
Abstract
Background
Neutrophil gelatinase-associated lipocalin (NGAL) is emerging as a new biomarker for the early identification of acute kidney injury (AKI). There is also increasing evidence of an association between urinary albumin/creatinine ratio (ACR) and AKI. The primary aim of this study was to evaluate the clinical utility of these biomarkers to predict AKI in a population of perioperative patients treated with goal-directed haemodynamic therapy (GDHT). Secondary aims were to examine NGAL and ACR as sensitive biomarkers to detect the effects of GDHT and to investigate the association of these biomarkers with secondary outcomes.
Methods
Urine was obtained from 109 patients admitted to a critical care unit following major abdominal surgery. Patients were treated with intravenous fluid, GDHT with intravenous fluid or GDHT with intravenous fluid and dopexamine. Urine was collected preoperatively, and at times 0, 8 and 24 h postoperatively and outcome monitored for 28 days.
Results
There were no significant differences in NGAL or ACR concentrations between the cohorts treated with GDHT compared to standard care. However, both biomarker concentrations rose significantly in all cohorts over the time points. There were no significant differences in NGAL observed between patients who developed AKI and those who did not. However, there were significantly higher ACR preoperatively in patients who developed AKI. There were higher NGAL concentrations in patients who developed an infection and who died.
Conclusions
NGAL has a poor predictive role in evaluating AKI in this clinical setting. Preoperative ACR may have a role as an AKI marker.
Introduction
Complications, including acute kidney injury (AKI), following major surgery are an important cause of death and disability. 1 Currently, the diagnosis of AKI is made by a rise in serum creatinine concentration or a fall in urine output.2,3 Despite attempts to standardize the definition of AKI, serum creatinine remains at the core of these definitions but is known to be a delayed and unreliable marker of AKI. The pursuit of improved biomarkers of AKI is an area of intense contemporary research.
Using genomic and protein microarray technology, a series of molecules have been identified as potential markers for AKI; among them neutrophil gelatinase-associated lipocalin (NGAL).4–6 Several studies have demonstrated that NGAL is significantly elevated in patients with AKI but not in the corresponding controls.7–9 However, recent evidence indicates NGAL can also be raised in other pathological conditions such as certain tumours and cardiovascular disease. 10 In addition, NGAL requires complete evaluation in different clinical settings but evidence so far suggests that it is a promising biomarker in AKI.
Urinary albumin/creatinine ratio (ACR) is an established marker for the detection of glomerular proteinuria in the diagnosis and management of chronic kidney disease (CKD). 11 Albuminuria may serve as a marker of AKI. Several recent studies have shown an association of either pre- or postoperative albuminuria with a higher incidence of AKI.12,13 Its potential utility as a biomarker of AKI has not been systematically examined. Compared with other novel markers proposed for AKI, it is inexpensive and readily available.
The technique known as goal-directed haemodynamic therapy (GDHT) appears to improve outcome following high-risk surgery.14–19 GDHT describes the use of intravenous fluid and inotropic agents to increase cardiac output and related haemodynamic parameters to predetermined levels. An important difference between GDHT and conventional postoperative care is the use of vasoactive agents. The use of vasoactive drugs as part of GDHT has been shown to be associated with decreased AKI.20,21 Dopexamine is of particular interest, because it has been associated with improved survival. 22
The primary aim of this study was to evaluate the clinical utility of NGAL and ACR to predict AKI in a population of perioperative patients treated with GDHT. This is a further analysis of a previously published trial, which demonstrated improvements in tissue perfusion and oxygenation associated with GDHT. 23 Secondary aims were to examine NGAL’s superiority as a sensitive biomarker when compared with ACR to detect the effects of GDHT. In addition, the association of NGAL and ACR with clinical outcomes such as infection and mortality were also investigated.
Methods
Patient population
Urine samples from a previously published study were used. 23 The study cohort consisted of 135 patients admitted to a critical care unit following major abdominal surgery at Barts and the London NHS Trust. Exclusion criteria included refusal of consent, concurrent lithium therapy, acute myocardial ischemia, acute arrhythmias, pregnancy, patients receiving palliative treatment only and weight less than 40 kg. The study was approved by the London Multicentre Research Ethics Committee and Medicines and Healthcare products Regulatory Agency (UK). Written informed consent was obtained from all patients prior to enrolment in the study.
