-alerts included IT issues, increased workload for the biochemistry department and cost.
We describe a simple automated delta check e-alert that can be easily implemented by laboratory staff on most modern laboratory IT systems, does not require manual input by biochemistry staff and is associated with minimal running costs for the laboratory.
Methods
e-alert
A real-time automated delta check in CliniSys WinPath (CliniSys, Chertsey, UK) flags a 50% increase in creatinine from the most recent result within a 90-day period provided that the creatinine concentration is also >50 µmol/L. The comment ‘?AKI – creatinine increase >50% from previous’ with a link to the London Acute Kidney Injury Network website (www.londonaki.net) is automatically added to results that fail the delta check. Delta check e-alerts with trigger creatinine >100 µmol/L or from patients <18 years result in the reflex addition of an ‘Acute Kidney Injury Flag’ dummy test to increase the prominence of the alert within electronic records and are phoned to the requesting clinician as part of normal laboratory procedures for phoning critical results. A list of all delta check AKI e-alerts from inpatients at University College Hospital is emailed to intensive treatment unit (ITU) outreach twice a day via an automated scheduled query of the pathology data repository. This email contains patient demographics, location and previous creatinine results. In addition, all creatinine results >300 µmol/L are retrospectively reviewed twice daily by the duty biochemist and phoned if AKI is suspected. The e-alert includes all patients served by the laboratory – inpatients, outpatients and primary care; no samples are excluded based on patient location.
Study design
We reviewed all alerts over a 12-day period. For each patient, we collected all creatinine results analysed at the laboratory at University College London Hospitals NHS Foundation Trust (UCLH) from 300 days before to 120 days after the first e-alert or creatinine result >300 µmol/L. Creatinine results were manually reviewed independently by both authors together with information from the patient’s electronic record to determine baseline creatinine and stage AKI according to Acute Kidney Injury Network (AKIN) criteria 10 (using the peak creatinine for each episode of AKI). Where possible, we categorized each patient’s baseline estimated glomerular filtration rate (eGFR) as >60 mL/min/1.73 m2 or <60 mL/min/1.73 m2, and determined whether creatinine values returned to within 20% of baseline following an episode of AKI. Initial disagreements were resolved after discussion. For patient mortality, we combined patients identified by either the delta check or a creatinine concentration >300 µmol/L. Mortality data were taken from the hospital electronic patient record.
Setting
UCLH is an 846 bed NHS trust providing acute and specialist services from several sites in central London. Services include accident and emergency, cancer care (including University College Hospital Macmillan Cancer Centre), cardiac care (including the Heart Hospital), critical care, endocrinology, general surgery, general medicine and urology. UCLH does not provide specialist renal services. The laboratory at UCLH also serves general practice in the London boroughs of Camden, Islington and Westminster.
Creatinine assay
The laboratory offers two methods for creatinine using the Roche Cobas modular analyser series (Roche Diagnostics, Burgess Hill, UK). A rate blanked, compensated Jaffe method is used for the vast majority of samples (>96%). An enzymatic method is reserved for samples from patients <1 year old and in samples from patients of any age where the icteric index falls between predefined limits. Both methods are traceable to isotope dilution mass spectrometry. The delta check e-alert uses only Jaffe creatinine results. Throughout the manuscript, unless specifically otherwise stated, ‘creatinine requests’ or ‘creatinine results’ refer only to requests or results for creatinine analysis using the Jaffe method.
