
Abstract
Background
Pre-analytical variables are common across all laboratories and can negatively impact on patient care. The aim of this study was to review the impact of electronic requesting in Primary Care on the number of pre-analytical errors seen by the laboratory.
Method
Error data were reviewed during two six-month periods, pre- and post-implementation of Primary Care electronic requesting. The outcome measures related to: the correct information on the sample tube (patient name, unique patient ID number, date of collection); the correct sample received and the availability of a clinical history.
Results
There was a marked decrease in the number of pre-analytical errors following the introduction of electronic requesting (2764 pre-implementation vs. 498 post-implementation, P < 0.001). There was an improvement in the quality of information provided with each request in the forms of clinical history, date and time of sample collection.
Conclusions
The introduction of electronic requesting in Primary Care can reduce the number of pre-analytical errors and can improve the quality of information received with each request.
Introduction
Sample processing can be divided into three processes: pre-analytical, analytical and post-analytical. The majority of errors occur in the pre-analytical phase. These are mainly due to incorrect information on the request form or the sample. 1
The Carter report highlighted the importance of pathology services to the NHS, and the end-to-end service they offer. 2 It is essential for laboratories to reduce the number of pre-analytical errors and improve patient care. Several studies have examined ways to reduce pre-analytical errors including teaching programmes and visual aids but have failed to show any significant improvements.3,4
In the sample pathway, entering patient information into the laboratories information systems has always been one of the bottlenecks in sample processing. Specific issues in this area such as illegible writing can lead to the misidentification of patients. Electronic requesting has the potential to reduce pre-analytical errors. It can be used to educate users at the time of sample collection, using specific messages and ensure sufficient information for the interpretation of the tests requested is supplied by the requesting clinician. 5
We aimed to show that the introduction of an electronic order communication system in Primary Care has reduced the number of pre-analytical errors and improved the quality of information received.
Methods
All biochemistry requests received from Primary Care by the Department of Clinical Biochemistry, Aberdeen Royal Infirmary were reviewed for pre-analytical errors. The laboratory follows a strict sample acceptance policy that outlines the minimum sample requirements for a sample to be processed, and covers the following: patient’s community health index number (CHI, the unique patient numbering system used in NHS Scotland); date of collection; correct sample tube type; appropriate request form used; sufficient patient ID on sample tube and sample mismatches (different names on the sample and request form). While our sample acceptance policy includes all the above information as mandatory fields, there is allowance for cases such as temporary residents who do not have a CHI number. All samples that do not comply with this policy are clearly recorded as non-compliant on the laboratory computer system (APEX, iSOFT plc, Banbury, UK).
Data were collected over two six-month periods, pre- (September 2008–February 2009), and post-implementation (September 2011–February 2012) of electronic requesting becoming available in Primary Care (Anglia ICE, Sunquest, UK). Following implementation of electronic requesting all General Practitioner practices started paperless requesting. The sample label contained the following information: patient name; CHI number; unique sample identifier; tube type and laboratory discipline. The categories were pre-specified according to the criteria on the departmental sample acceptance policy. Chi-squared analysis was carried out to identify if there were any significant differences between the two time periods (Minitab, release 13.1). The number of requests for which no patient CHI number was used during each of the two periods of the study was compared using Fisher’s exact test.
Results
The effect of electronic requesting in Primary Care on pre-analytical variables.
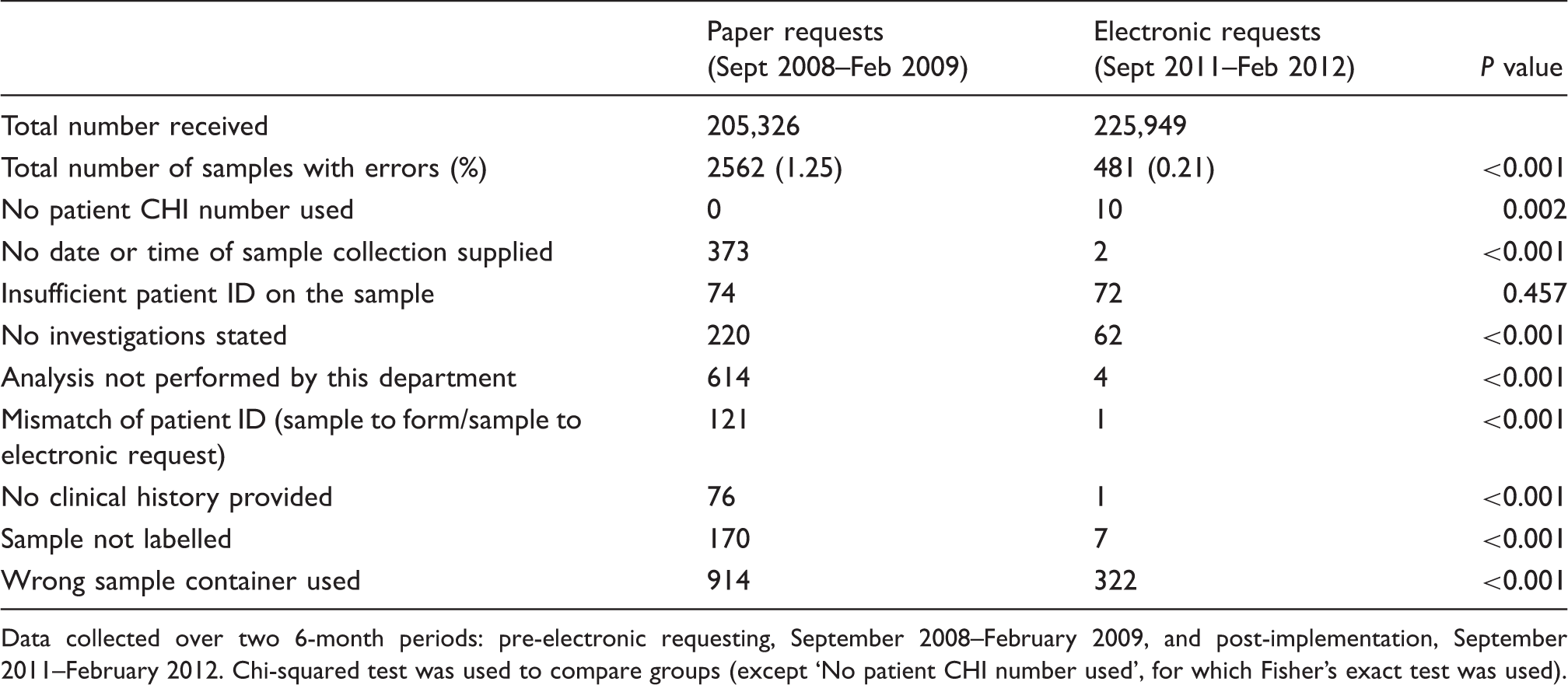
