
Abstract
Introduction:
Urinary metanephrines are widely used in the diagnosis of catecholamine secreting tumours. Over the past two years we have been using the commercial Recipe® ClinRep® Complete Kit for Metanephrines in Urine coupled with high-performance liquid chromatography and coulometric detection. It was noticed that the internal standards on the patient chromatograms were sporadically raised due to interference.
Methods:
The interference had identical chromatographic and electrochemical properties to the Recipe® internal standard (undisclosed identity). Inspection of the patient names showed it seemingly had a higher frequency and magnitude in patients of Indian origin. The source of the interference was tracked by dietary observation and intervention to curry leaves, a common component of Indian foods.
Results:
The interference was chromatographically and electrochemically indistinguishable from the internal standard. The mass spectrum of the pentafluoropropionate derivative of the interference matched the Recipe® internal standard and was identified as methoxyhydroxybenzylamine by library match.
Conclusion:
The component co-elutes exactly with internal standard and artifactually decreases the metanephrine and normetanephrine results. It is surprising that it has not been described previously. Patients being assessed for catecholamine secreting tumours should be advised to withdraw from eating Indian foods at least 24 h prior to commencement of urinary collection.
Introduction
Urinary metanephrines are still recommended in the diagnosis of catecholamine secreting tumours.1,2 Over the past two years a commercial Recipe® ClinRep® Complete Kit 3 for Metanephrines in Urine has been used with high-performance liquid chromatography and coulometric detection. We had previously 4 noticed that the internal standard on the patient chromatograms was sporadically raised due to interference and often very substantially. Inspection of the patient names showed the interference seemingly had a higher frequency and magnitude in patients of Indian origin. Drug interferences have been described5–7 but dietary interference appears to be uncommon.
Experimental
High-performance liquid chromatography with electrochemical detection
Analyses were performed on a Dionex Ultimate HPLC system consisting of a 3000 pump modified with an in-line degasser and pulse dampener and an Ultimate 3000 autosampler.
Detection was by Coulochem III (ESA, Chelmsford, MA, USA) equipped with a 5021A conditioning cell at −650 mV and a 5011A analytical cell at −100 mV (electrochemical detector cell; ECD1) and +450 mV (ECD2). The optimum detector settings were determined by voltammetry. The upstream conditioning cell was kept strongly reductive to greatly improve metanephrine sensitivity at the downstream oxidative ECD2 electrode. The voltammogram showed a tenfold improvement if the conditioning cell is held at −650 mV or below. This upstream reduction removes dissolved oxygen in the mobile phase. Helium sparging of the mobile phase also improved sensitivity but only to about half of the electrodic reduction.
The column and cells were kept at constant 40℃ temperature. The column was Phenomenex Prodigy ODS(3) 150 mm x 4.6 mm 5 µm particle size. This was equivalent to the Recipe® ClinRep® analytical column (catalogue #4030) but was slightly more retentive. The mobile phase was supplied by Recipe® and was used without modification. The flow rate was 1.0 mL/min through an in-line graphite filter supplied by ESA.
For comparative purposes only, amperometric detection was made on Decade II (Antec-Leyden, Zoeterwoude, The Netherlands) with a VT03 cell, 50 µL spacer and an in situ Ag/AgCl reference cell. Detector voltage was 0.65 V at 30℃ with 2 mmol/L NaCl added to the Recipe® mobile phase.
Gas chromatography-mass spectrometry
Gas chromatography-mass spectrometry (GC-MS) was performed on a Hewlett Packard HP 6890 gas chromatograph interfaced to an HP 5973 Quadruple mass spectrometer and Chemstation software. The gas chromatograph was operated in the splitless mode using helium as carrier gas. The column was an HP-5MS capillary (30 m, 0.25 mm id; 0.25 µm film thickness). A Hewlett-Packard HP 7683 series autosampler was used for automatic sample injection. The injector temperature was 225℃. The oven was held at 150℃ for 1 min, then ramped at 20℃ per minute to 290℃ and held for 6 min. The overall run time was 16 min.
