
Abstract
To investigate the predictive effects of neutrophil gelatinase-associated lipocalin (NGAL) and kidney injury molecule-1 (KIM-1) on renal-replacement therapy for traumatic acute kidney injury (TAKI). The urinary NGAL and KIM-1 levels of TAKI patients underwent renal-replacement therapy were assessed. The correlation and predictive model were also analyzed. Short-term (28 days) survival rate of patients were 54.5%. As TAKI stage increased, urinary KIM-1 and NGAL level increased significantly (P < 0.05). The urinary KIM-1 and NGAL level, negatively correlated with 28-day survial, were all higher in deceased patients than survival patients (P < 0.05). The Youden index demonstrated the predictive value of urinary NGAL area under the curve (AUC; 0.830) and KIM-1 AUC (0.879) levels in the prognosis of patients in this study. NGAL and KIM-1 can predict the prognosis of patients with TAKI and have significant correlation with the prognosis of patients.
Keywords
Introduction
Traumatic acute kidney injury (TAKI) is a common critical disease. At present, kidney injury caused by shock resulting from serious infection/external trauma has become one of important reasons acute kidney injury (AKI). 1 The pathogenesis of TAKI is very complex, and involves the complex pathophysiological process of kidney tubule cell damage caused by kidney tubules injury, endothelial cell microvasculature, oxidative stress, and immune response. 2 The disease has very high death rate, and accompanied with cardiovascular system and organ damage as well as dysfunction, so the treatment requirements are high. Renal-replacement therapy (RRT) as a new blood purification technology can regulate water and electrolyte transfer and balance, improve immune hyperactivity, and reach internal environment balance so as to promote prognosis improvement. 3 Thus, seeking the biomarker with high sensitivity and specificity for early TAKI diagnosis and adopting proper RRT are very necessary to improve clinical prognosis. 4 Serum creatinine and urine volume are common prognosis prediction indicator, but their diagnosis sensibility and specificity are not high. 5 Recent research has found that neutrophil gelatinase-associated lipocalin (NGAL) can reflect patients’ TAKI status, and NGAL content in the urine of TAKI patients increases. 6 Kidney injury molecule-1 (KIM-1) is a kind of Type-I transmembrane glycoprotein. This factor presents high expression in renal tubular epithelial cell of AKI caused by ischemia and renal toxicity, and it can be split and decomposed into soluble figment which is discharged in urine, so it can be detected as a specific marker. 7 In this study, the predictive effect of NGAL and KIM-1 on RRT for TAKI so as to promote early prediction of prognosis.
Data and method
Ethical approval
The study was approved by the Institutional Ethics Committee of our hospitals, and written informed consent was obtained from all participants.
Object of study
Between September 2013 and February 2018, 55 patients with AKI consecutively admitted to a general intensive care unit (ICU), were analyzed in the following research. Demographic data, characteristics of injury, and severity of trauma variables were collected. The inclusion criteria for the AKI group were the Kidney Disease Improving Global Outcomes (KDIGO) criteria, presented as follows: increased SCr ⩾ 26.5 μmol/L within 48 h, SCr increased by ⩾1.5-fold relative to baseline values within 7 days, or urine volume <0.5 mL/kg/h for 6 continuous hours. The exclusion criteria were as follows: (1) history of nephrotoxic medication use; (2) accompanying underlying kidney disease or liver cancer; and (3) patients with concomitant conditions that might damage kidney function, including rheumatoid immune disease, diabetes and hypertension, coronary heart disease, or cardiac insufficiency.
Treatment method
Sustained low-efficiency dialysis (SLED) treatments, using the Fresenius 4008S ArRT-Plus on-line haemodiafiltration system (Fresenius Medical Care-Asia Pacific Pty, NSW, Australia) were applied to RRT. Accepted urgent indications for RRT in patients with AKI generally include (1) refractory fluid overload; (2) severe hyperkalemia (plasma potassium concentration >6.5 mEq/L); (3) signs of uremia, encephalopathy, or otherwise unexplained decline in mental status; (4) severe metabolic acidosis (pH < 7.1); and (5) certain alcohol and drug intoxications. The RRT is initiated electively in patients with K >6.0 mEq/L or severe metabolic acidosis (pH < 7.2) and among patients who are repeatedly in positive fluid balance despite aggressive attempts at diuresis.