Data collected over two 6-month periods: pre-electronic requesting, September 2008–February 2009, and post-implementation, September 2011–February 2012. Chi-squared test was used to compare groups (except ‘No patient CHI number used’, for which Fisher’s exact test was used).
Prior to using electronic requesting a large number of the errors were due to samples being sent to the wrong laboratory discipline (n = 614); this has reduced to only four cases once electronic requesting was introduced. Another common error was sending the wrong sample tube type. Prior to electronic requesting 914 requests were received in the wrong container within a 6-month period; this dropped to 322 requests after implementation (P < 0.001).
Disappointingly an increase was seen in the number of samples received without the patient CHI number, 10 compared with 0 pre-implementation. There has been no significant change in the number of samples received with insufficient patient ID on the sample tube, 74 pre-implementation and 72 samples after electronic requesting was implemented (P = 0.457).
In terms of the quality of information received, the introduction of electronic requesting has significantly reduced the number of samples received without a clinical history (76 cases pre-implementation vs. one post-implementation, P < 0.001) or with no date or time of collection stated (373 cases pre-implementation vs. two post-implementation, P < 0.001).
Discussion
The main objective of electronic requesting in Primary Care was to improve the quality of information received with each request. We have shown evidence that electronic requesting has reduced the number of pre-analytical errors. We have also shown that the use of electronic requesting improves the quality of information supplied with each request.
The electronic request generates a printed sample label that clearly indicates which sample tube should be used and where the sample should be sent. We have shown that this has led to significant improvements but issues still occur if the wrong request label is placed on the wrong tube.
Electronic requesting will never produce a zero-error environment, and the occurrence of some errors did not change. The lack of patient ID on the sample has remained an issue. It was hoped that electronic requesting would eliminate this pre-analytical error. The fact that it did not can in part be explained by issues in the roll-out of the new system. The printers used to print sample labels occasionally missed printing patient ID information; this has since been rectified. Users were warned of the error and asked to double check each label prior to sending the sample into the laboratory. The increase in samples received without a patient CHI number can also be explained by this issue.
Electronic requesting can stipulate the information supplied with each request, which in turn enables laboratory staff to interpret the results more appropriately, and improve the service the laboratory can offer its users. 5 Electronic requesting has the potential to save money for the NHS by reducing the repeat requests created when the original sample was non-compliant. However, we are aware that the system is not perfect and errors will continue to occur. Therefore continued education of users is essential. The computer system is flexible so that modifications can be made continuously to ensure users have the most up to date information. It has been proposed that electronic requesting will enhance the role that pathology has in patient care pathways. 6 Electronic requesting has the potential to revolutionize pathology services, but requires the support of its users, IT services and laboratory staff for it to be user-friendly and successful.
An observational study such as this clearly has limitations. The two periods over which data were collected were three years apart. Although the introduction of electronic requesting was the significant change implemented between these two periods, we cannot exclude effects of unmeasured confounders. However, there were no other significant changes made to the primary care procedure for requesting biochemistry investigations during this time period.
We have shown that electronic requesting can improve the information received from users and reduce pre-analytical errors, thus positively impacting on pathology services.
Footnotes
Declaration of conflicting interests
None.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethical approval
Not applicable.
Guarantor
HET.
Contributorship
BLC had the original concept for this paper. AK collected the data. HET processed the data and prepared the draft paper. KAD assisted with the statistical analysis. All authors reviewed and edited the final version of the manuscript.