Sample preparation
Sample preparation followed that stated by Recipe® ClinRep® Complete Kit for Metanephrines in Urine (catalogue #4000). 3 Briefly, 1 mL specimens with added internal standard (catalogue #4012) were hydrolyzed in acid, cooled and pH adjusted using diluting solution (catalogue # 4022) containing indicator dye. They were then applied to sample preparation columns (catalogue #4020) drained and washed with water, washing solution (catalogue #4023) and repeat water before being eluted with eluting reagent (catalogue #4024) for collection into stabilizing reagent (catalogue #4025). The extracts were injected into the chromatograph. Quantitation was made against Recipe® ClinCal® calibrators using the values assigned by the manufacturer and controlled using BioRad Lyphochek® Quantitative Urine Controls levels 1 and 2. The internal standard as supplied by Recipe® (catalogue #4012) is undisclosed but is most likely an isomer of methoxyhydroxybenzylamine (MHBA).
Results
Interference of internal standard
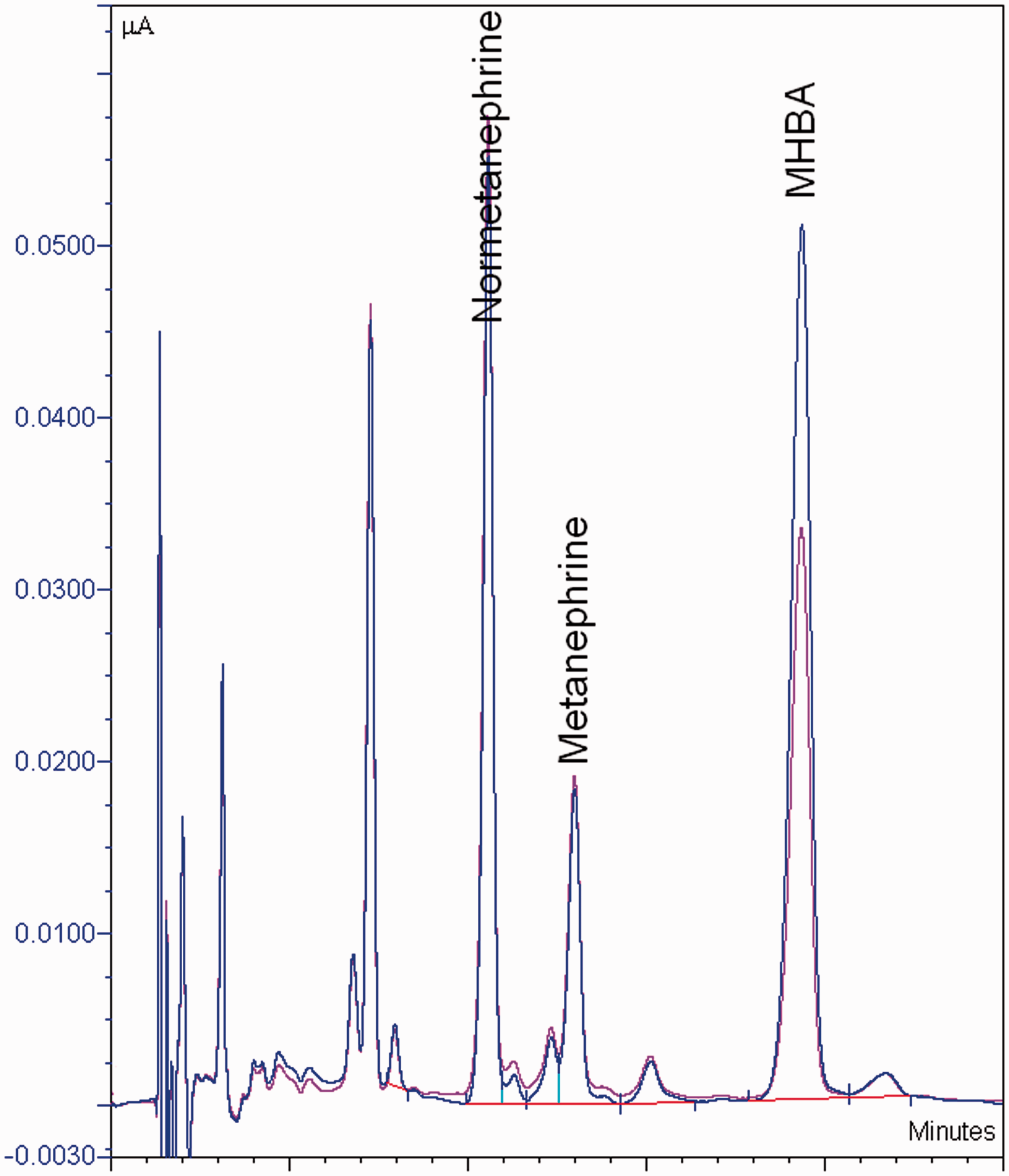
Figure 1 shows the relative internal standard peak heights for 552 consecutive patients over three representative months. They are presented as multifold values relative to the internal standard peak height of the calibrator within their respective batches. The distribution of the multifold values is skewed upwards with several obviously high values. Transformation of the data revealed that any multifold increase above 1.35 could not be explained by this distribution and was considered a potential interference. This occurred in 42/522 (8.0%) of patients. We had determined that the within-patient variation in internal standard peak height was ±4%. A series of these patients were re-analysed with and without added internal standard. In all cases the increase was entirely explained by a peak exactly co-eluting with the internal standard. Figure 2 shows a typical chromatogram with this interference.