Clinical management
Full details of this study have been published previously. 23 In brief, following surgery, all patients were managed in a critical care area and received standardized care to maintain arterial oxygenation > 94%, haemoglobin > 8 g/dL, temperature at 37℃ and heart rate less than 100 beats per minute. Participants were randomized to one of three groups by computer-generated random sequences. In the control arm, patients received 250 mL fluid challenges with colloid solution (Gelofusine, BBraun, Melsungen, Germany), as required, to achieve a sustained rise in central venous pressure (CVP). In the two treatment arms, similar fluid challenges were used to achieve a sustained rise in stroke volume (SV). In one of the treatment arms, patients also received dopexamine infused at a fixed rate of 0.5 μg kg−1 min−1. Clinical staff took all other patient management decisions.
Urine was collected from each catheterized patient at four different time points: preoperatively, and at times 0, 8 and 24 h following surgery.
NGAL and ACR analysis
Urine was aliquoted and stored at −70℃ until the day of analysis. Urinary NGAL was analysed on the Abbott (Abbott Park, IL, USA) ARCHITECT i1000sr system. The ARCHITECT urine NGAL assay utilizes a noncompetitive immunometric sandwich format with chemiluminescent signal detection. The assay is reported to have a measurement interval of 10–1500 ng/mL. Within- and between-series imprecision at 20 ng/mL was 1.4% and 4.4%, respectively. Within- and between-series imprecision at 1200 ng/mL was 1.4% and 2.2%, respectively. Urinary creatinine and albumin were analysed by the Jaffe rate reaction and immunoturbidimetry, respectively, on a Beckman Coulter (Beckman Coulter Inc, Brea, CA, USA) DxC800 system. Urinary NGAL was expressed in mass as nanogram/millilitre (ng/mL) and not microgram/litre (µg/L), as traceability back to a SI definition is not possible as there is no recognized reference material. 24 NGAL was also normalized to urinary creatinine as the neutrophil gelatinase-associated lipocalin/creatinine ratio (NCR) (ng/µmol). ACR was expressed as albumin:creatinine (mg/mmol).
Outcome measures
The primary outcome was the development of AKI using creatinine changes as defined using the Acute Kidney Injury Network (AKIN) criteria. 25 Secondary outcomes were the development of infection and mortality within 28 days post surgery. Postoperative infection was defined as follows: if the patients developed any of the following, pneumonia, deep wound infection and urinary tract infection.
Statistical analysis
All statistical analyses were performed using GraphPad prism software version 5.03 (GraphPad Software Inc, La Jolla, CA, USA). The Kolmogorov–Smirnov test was performed to assess for normality. All the continuous variables were determined to display non-Gaussian distribution, therefore nonparametric analysis was performed. Data were graphically presented as median and interquartile range. A value of P < 0.05 was considered significant. Differences in NGAL, NCR and ACR concentrations within and between the CV, SVP and SVP + dopexamine groups were assessed by Kruskal–Wallis one-way analysis of variance. The Mann–Whitney test was used to assess differences between NGAL, NCR and ACR concentrations in patients who developed AKI, development of a postoperative infection and mortality with their controls. Receiver operating characteristic (ROC) analysis was performed to assess the area under the curve (AUC) to determine diagnostic utility of NGAL, NCR and ACR to predict AKI, postoperative infection and mortality using the patients in each group who were free of that complication as controls.
Results
GDHT patient characteristics
GDHT patient characteristics.
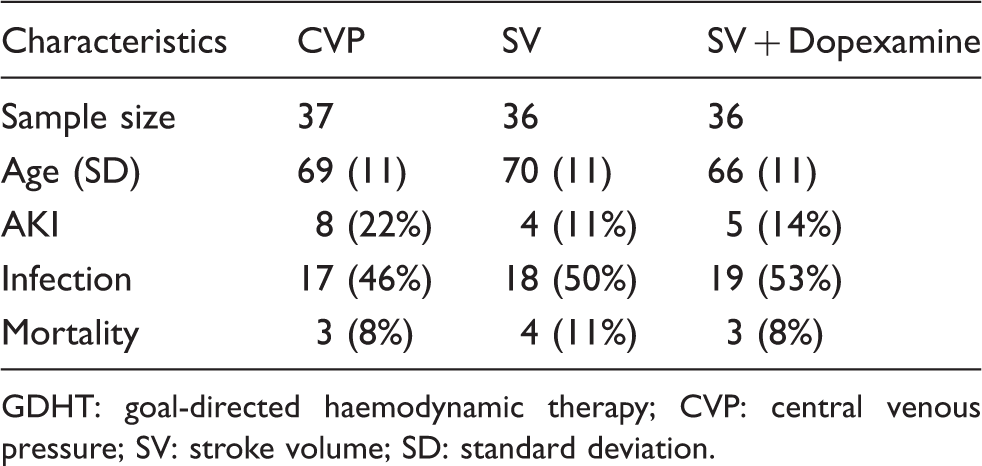
GDHT: goal-directed haemodynamic therapy; CVP: central venous pressure; SV: stroke volume; SD: standard deviation.