Results
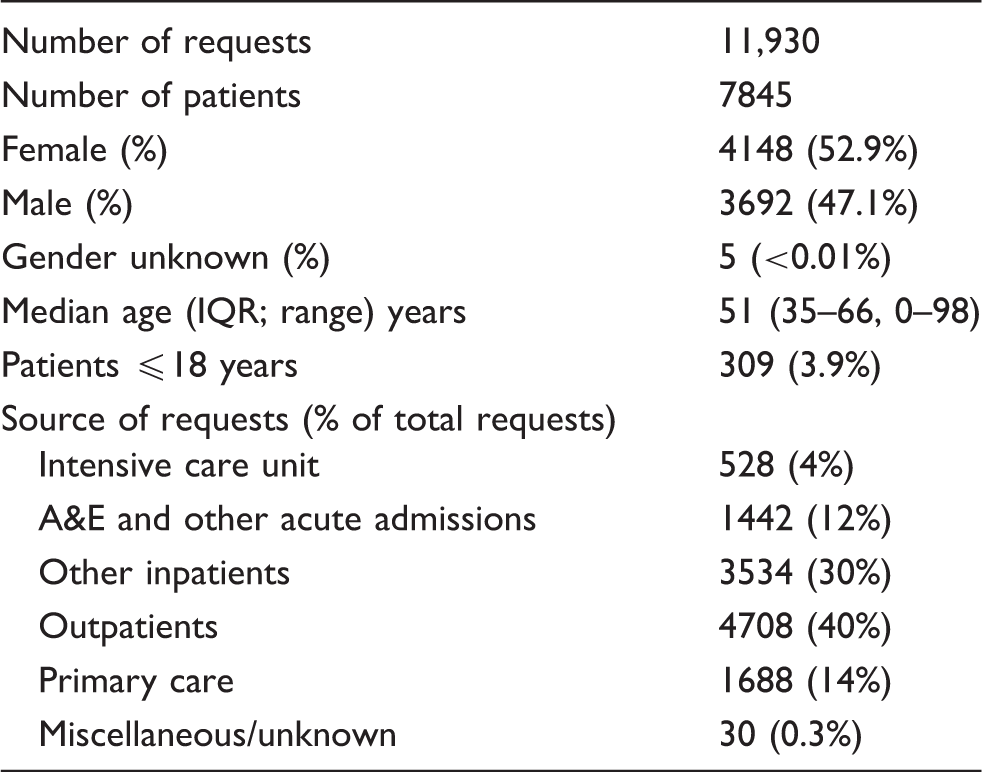
Requests for creatinine analysis using the Jaffe method.
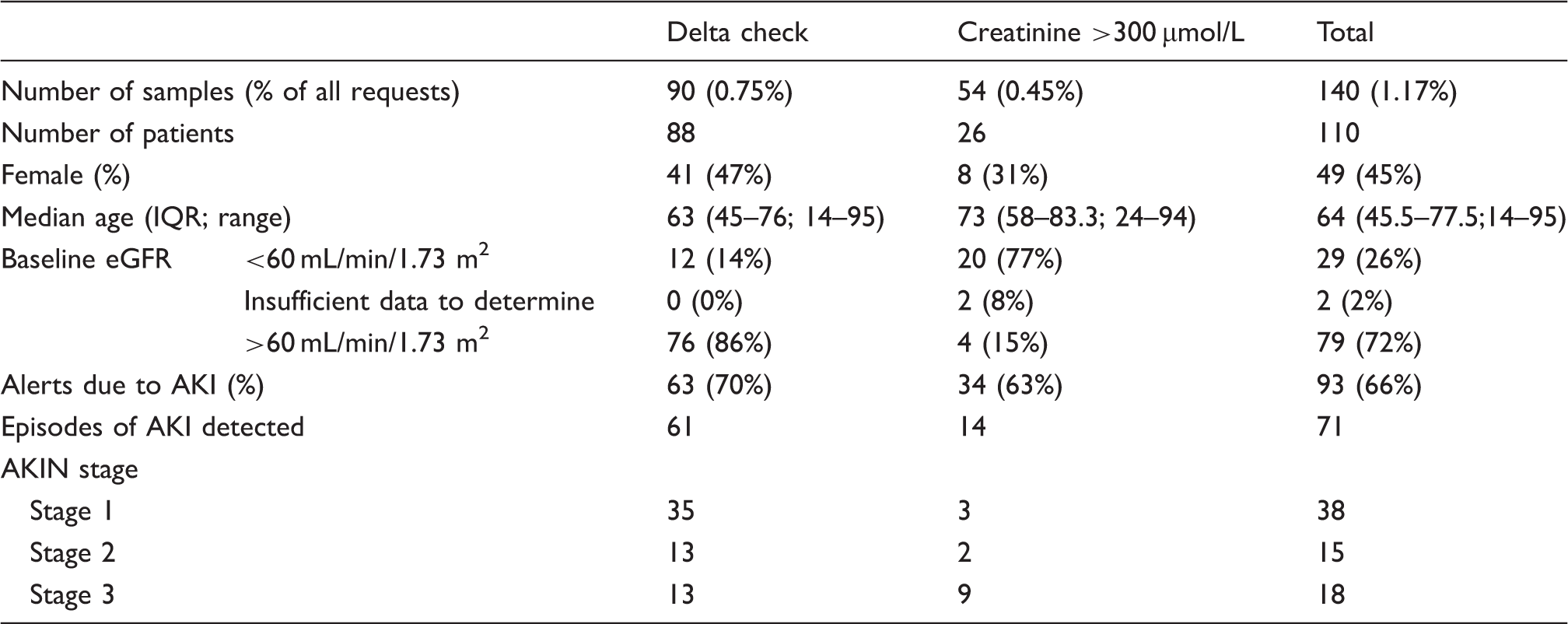
Delta check e-alerts and creatinine results >300 µmol/L. Four samples (from four different patients) triggered a delta check e-alert with a creatinine >300 µmol/L and so are included in both categories.
There was a median (interquartile range (IQR); range) of 10 (3–21.8; 0–176) creatinine results in the 300 days before and 6 (2–12.8; 0–79) in the 120 days after the first delta check e-alert or creatinine result >300 µmol/L for each patient. In total, each patient had a median (IQR; range) of 21.5 (9–36; 2–244) creatinine results in the period from 300 days before to 120 days after their first delta check e-alert or creatinine result >300 µmol/L.
There was initial agreement on AKI stage (not AKI, stage 1, stage 2, stage 3) between the two reviewers in 137/144 (95%) of delta check e-alerts and creatinine results >300 µmol/L. All cases of disagreement were resolved after discussion.
Of the delta check e-alerts, 63/90 (70%) were due to AKI, identifying 61 episodes of AKI, of which the majority were AKIN stage 1. Thirty four of 54 (63%) creatinine results >300 µmol/L were due to AKI, identifying 14 episodes of AKI, of which the majority were AKIN stage 3. In total, we identified 71 episodes of AKI; 38 stage 1 (53%), 15 stage 2 (21%) and 18 stage 3 (25%).
Variation of AKI classification with patient characteristics
Of 88 patients with a delta check e-alert, eight (9%) were from ITU, 24 (27%) from accident and emergency (A&E) or acute admissions unit (AAU), 32 (36%) from other inpatients, 20 (23%) from outpatients and four (5%) from primary care (Figure 1). Of the 26 patients with a creatinine result >300 µmol/L, four (15%) were from ITU, seven (27%) from A&E or AAU, five (19%) from other inpatients, eight (30%) from outpatients and two (8%) from primary care (Figure 1).