Fold increase in MHBA peak height relative to calibrator. HPLC overlay chromatogram of a patient with and without internal standard showing the MHBA interference.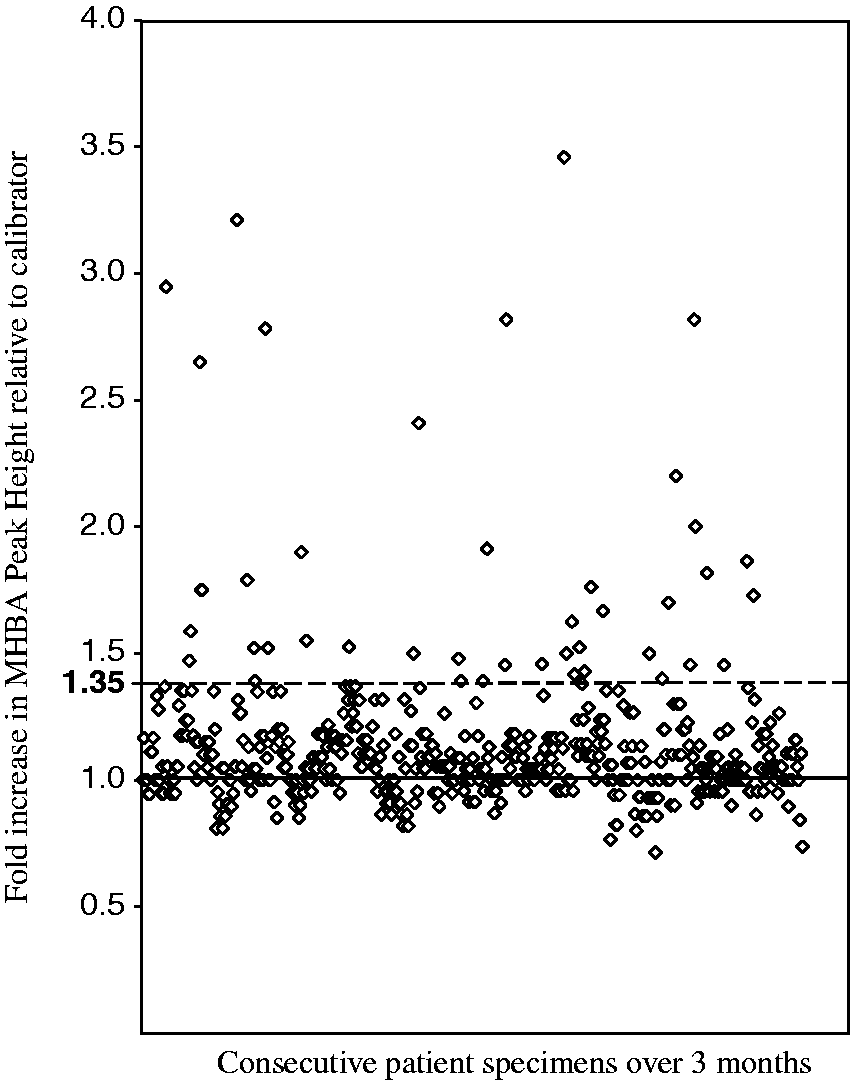
Characteristics of the internal standard interference
Interference in BioRad Lyphochek® Quantitative Urine controls.
This interference was not observed in Recipe® ClinChek® control material nor in any RCPAQAP external quality control material from cycle 49 (2009) to cycle 56 (2012).
The interference is conjugated and hence not detectable in unhydrolysed urine extracts.