SLED-operating parameters at our institution have been largely standardized. Countercurrent dialysate flows (QD) were routinely set to 200 mL/min, and on-line haemofiltration (QF) to 100 mL/min in pre-dilution mode. Blood flows (QB) were set to between 250 and 350 mL/min as angioaccess permitted. Default treatment duration was 8 h. SLED-treatments discontinued before completion for any reason were restarted only if therapeutic objectives had not already been met. All aspects of SLED treatment were performed and monitored by nursing personnel from the Department of Intensive Care Medicine, including set-up and discontinuation. Haemodialysis personnel with SLED experience were, however, available for troubleshooting and technical advice.
Assessment of renal function
The KDIGO criteria defines AKI as an increase in SCr by ⩾0.3 mg/dL (26.5 μmol/L) within 48 h, an increase in SCr to ⩾1.5-fold that of baseline values, which is known or presumed to have occurred within the previous 7 days, or urine volume <0.5 mL/kg/h for 6 h. Stage 1 is defined as an increase in serum creatinine to more than 1.5- to 1.9-fold greater than baseline values, an increase in SCr ⩾0.3 mg/dL (26.5 μmol/L), or urine output <0.5 mL/kg/h for 6-12 h. Stage 2 was defined as an increase in serum creatinine to more than 2.0- to 2.9-fold greater than baseline values or urine output <0.5 mL/kg/h for ⩾12 h. Stage 3 was an increase in serum creatinine to more than 3.0-fold that of baseline values, an increase in SCr to ⩾4.0 mg/dL (353.6 μmol/L), the initiation of RRT, urine output <0.3 mL/kg/h for ⩾24 h, or anuria for ⩾12 h.
Urine NGAL and KIM-1 indicator test
A 25-mL midstream urine sample was collected from each patient after fasting on the day of hospitalization and centrifuged at 3500g for 10 min at room temperature to remove debris. During analyses, all samples were thawed only once, and urine precipitates were thoroughly mixed after complete thawing. The measurement of urinary KIM-1 and NGAL levels was performed by means of a commercially available ELAISA test kit (Antibody Shop, Gentofte, Denmark).
Observation indicator
Prognosis results of patients and 28-day case fatality rate were recorded. If the survival time is less than 28 days, the prognosis is recorded as death. If they still survive after 28 days, the prognosis is recorded as survival. Meanwhile, basic data of all patients were recorded, including age, gender, body mass index (BMI), combined disease, sequential organ failure assessment (SOFA), and acute physiology and chronic health evaluation II (APACHE II).
Statistical method
Epidata 3.1 software was used for data registration. SPSS 19.0 software was used for data analysis. Normally distributed quantitative data are shown as the mean ± standard deviation. Analysis of variance was used to compare differences among multiple groups. The least significant difference (LSD) test was used for pairwise comparisons. Chi-square test was adopted for comparison, and Kaplan–Meier test was used for survival analysis. Correlativity between two variables was analyzed with Spearman correlation analysis. To measure the sensitivity and specificity of urinary NGAL and KIM-1 at different cut-off values, a conventional receiver operating characteristic (ROC) curve was generated. The area under the curve (AUC) for each ROC curve was used to quantify the capacity of NGAL and KIM-1 to diagnose AKI and predict the mortality. An area of 0.5 is no better than expected by chance, whereas a value of 1.0 signifies a perfect biomarker. P value less than 0.05 was statistically considered significant.
Results
Prognosis
APACHE II and SOFA scores were calculated using the Riyadh Intensive Care (RIP) program. There was no significant difference in sex, age, BMI, and complications between the two groups at admission (P > 0.05). The SOFA score and APACHE II score of the dead patients were higher than those of the survivors (P < 0.05). See Table 1. After treatment, 30 patients survived in 28 days and 25 died. The survival rate was 54.5%.
Comparison of general information.

BMI: body mass index; SOFA: sequential organ failure assessment; APACHE: Acute Physiology and Chronic Health Evaluation.