Source of delta check e-alerts. (a) Delta check e-alerts, (b) creatinine >300 µmol/L. A&E: accident and emergency; AAU: acute admissions unit; ITU: Intensive treatment unit.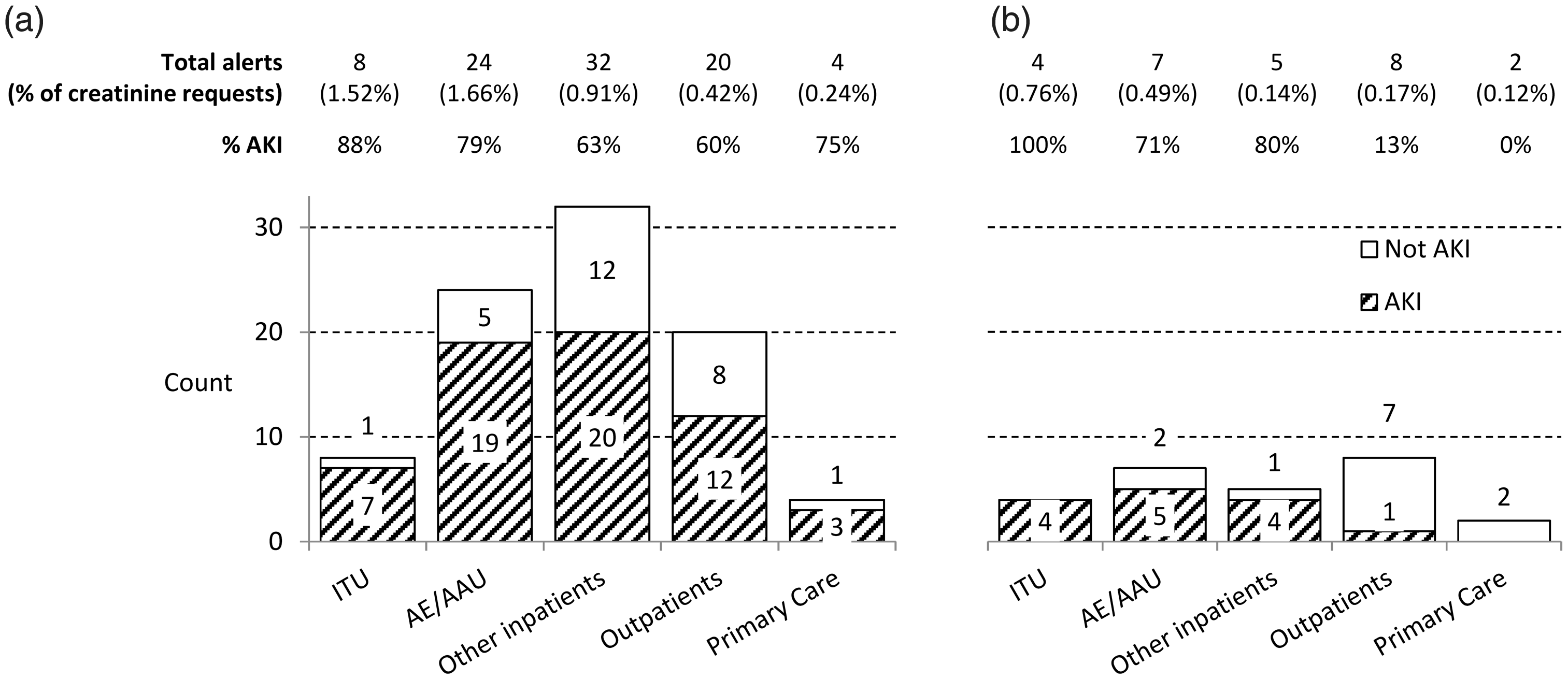
The delta check predominantly detected AKI in patients with baseline eGFR >60 mL/min/1.73 m2; in the 61 cases of AKI detected by the delta check, 53 (87%) had eGFR >60 mL/min/1.73 m2 (Figure 2). Creatinine results >300 µmol/L detected acute on chronic kidney injury, severe AKI in patients with normal renal function and CKD without AKI (Figure 2).