NGAL, NCR, ACR and GDHT
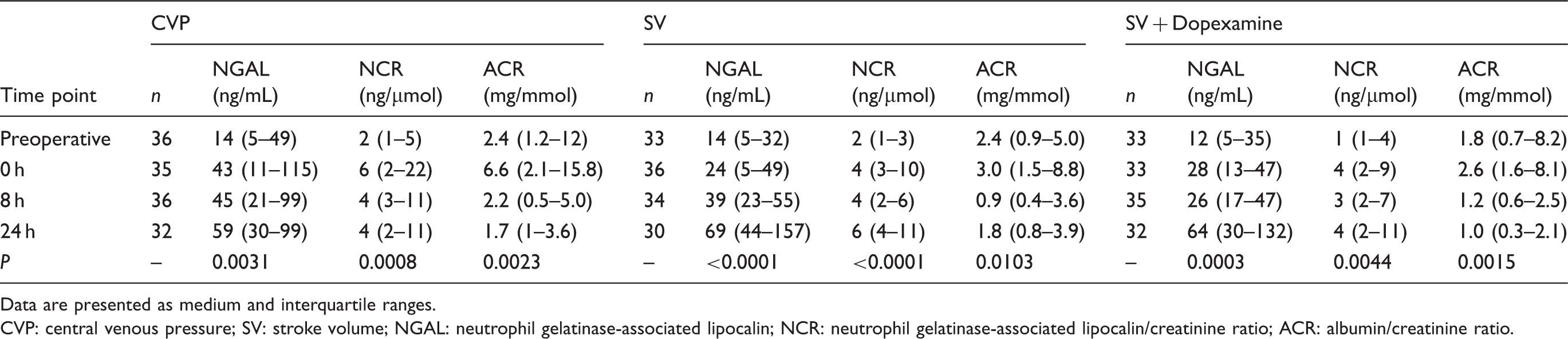
There were no significant differences in NGAL, NCR or ACR concentrations between the three treatment groups at the four time points investigated. However, there were statistically significant differences in NGAL, NCR and ACR concentrations in each of the three treatment groups over the four time points (Figure 1). Refer to Table 2 for a full descriptive table of the median, measure of spread and P values for each of the variables.
Concentrations of NGAL, NCR and ACR in the three treatment groups across the four time points. *P < 0.05, **P < 0.01, ***P < 0.001. Descritptive data for NGAL, NCR and ACR concentrations in the three treatment groups across the four time points. Data are presented as medium and interquartile ranges. CVP: central venous pressure; SV: stroke volume; NGAL: neutrophil gelatinase-associated lipocalin; NCR: neutrophil gelatinase-associated lipocalin/creatinine ratio; ACR: albumin/creatinine ratio.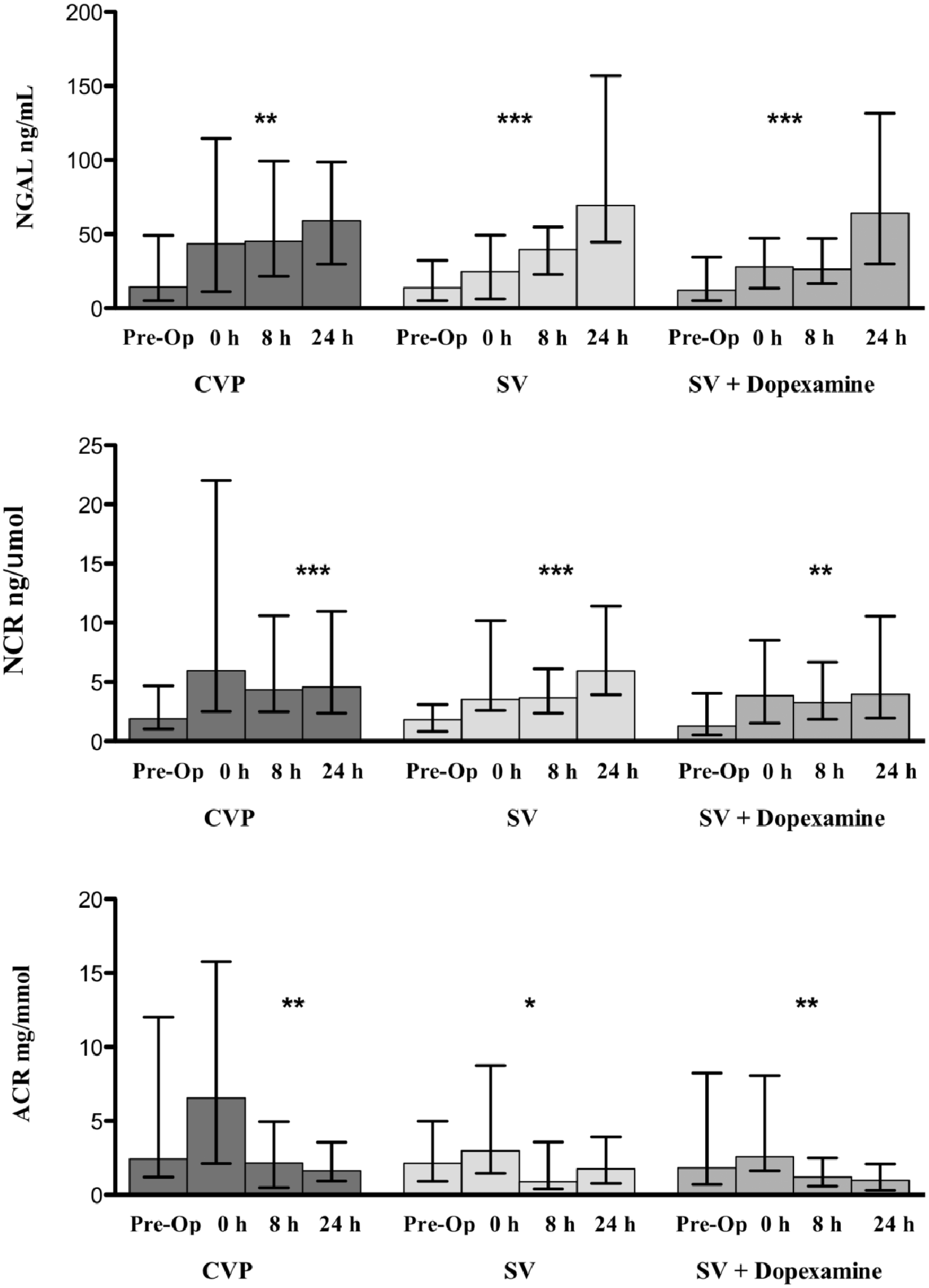
Relationship between NGAL, NCR, ACR concentrations and clinical outcome
There were no significant differences in NGAL concentrations between patients who developed AKI and those who did not for any of the four time points. In addition, there were no significant differences in