Comparison of urinary KIM-1 and NGAL among patients with different stages of AKI
The patients in the AKI group were divided into three groups according to the 2012 KDIGO staging criteria. A total of 12 patients were classified as Stage 1 AKI, 16 as Stage 2 AKI, and 27 as Stage 3 AKI. Urianry NGAL and KIM-1 were compared among the groups. Urinary KIM-1 levels in Stage 3 AKI patients (8.9 ± 0.3 ng/L) were significantly higher than either those in Stage 2 AKI patients (6.7 ± 0.4 ng/L), or those in Stage 1 AKI patients (5.9 ± 0.7 ng/L); all differences were statistically significant (P < 0.05) (Figure 1(a)). Urinary NGAL levels in Stage 3 AKI patients (171.8 ± 12.1 μg/L) were significantly higher than either those in Stage 2 AKI patients (149.1 ± 12.3 μg/L), or those in Stage 1 AKI patients (139.7 ± 13.4 μg/L); all differences were statistically significant (P < 0.05) (Figure 1(b)).

(a) Comparison of urinary kidney injury molecule-1 (KIM-1). (b) Urinary neutrophil gelatinase-associated lipocalin (NGAL) in different stages of acute kidney injury (AKI).
Comparison of urinary KIM-1 and urinary NGAL in living and deceased patients
Of 55 patients, 25 died, resulting in a mortality rate of 45.5%. Results showed that urinary KIM-1 levels, urinary NGAL levels among the deceased patients (8.9 ± 0.5 ng/L, 170.7 ± 20.2 μg/L) were significantly higher than those among the living patients (6.4 ± 1.1 ng/L, 135.1 ± 15.4 μg/L) (Figure 2).
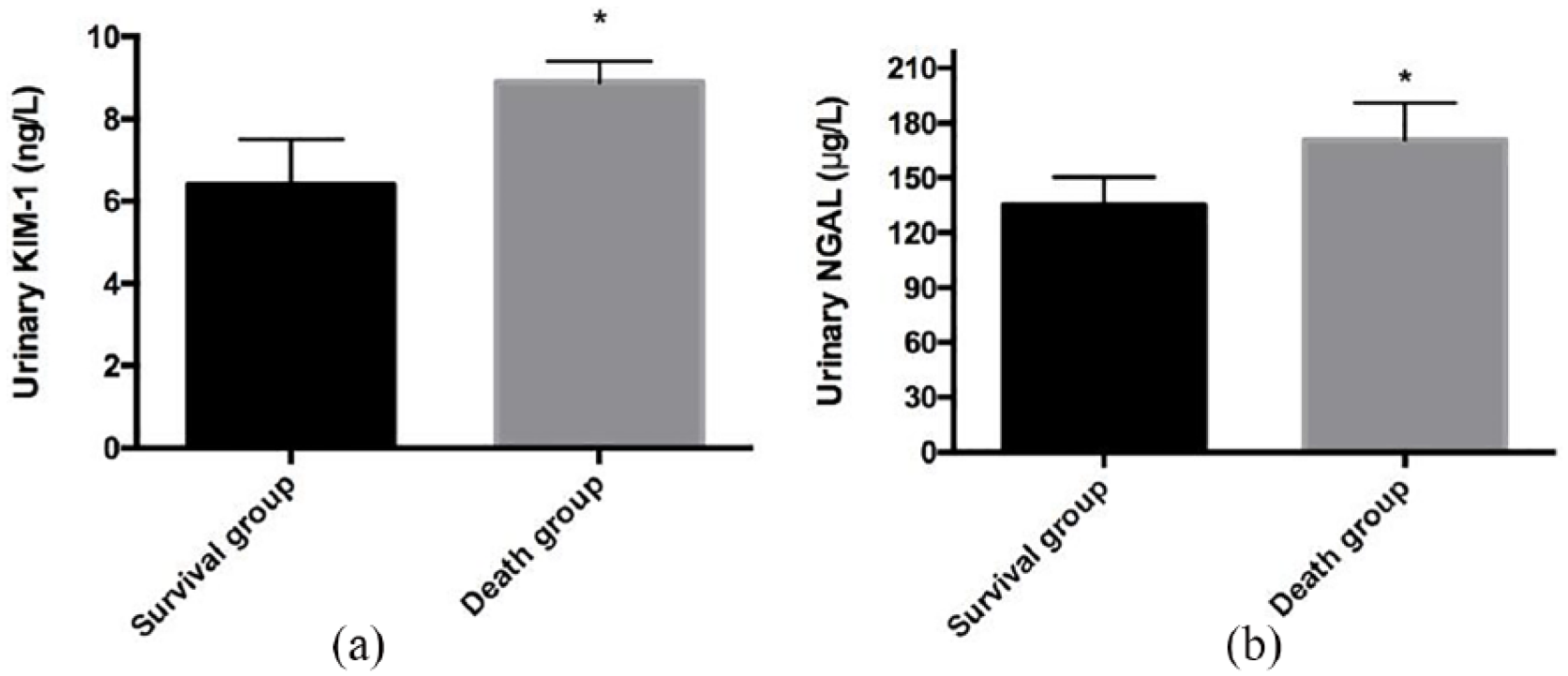
(a) Comparison of urinary kidney injury molecule-1 (KIM-1). (b) Urinary neutrophil gelatinase-associated lipocalin (NGAL) between living and deceased patients in the acute kidney injury (AKI) group.