AKIN stage classified by alert type and baseline eGFR. (a) Delta check e-alerts, (b) patients with creatinine >300 µmol/L.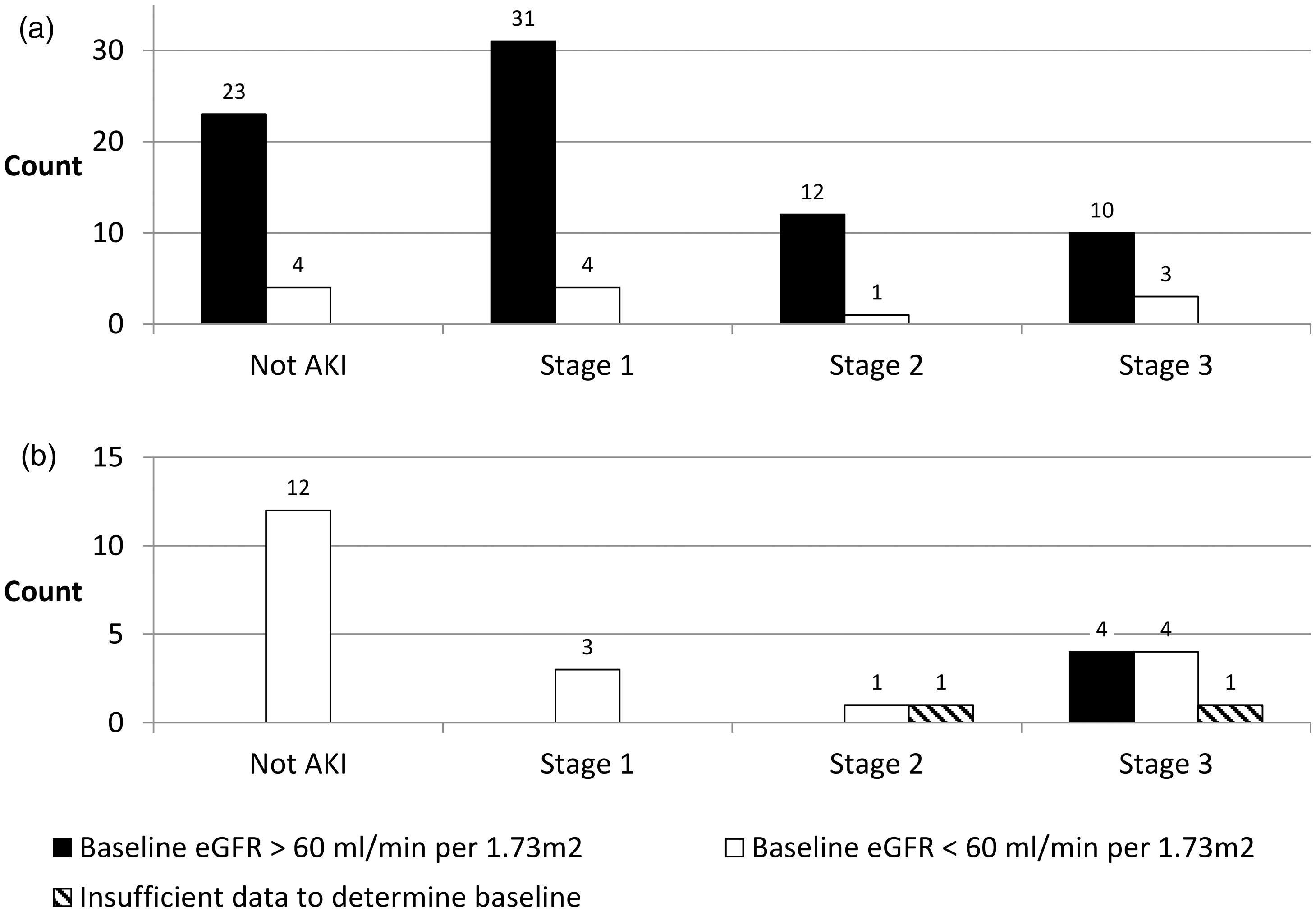
Variation of AKI classification with delta check characteristics
The median (IQR; range) trigger creatinine was 120 µmol/L (78–152; 51–752). The positive predictive value (PPV) of the delta check e-alerts was greater when the trigger creatinine was >100 µmol/L (PPV 89%) compared to e-alerts with trigger creatinine between 50 and 100 µmol/L (PPV 42%) (P < 0.01, chi-squared test). During a separate 12-day period, we removed the need for creatinine to rise to a concentration of >50 µmol/L, however there were no convincing cases of AKI amongst 20 e-alerts with trigger creatinine <50 µmol/L.
The median absolute creatinine increase (IQR; range) was 47 µmol/L (36–71; 18–666) at a median (IQR; range) of 9.3 days from the previous result (1.2–37 days; 0–77 days). The PPV of the delta check e-alerts was greater when the absolute change in creatinine was >50 µmol/L (PPV 93%) compared to e-alerts with Δ creatinine <50 µmol/L (PPV 52%) (P < 0.01, chi-squared test).