We have previously observed that by varying the pH of mobile phase we can successfully resolve interfering peaks from the analytes that one wants to quantify. 8 However, in this instance the interference invariably co-eluted with the internal standard and was chromatographically indistinguishable when the pH of the mobile phase was adjusted across a full range of 3.5–7.5. Additionally, the interference could not be resolved using another column Phenomenex Phenylhexyl 150 mm x 3.1 mm 3µm particle size which has a different selectivity for the internal standard.
The electrochemical properties of the interference matched those of the internal standard. It was present in chromatograms with both coulometric and amperometric detectors. It was equally oxidizable to the internal standard with indistinguishable voltammograms. Importantly, it was not produced in situ by reduction in the Coulochem conditioning cell.
Identification of the interference by gas chromatography-mass spectrometry
Blank urines with and without added internal standard and a patient’s sample which had the interference were extracted and derivatized by pentafluoropropionic anhydride. The method used for extraction and derivatization was from Muskiet et al. 9
The retention times and mass fragmentation pattern (Figure 3) of the internal standard and the interference are identical and match the pentafluoropropionyl derivative of 4-methoxy-3-hydroxybenzylamine. It is concluded that the interference is MHBA. We cannot distinguish which MHBA isomer because they may have indistinguishable chromatographic properties.
Fragmentation pattern of pentafluoropropionyl derivative of MHBA internal standard and the interference (both at retention time 3.97 min).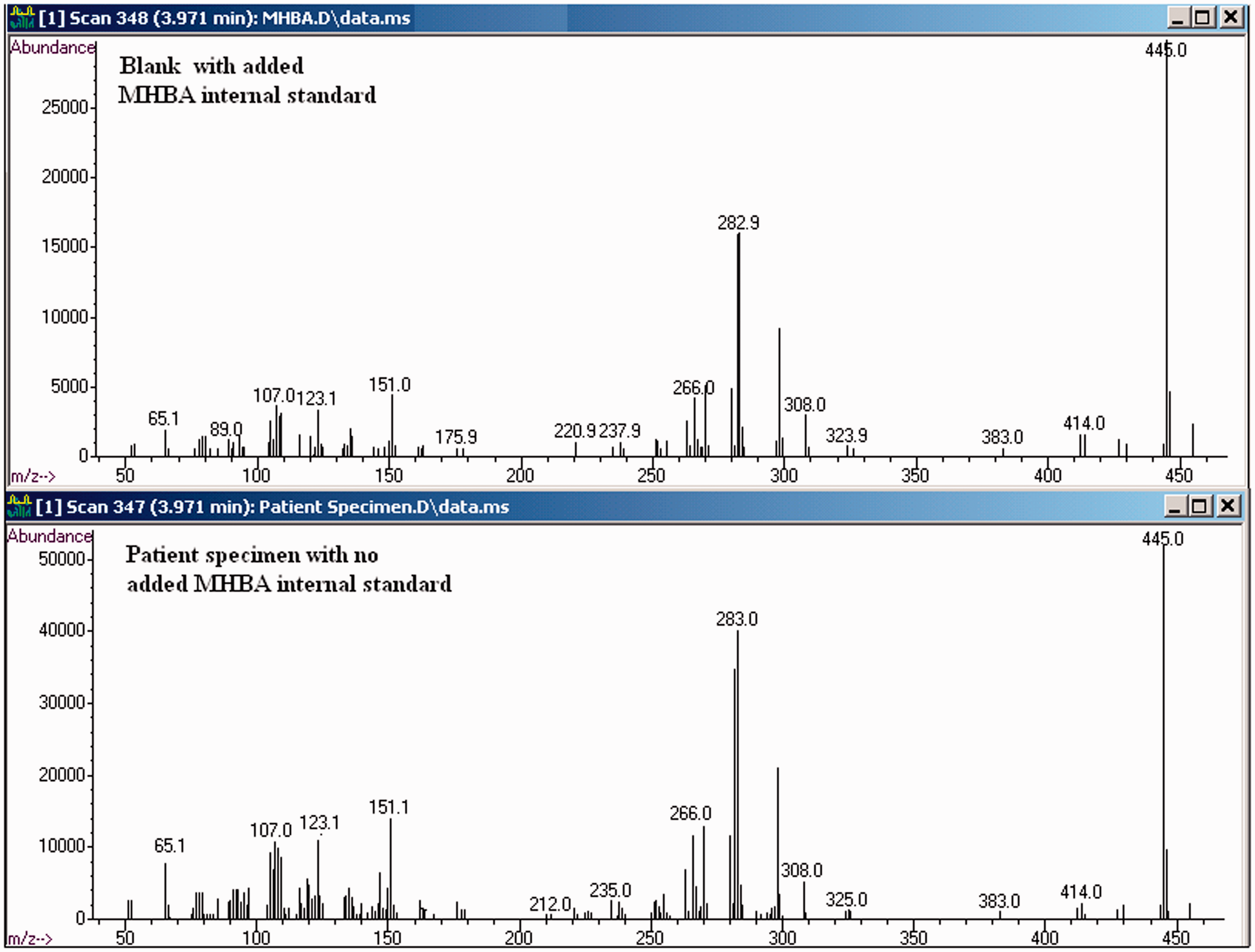
Dietary observational study
The likely source of the interference was sought. Based on the higher frequency observed in patients with Indian names casual urine samples were collected from 10 Indian co-workers consuming their usual diets. Five of them had multifold elevations (1.5–4.5) in their internal standard peak heights. This agrees with our initial findings whereby Indians were overrepresented with substantial interferences on the internal standard peak.