Correlation analysis and predictive value
Using univariate regression analysis, we demonstrated that, among the 55 patients, the 28-day survival of patients with urine NGAL (r = –0.529, P = 0.008) and KIM-1 content (r = –0.492, P = 0.011), SOFA score (r = –0.566, P = 0.004) showed a significant negative correlation with the APACHE II score (r = –0.633, P = 0.000).
Efficacy of urinary KIM-1 and urinary NGAL for the diagnosis of AKI during SLED
An ROC curve was then plotted using urinary KIM-1 and urinary NGAL as experimental variables and AKI under treatment of dialysis as the state variable. The AUC of urinary NGAL was 0.830 (95% confidence interval (CI): 0.741–0.919, P < 0.05), and when urinary NGAL concentration was 51.74 μg/L, the sensitivity and specificity were 79.1% and 80.9%, respectively. The AUC of KIM-1 was 0.879 (95% CI: 0.793–0.948, P < 0.05), and when urinary KIM-1 concentration was 4.77 ng/L, the sensitivity and specificity were 77.5% and 79.5%, respectively. This shows that urinary KIM-1 and urinary NGAL have predictive value for AKI during SLED.
Discussion
Although RRT has excellent effect, prognostic mortality of TAKI stays at a high level. The definite mechanism and clinical features of TAKI are still not clear, and early diagnosis toll for TAKI may be beneficial to improvement of TAKI prognosis. Conventional SCr and other indicators cannot definitely reflect glomerular filtration rate (GFR) because GFR is influenced by tubule SCr secretion and non-renal factors. Besides, SCr secretion is also influenced by multiple factors such as age, gender, weight, active state, diet, drug, and liver function. 8 This study indicated that SOFA score and APACHE II score of dead patients were higher than that of the patients alive (P > 0.05). However, the systems of SOFA score and APACHE II score are complex, so their clinical application is restricted.
NGAL is closely related to bacterial growth and tissue differentiation. The expression of NGAL in normal human kidney tissue is low. However, when renal tubular epithelial cells are damaged, its expression is significantly increased. 9 KIM-1 can regulate the adhesion between regenerated cells and endocytosis, and the soluble fragments produced fall off from cells into urine, which may be an early marker of renal injury. 10 Meanwhile, the urine NGAL and KIM-1 content of dead patients were significantly higher than that of the patients alive (P < 0.05). Based on the roles of urinary KIM-1 and urinary NGAL, this study evaluated their value in predicting AKI during SLED. An ROC curve was plotted using urinary KIM-1 and urinary NGAL as experimental variables and AKI under treatment of dialysis as the state variable. It was found that either urinary KIM-1 or urinary NGAL had predictive value for this condition (all P < 0.05).
This study also has some defects. For example, patients’ urine NGAL and KIM-1 are not detected dynamically, and there are many factors influencing patients’ prognosis. Multi-center, multi-sample, and multi-indicator analyses will be carried out next.
In conclusion, this study found that NGAL and KIM-1 can predict the prognosis of TAKI patients to a certain extent during the treatment of TAKI with renal replacement (SLED), and there is a correlation between NGAL and KIM-1 and the prognosis of TAKI patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.