There was no obvious useful relationship between the specificity of the e-alert and either the time from previous result (Figure 3(c)) or relative change in creatinine (Figure 3(d))
Variation of AKI classification with (a) trigger creatinine concentration, (b) absolute change in creatinine, (c) time from previous result and (d) relative change in creatinine.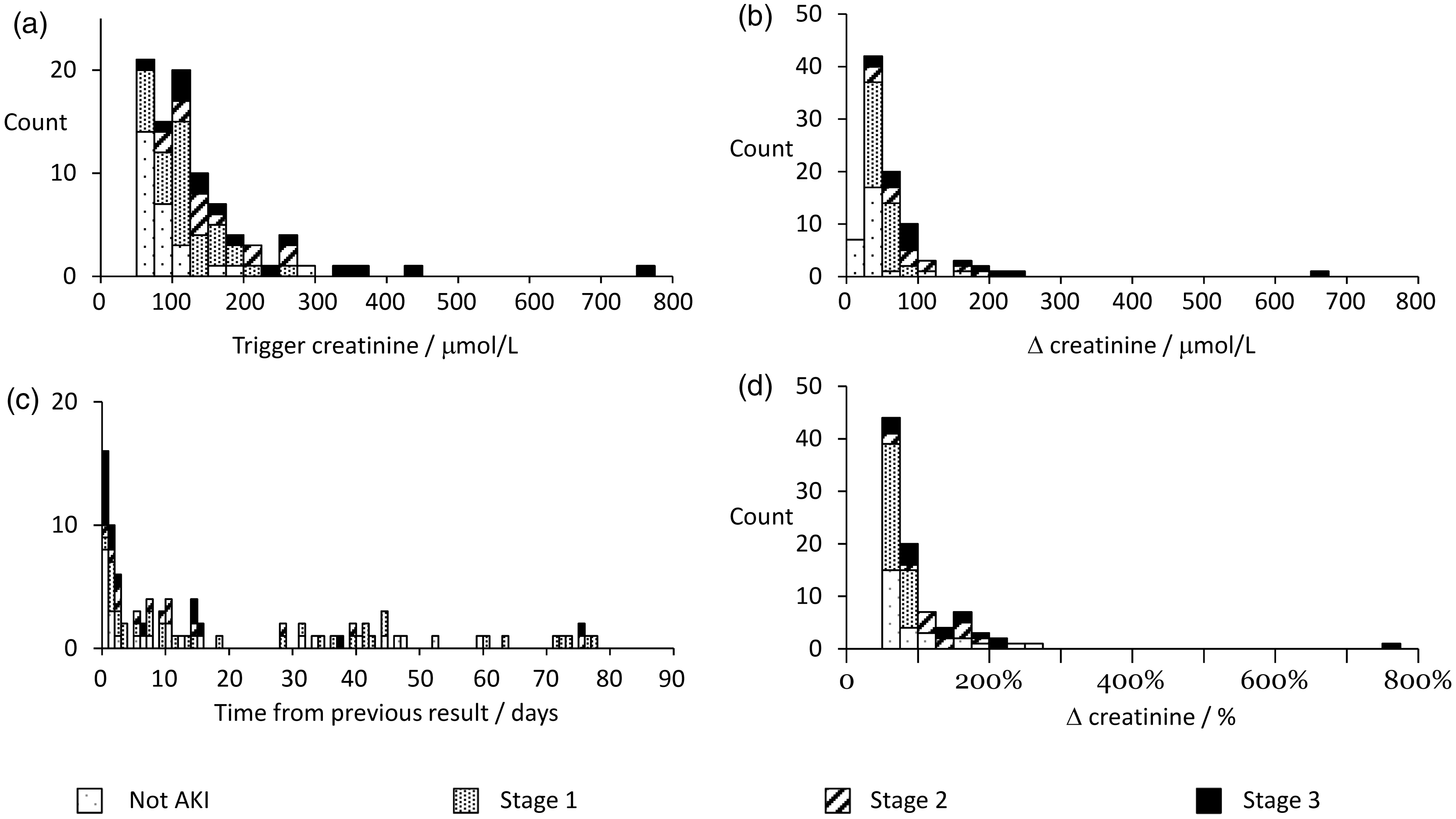
Patient outcomes
Seven-day mortality after the first e-alert or creatinine result >300 µmol/L for each patient was 0/39 (0%) in patients with false positive alerts, 1/38 (3%) in AKI stage 1, 3/15 (20%) in AKI stage 2 and 5/18 (28%) in AKI stage 3. After 120 days, mortality was 3/39 (8%) in patients with false positive alerts, 4/38 (11%) in AKI stage 1, 4/15 (27%) in AKI stage 2 and 9/18 (50%) in AKI stage 3. One hundred and twenty day mortality was slightly higher amongst patients with AKI identified by a creatinine result >300 µmol/L (5/14, 36%) compared to patients with AKI identified by the delta check (14/61, 23%). Of the 54 patients with AKI who survived to 120 days, 43 (80%) recovered their baseline renal function (serum creatinine within 20% of baseline) and four (7%) did not; seven (13%) had insufficient data to assess recovery of renal function.