Dietary intervention studies
One of the 10 volunteers was further investigated by dietary withdrawal of all Indian food for 3 days. Figure 4 shows a decrease in the interfering peak during abstinence and the subsequent increase on recommencement. No internal standard was added to any of the urine samples. A volunteer of European decent who does not normally eat Indian food was challenged with a single typical Indian meal. The interference peak appeared after only 3 h.
Partial overlaid chromatograms showing MHBA interfering peak during dietary withdrawal in one volunteer: (a) on usual diet, (b) after Indian diet withdrawn for 3 days and (c) after resumption of usual diet for 1 day.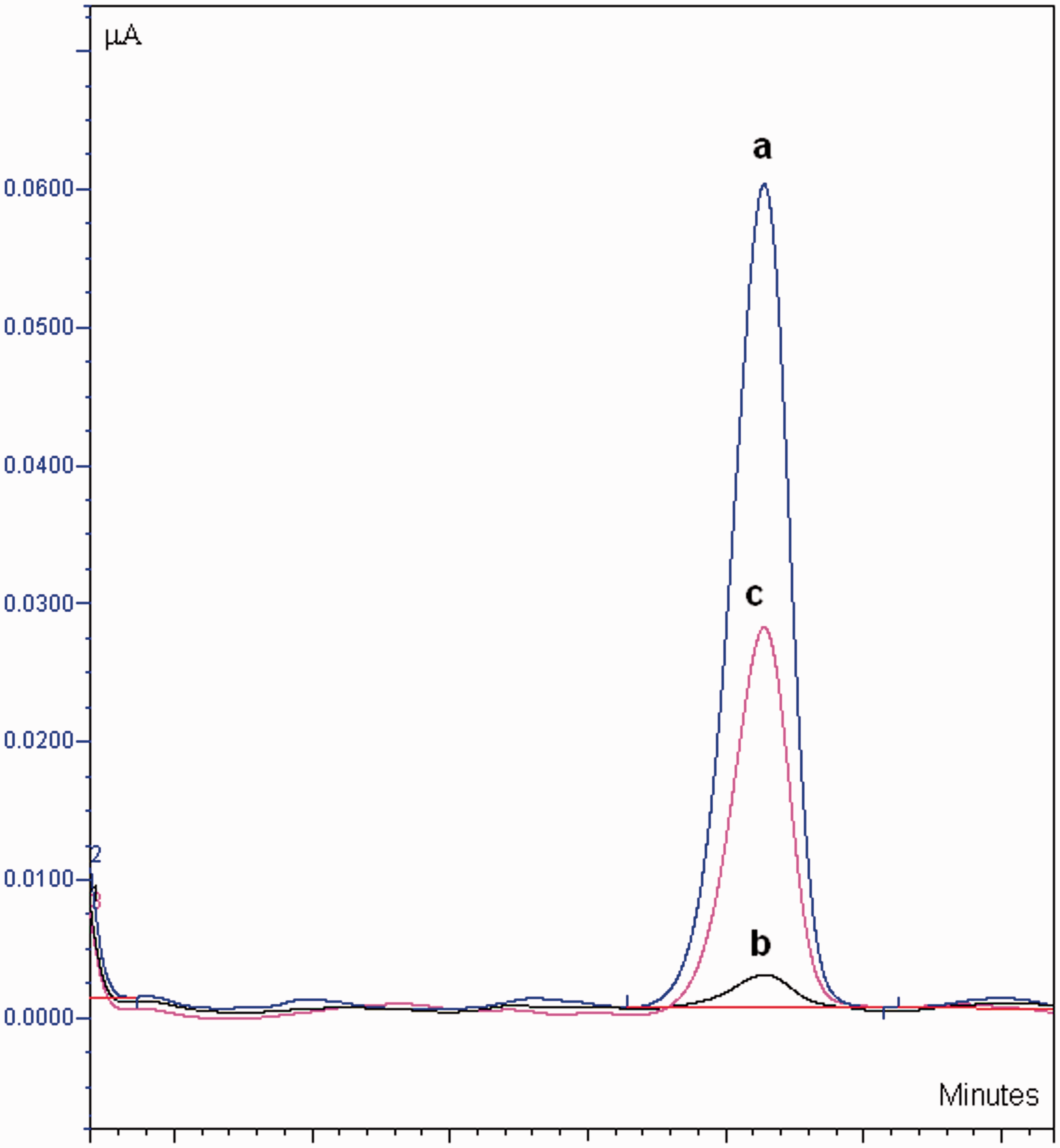
Dietary origin of interference
Examination of the diets of the four volunteers who had substantially raised MHBA interferences suggested a common ingredient was curry leaves. Incidentally, the food consumed by the European also contained curry leaves. In order to further isolate the possible component of the diet contributing to the interference, omelette prepared with curry leaves was consumed by three European volunteers who are not normally exposed to Indian food. The time course of the appearance of the interference is presented in the chromatograms with no added internal standard (Figure 5). This shows that the rate and extent of the interference vary between the subjects but always appears within 3–12 h.
Partial overlaid chromatograms showing appearance of MHBA interfering peak after a single dietary challenge of curry leaves: 0 h: pre dietary challenge; 3 h: 3 hours after curry leaf ingestion; 6 h : 6 hours after curry leaf ingestion and 12 h: 12 hours after curry leaf ingestion.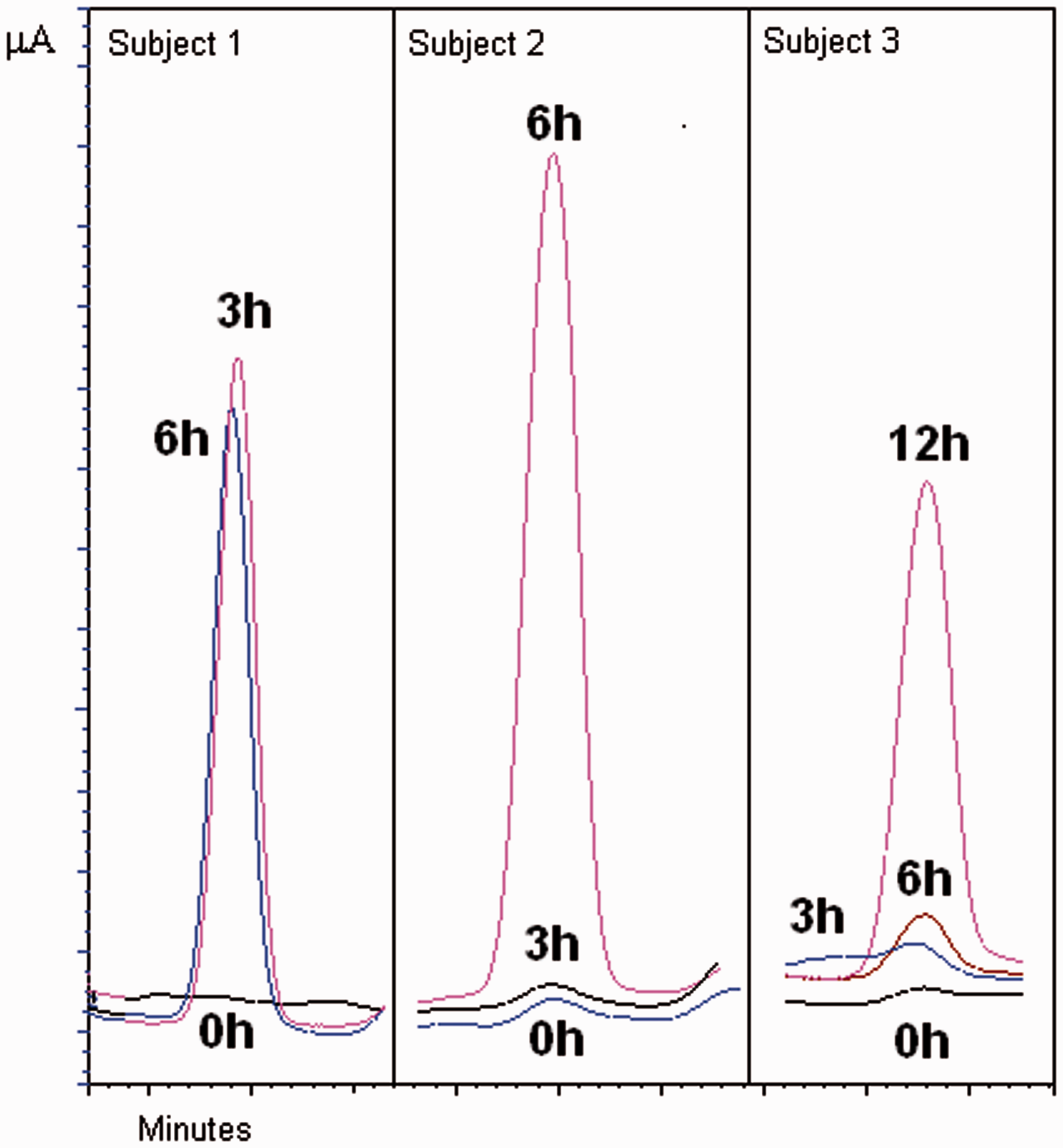
Discussion