the NGAL changing ratio from baseline (preoperative) to 8 or 24 h between patients who developed AKI and those who did not. However, there were statistically higher concentrations of ACR preoperatively in patients who developed AKI (P = 0.0034) (n = 16, median 4.62 mg/mmol, interquartile range 2.42–14.55 mg/mmol) compared with patients who did not develop AKI (n = 86, median 1.83 mg/mmol, interquartile range 0.89–5.78 mg/mmol).
There were significantly higher concentrations of NGAL at 24 h following surgery in patients who developed a postoperative infection (P = 0.0263) (n = 49, median 80 ng/mL, interquartile range 39–159 ng/mL) compared to patients did not develop a postoperative infection (n = 45, median 55 ng/mL, interquartile range 28–88 ng/mL).
There were significantly higher concentrations of NGAL at 8 h following surgery in patients who died (P = 0.0289) (n = 9, median 56 ng/mL, interquartile range 38–151 ng/mL) compared to patients who survived (n = 96, median 33 ng/mL, interquartile range 18–55 ng/mL). Also, there were significantly higher concentrations of NGAL at 24 h following surgery in patients who died (P = 0.0280) (n = 9, median 135 ng/mL, interquartile range 64–224 ng/mL) compared to patients who survived (n = 85, median 63 ng/mL, interquartile range 30–101 ng/mL) at 24 h.