Discussion
This study demonstrates that a simple, automated delta-check e-alert can detect and flag AKI in real time, 24 h a day, 365 days a year, at little extra cost, without any human input and using existing laboratory software. As delta checks are a simple feature of many laboratory information management systems, this is a system most laboratories could easily replicate.
On average, the delta check e-alert identified approximately five episodes of AKI every day. By reviewing creatinine results >300 µmol/L we were able to detect approximately one further case of AKI per day.
As with all screening techniques, the AKI e-alert system does not have 100% specificity or sensitivity. We acknowledge that there are likely to be missed cases of AKI. This could occur if there are no previous creatinine results within a 90-day period or if successive creatinine increases are <50% of the previous value. Although some of these cases are detected if creatinine rises above 300 µmol/L, some may be missed completely. However, our aim was not to detect systematically all cases of AKI, but rather to highlight gross changes in creatinine in patients for whom there is a high likelihood of an acute decline in renal function; the e-alert should be seen as an adjunct, not a replacement, for timely review of laboratory results.
Similarly, 27 of 90 (30%) delta check e-alerts with a trigger creatinine >50 µmol/L were not due to AKI, representing approximately 0.2% of all creatinine requests. We do not claim that every alert will be a true case of AKI, and ask only for the requesting clinician to consider AKI. In most cases, a simple review of previous results should be sufficient to determine that these alerts are false positives. Although it is desirable to minimize false alerts to prevent ‘alert fatigue’, we believe that for such a simple system, the false positive rate is tolerable.
Other AKI e-alert systems have been reported, for example, a hospital-wide system relying on manual determination of baseline creatinine in patients where creatinine is >50% greater than an ‘ideal’ creatinine. 8 This ‘ideal’ value is reverse calculated from the modified diet in renal disease equation assuming a GFR of 75 mL/min/1.73 m2. This system has been validated with a low false positive (1.7%) and false negative rate (0.2%) and is likely to be a valuable resource for prospective data collection of AKI incidence and outcomes. However, this system has not been widely adopted elsewhere, perhaps due to the human and IT resources required.
Instead, many have opted for systems relying on automated estimation of baseline creatinine, for example, when the current serum creatinine is >75% greater than the last recorded value. 11 Despite the known difficulties in automatically estimating baseline creatinine, not all hospitals have validated their automated e-alert systems against manual review. Some automated e-alert systems define baseline as the lowest creatinine within a predefined period; however, nadir creatinine has been shown to be a poor estimation method with high potential for AKI misclassification. 12 This is in agreement with our experiences. It was not unusual to see an occasional low creatinine result, with the subsequent creatinine result triggering a false positive delta check. If baseline had been defined as the nadir creatinine, this would result in multiple false positive AKI e-alerts, reducing the accuracy of the system. We therefore advise against using nadir creatinine for baseline estimation in automated e-alert systems.