Urinary metanephrines are well established biomarkers for phaeochromocytoma and are in routine service in widespread locations. In normal circumstances, the peak heights of internal standards are expected to be constant and part of usual batch validation is to inspect these to assess recovery or correct internal standard addition. Following the establishment of our service using a commercial assay from Recipe® it was noticed that the internal standard was frequently raised. Early experiments showed this was not due to altered recovery, instead was due to the co-elution of an interfering peak. Our initial response was to attempt to resolve the interference chromatographically firstly by altering the mobile phase pH and then by using a phenylhexyl column with different selectivity. These were unsuccessful and we were also unable to use a more selective oxidation potential because of identical electrochemical properties. The properties of the interference were so strikingly similar to that of the internal standard that it was considered to be possibly the same compound. GC-MS was then used in an attempt to identify the interference. The pentafluoropropionate derivative had matching mass spectra to the internal standard which was recognized as 4-methoxy-3-hydroxybenzylamine against the mass spectral library. This does not exclude 3-methoxy-4-hydroxybenzylamine isomer which may have the same spectrum. Consequently, the origin of the MHBA interference was sought having observed that it was present more frequently, though not exclusively, in patients with Indian names. The interference was also seen in Europeans though seldom as high as that found in Indians. Occasionally, it was very high in Pacific Islanders and other Asians. The dietary observational studies on Indian co-workers and subsequent evaluation of