There were significantly higher concentrations of NCR preoperatively in patients who died (P = 0.0270) (n = 9, median 5 ng/µmol, interquartile range 2–46 ng/µmol) compared to patients who survived (n = 93, median 2 ng/µmol, interquartile range 1–4 ng/µmol). Also, there were significantly higher concentrations of NCR at 24 h following surgery in patients who died (P = 0.0289) (n = 9, median 12 ng/µmol, interquartile range 5–22 ng/µmol) compared to patients who survived (n = 85, median 4 ng/µmol, interquartile range 2–10 ng/µmol).
Diagnostic accuracy of NGAL, NCR and ACR
Diagnostic performance of NGAL, NCR at various times to predict AKI, postinfection and mortality in patients who developed those complications compared to those who did not.
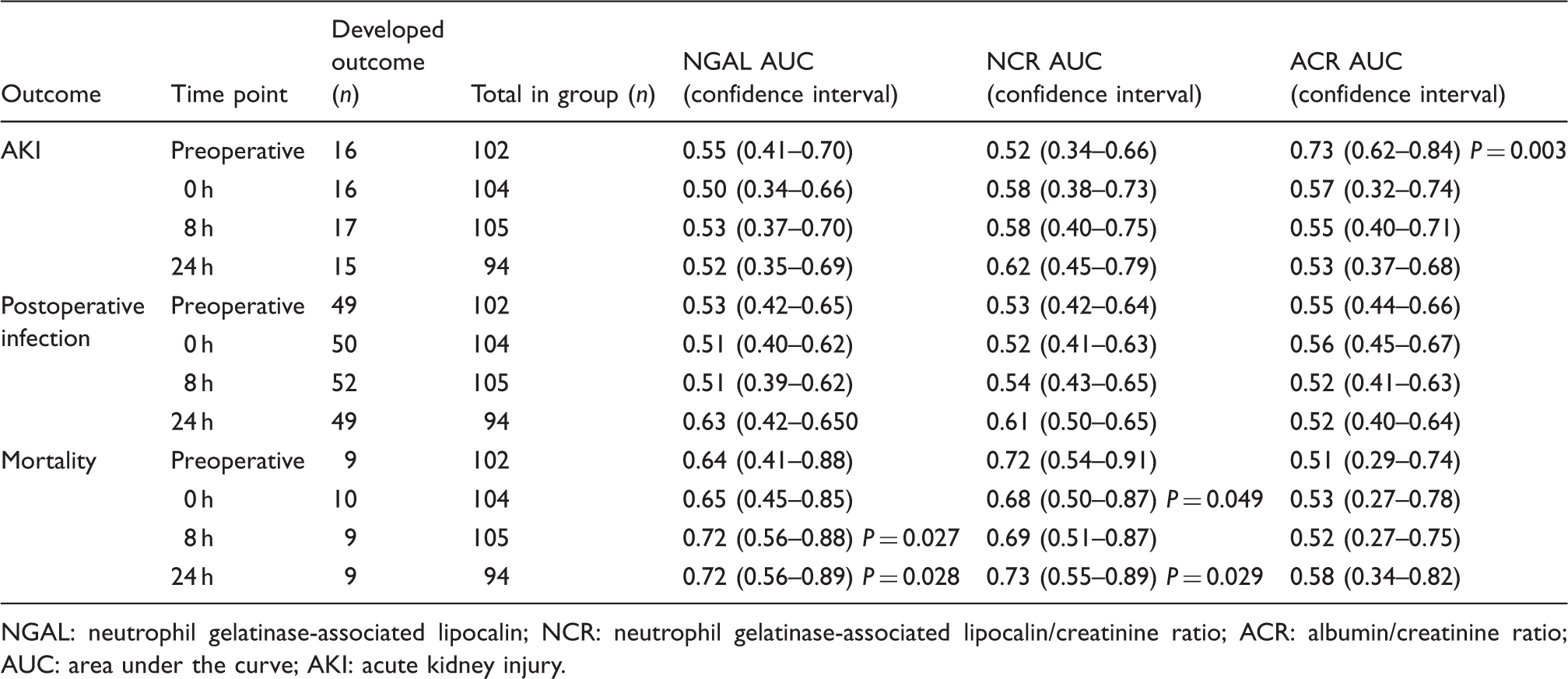
NGAL: neutrophil gelatinase-associated lipocalin; NCR: neutrophil gelatinase-associated lipocalin/creatinine ratio; ACR: albumin/creatinine ratio; AUC: area under the curve; AKI: acute kidney injury.