Other systems rely on strict application of AKI definitions (either RIFLE (Risk Injury Failure Loss End-stage renal disease), AKIN or KDIGO (Kidney Disease: Improving Global Outcomes)). For our automated delta check, we applied only the 50% increase present in all three criteria, but not the 26 µmol/L increase present in AKIN and KDIGO definitions. This was due to the inability of our software to apply more than one delta check forcing a choice between delta checking for a 50% or a 26 µmol/L increase. Due to concerns of overdiagnosis and that a 26 µmol/L increase in creatinine would not be unusual in patients without any real acute change in renal function, particularly those with CKD in whom such changes are not independently associated with mortality, 13 we opted to use the 50% criterion.
Owing to software limitations we could not automate the staging of AKI based on the change in creatinine. A study comparing different automated strategies (ideally utilizing both relative and absolute creatinine changes and different definitions of baseline) against manual review would be valuable to determine optimal automated AKI detection.
The characteristics of different hospitals and laboratories are likely to affect the sensitivity and specificity of this delta check e-alert. Detection of AKI in children may be delayed or missed by specifying that creatinine must rise to >50 µmol/L. However, patients less than 18 years old accounted for less than 5% of Jaffe creatinine requests, and are perhaps more likely to receive closer monitoring, reducing the need for the AKI e-alert. Nevertheless, it may be prudent to review this cut off if applying the delta check to populations with a higher proportion of paediatric patients. Similarly, UCLH does not provide specialist renal services; in such hospitals, the specificity of creatinine results >300 µmol/L for the detection of AKI is likely to be reduced, but most laboratory systems can exclude specific locations such as renal units.
We detected a surprisingly high number of episodes of AKI in outpatients. University College Hospital Macmillan Cancer Centre, which provides outpatient and day care cancer services, accounted for about half of these cases. AKI is a common complication in cancer patients, 14 due to a variety of factors including the use of nephrotoxic drugs, obstruction of renal or post-renal structures by the tumour mass, cast nephropathy and tumour lysis syndrome.
The e-alert covers all patients served by the laboratory, not just over several hospital sites, but also patients in primary care; over the 12-day study period, the delta-check identified three episodes of AKI in patients presenting to their general practitioner.
We observed high mortality in patients with AKI, which increased with increasing AKI stage. This is as expected from previous studies 1 and validates that our e-alert identifies a population at higher risk of death. A minority of patients who survived the episode of AKI did not recover their baseline renal function after 120 days follow up.
In this study we demonstrate that a simple e-alert system can be used to highlight cases of AKI; we have not shown that this has any effect on clinician behaviour or patient outcomes, which is the ultimate goal. There have been a small number of studies looking to investigate the effect of AKI e-alerts.
A real-time alert of worsening AKI stage through a text message sent to the clinician’s telephone was found to increase the number of early therapeutic interventions in an ICU in Belgium. 15 There was also an increase in the proportion of patients who recovered their renal function within 8 h after an alert indicating less severe AKI, but not amongst those with more severe AKI. There was no significant effect on renal replacement therapy, ICU length of stay, mortality, maximum creatinine or maximum AKI stage. Importantly, nine out of 10 AKI alerts were based on urine volume criteria, so the applicability of these findings to creatinine based e-alerts is questionable.
Hospitals that have already implemented AKI e-alerts have noted improved outcomes following their introduction. For example, a hospital wide e-alert system based on changes in serum creatinine at the Royal Derby Hospital led to a progressive reduction in 30-day mortality over consecutive 6-month periods (23.7, 20.8, 20.8, 19.5%, chi-square for trend p = 0.006). 16 This improvement in survival was maintained after adjustment for age, co-morbid conditions, severity of AKI, elective/non-elective admission and baseline renal function. However, the e-alert was introduced as part of a range of educational interventions so it is difficult to determine the contribution made by the e-alert component. Further studies are therefore needed to demonstrate the effect of AKI e-alerts on measurable patient outcomes.
In this study, we validated a simple delta check e-alert for the detection of AKI. We advise that hospitals validate their automated AKI e-alert systems against manual review to ensure that they correctly identify a high-risk population.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not required.
Guarantor
AD.
Contributorship
NF analysed the data and wrote the first draft of the manuscript. Both authors contributed to study design, reviewed and edited the manuscript and approved the final version of the manuscript.