their diets pointed to the interference being caused by a component of Indian foods. The dietary interventions proved this and led us to suspect curry leaves (from native Indian tree Murraya koenigii) were the primary source. These are a common ingredient in many Indian foods. Other food sources have not been excluded. Interestingly, acyl derivatives of 3-methoxy-4-hydroxybenzylamine are capsaicinoids which are the compounds found in capsicum genus including chilli peppers. The time course for the interference has not been examined in detail but it appears within hours of dietary exposure. It is not known if the interference is present as such in curry leaves or is a metabolic product of another component.
The consequences to this interference are far reaching. Using the Recipe® calibrator we were unable to attain the target values of the BioRad controls which contain this interference. More importantly, some patients can have interferences which are over three times larger than the added internal standard which severely underestimates the metanephrine results. To our knowledge this interference has not been widely reported. Patients being assessed for catecholamine secreting tumours should be advised to withdraw from eating Indian foods at least 24 h prior to commencement of urinary collection.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
None.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethical approval
Not required.
Guarantor
HM.
Contributorship
HM and GW validated the commercial metanephrine method. GW installed and routinely ran the metanephrine service. HM and GW collectively noticed the internal standard interference. HM recruited subjects for dietary studies and performed the mass spectrometry. Both authors wrote the manuscript and approved the final version.