Discussion
This is the first study to investigate the clinical utility of NGAL and ACR to predict AKI in a cohort of patients treated using GDHT after major abdominal surgery. Our principal finding is that we did not find any association between NGAL in the first 24 h after major surgery and the development of AKI in this cohort. However, preoperative ACR was significantly higher in patients who developed AKI. In addition, there were no significant differences in NGAL or ACR concentrations across the groups. However, both NGAL and ACR concentrations rose significantly in all groups over time. Our study found higher NGAL concentrations in patients who developed an infectious complication and in those who did not survive.
Our findings are consistent with a recent study that found no association between NGAL and AKI but found an association with mortality and infection in a cohort of patients undergoing a wide spectrum of major surgical procedures. 26 Although our results reached statistical significance, our findings will need to be validated in a larger cohort of patients, including those undergoing other surgical procedures. In this study, we found NGAL rose significantly following surgery in all groups. Whether this is caused by direct kidney injury or due to generalized inflammation is unclear. We found preoperative ACR was associated with AKI. Proteinuria ultimately leads to tubular inflammation and fibrosis and patients are less able to tolerate kidney haemodynamic changes and nephrotoxic insults. Several recent studies have examined proteinuria and AKI. However, there is conflicting evidence whether pre- or postoperative concentrations of proteinuria may serve as the optimum time point.12,13,27–29 Huang et al. 27 found that preoperative proteinuria within two days before surgery is highly predictive of postoperative AKI and concluded it was irrespective of acute or chronic insults. Larger studies are needed to establish the clinical utility of ACR as a marker of AKI.
A limitation is the fact that it is a single-centre retrospective analysis of a prospective study with small numbers of patients with AKI, which did not facilitate performing a power calculation to confirm the predictive value of urinary NGAL for AKI. In addition, we were unable to demonstrate clinical utility for the use of the NGAL changing ratio from baseline, which has been proposed recently to improve the clinical utility of NGAL in AKI. In our study, we used the preoperative NGAL as a baseline, so that each patient acted as his or her own control. Initial studies on NGAL demonstrated it had a high predictive role in AKI but most of these were either performed using cardiac surgery patients or after excluding patients with comorbidities. NGAL is raised in other conditions such as cardiovascular disease, CKD, diabetes and malignancy.30,31 This could suggest that NGAL performs best in situations where patients with conditions that impact on kidney function are excluded and that it may not be a diagnostic biomarker that can be applied to all clinical settings, for example in our population who underwent abdominal surgery and had co-morbidities. This will only be proven when large studies with homogeneous patient cohorts report on the role of NGAL as a diagnostic biomarker of AKI in this clinical setting.
Further studies are required to determine the clinical and analytical significance of the systemic inflammatory response syndrome (SIRS) and urosepsis on the specificity of NGAL and how it impacts on the clinical utility of the test. The antibody configuration of the assay influences its clinical performance, and the manufacturers claim that the current NGAL detects only the monomeric from of NGAL, which is produced by renal damage. However, our study suggests the antibody may also recognize the dimeric form, which is produced by neutrophils. Recently, we have demonstrated the significant potential interference of leukocyturia in confounding the interpretation of NGAL. 32 The poor specificity of the assay is a major concern as it potentially erodes its value as a definitive biomarker of AKI. NGAL can also be measured in blood; however, we did not measure NGAL in this matrix. Currently, there is no definitive evidence about the optimal biological matrix for analysis; however, a recent review on the analytical issue of NGAL suggests the diagnostic performance seems to better in urine compared to blood. 31 NGAL is currently an expensive biomarker and thus requires optimal clinical utility to justify the cost.
Conclusion
Urinary NGAL had a poor predictive role in evaluating AKI in patients treated using GDHT after major abdominal surgery. However, NGAL may have a potential role as a prognostic marker in the management of patients with SIRS, in particular, in the critical care setting. Preoperative ACR may have a role as a marker in predicting AKI.
Footnotes
Acknowledgements
Abbott Diagnostics donated a portion of the reagent kits. SJ acknowledges support from the NIHR RM/ICR Biomedical Research Centre.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
The study was approved by the London Multicentre Research Ethics Committee and Medical and Healthcare products Regulatory Agency (UK), 06/MRE 02/70.
Guarantor
MCF.
Contributorship
MCF, RMP and SJ conceived the study. MRC performed the analysis and wrote first draft. All authors contributed to subsequent drafts.