
Abstract
Background
The inappropriate use of tumour markers (TMs) is a common problem. The aim of this audit was to evaluate the impact of local guidelines on the TM requesting patterns of a General Surgery Department.
Methods
CA 125, CA 19-9, CA15-3, CEA, AFP and HCG requests from all hospital surgical locations were audited over two periods of eight months before and after the implementation of local requesting guidelines.
Results
Postintervention, total TM requests decreased by 32% while patient requests decreased by 9.8%. Single TM requesting increased and requests for panels containing four or more TMs decreased from 279 to 60 requests (78% reduction).
Conclusion
Interdepartmental collaboration and the implementation of local guidelines have resulted in a change in requesting behaviour, most notably a reduction in multiple TM panel requests.
Introduction
Tumour markers (TMs) are substances present in the body which, when measured, provide information on the presence or progression of malignancy. While some TMs provide useful information during diagnosis of malignancy, they have been found to be of most clinical use in monitoring treatment and detecting disease recurrence.
The use of TMs in everyday medical practice has become routine. This has resulted in an increased workload for many biochemistry laboratories in recent years. 1 Current guidelines encourage organ appropriate single TM requesting and advise against opportunistic screening with multiple TMs in patients with non-specific symptoms.2,3
Despite their limitations with regard to sensitivity, specificity and limited positive predictive value in unselected populations, many reports have been published describing their inappropriate use.1,4,5
The Cardiff and Vale University Health Board serves a population of around 445,000 people living in Cardiff and the Vale of Glamorgan, and additionally offers specialist services to the South and Mid Wales area. The Health Board has a total of 1548 beds over six sites. The University Hospital of Wales currently has 841 beds which include approximately 132 General Surgery ward admission beds.
Managing demand in the current economic climate is a great challenge to most laboratories. The number of TMs analysed in our department increased from 23,383 in 2000 to 43,984 in 2009. Anecdotally we noticed that requests from the General Surgery Department contained an unexpected number of TM panels containing four or more different TMs requested per individual patient. Clinical information on request forms was often inadequate or irrelevant, making it difficult to assess the appropriateness of requests. This together with audit of the numbers and request locations led us to suspect that a high number of TMs were inappropriately requested for opportunistic screening or diagnosis rather than monitoring and follow-up.
Aim
The aim of this study was to compare the requesting patterns of the University Hospital of Wales’ General Surgery Department before and after the implementation of local TM requesting guidelines.
Method
We performed a baseline retrospective audit of TM requests between March and October 2009. The TMs audited included carbohydrate antigen-125 (CA 125), carbohydrate antigen-19-9 (CA 19-9), carbohydrate antigen-15-3 (CA 15-3), carcinoembryonic antigen (CEA), alpha-fetoprotein (AFP), human chorionic gonadotropin (HCG) and prostate-specific antigen (PSA). PSA requests from Urology locations and HCG pregnancy requests were excluded. Data collection was performed by extraction from the laboratory information system. Surgical locations audited included the Surgery Outpatient Department (SOPD), the Short Stay Surgical Unit (SSU), the Surgical Assessment Unit (SAU) and three surgical inpatient wards. The SSU admits day cases, but also acts as an overflow unit to the SAU.
Results of the audit raised concern as to the awareness of indications for TM requesting. We raised this concern with our surgical colleagues. As a result local TM requesting guidelines (based on The National Academy of Clinical Biochemistry practice guidelines)2,3 were produced by the Surgery Department in conjunction with the Biochemistry Department (Appendix 1). As a further measure, a minimum retest interval of five days for all TMs was agreed. Any requests received breaching this time limit would be automatically rejected by the laboratory. Specific clinical scenarios which could arise in which a repeat TM was needed within the five-day interval would be vetted by the Chemical Pathologist validating TM results.
The requesting guidelines were introduced in February 2010. The guidelines were discussed in the local Surgery departmental meeting and distributed to all wards and the outpatient department in the form of posters. They could be accessed electronically on the hospital information system as a link from the laboratory test information page. New junior doctors joining the Surgery Department on a rotational basis were given these guidelines as part of their induction pack.
Following the implementation of these local guidelines, we performed a postintervention re-audit of the same period during the following year (1 March 2010 to 31 October 2010). Statistical analysis was performed using Microsoft Excel.
Results
During the eight-month baseline audit period, the Surgery Department requested 1878 TMs on 727 patients. Thirty-eight percent of all requests consisted of panels containing four or more TMs. On the wards more than half of requests (53%) were for panels of four or more markers (Figure 1). Seventeen requests asked for five or more TMs. It is noteworthy that 33% of CA 125 requests were on male patients.
Number of tumour marker panels requested during the 2009 baseline preintervention audit. SAU: surgical assessment unit; SSU: short stay surgical unit; SOPD: surgical outpatient department; TM: tumour marker.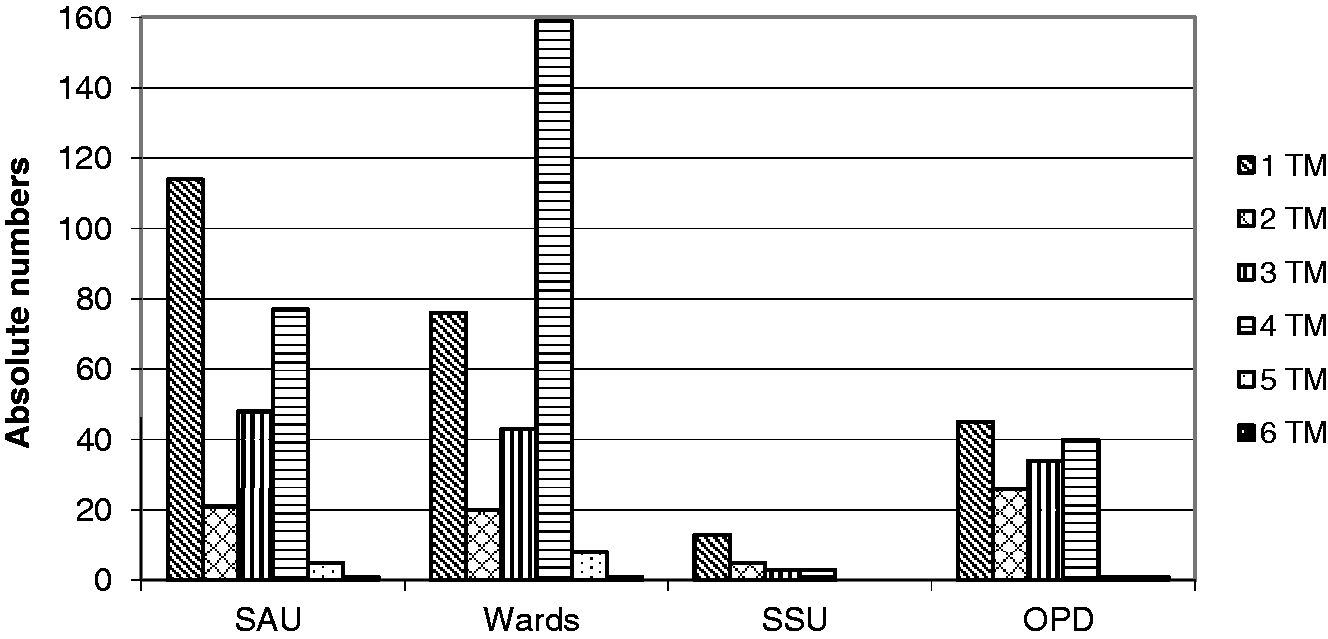
Comparison of the number of tumour marker and patient requests before (2009) and after (2010) implementation of guidelines.
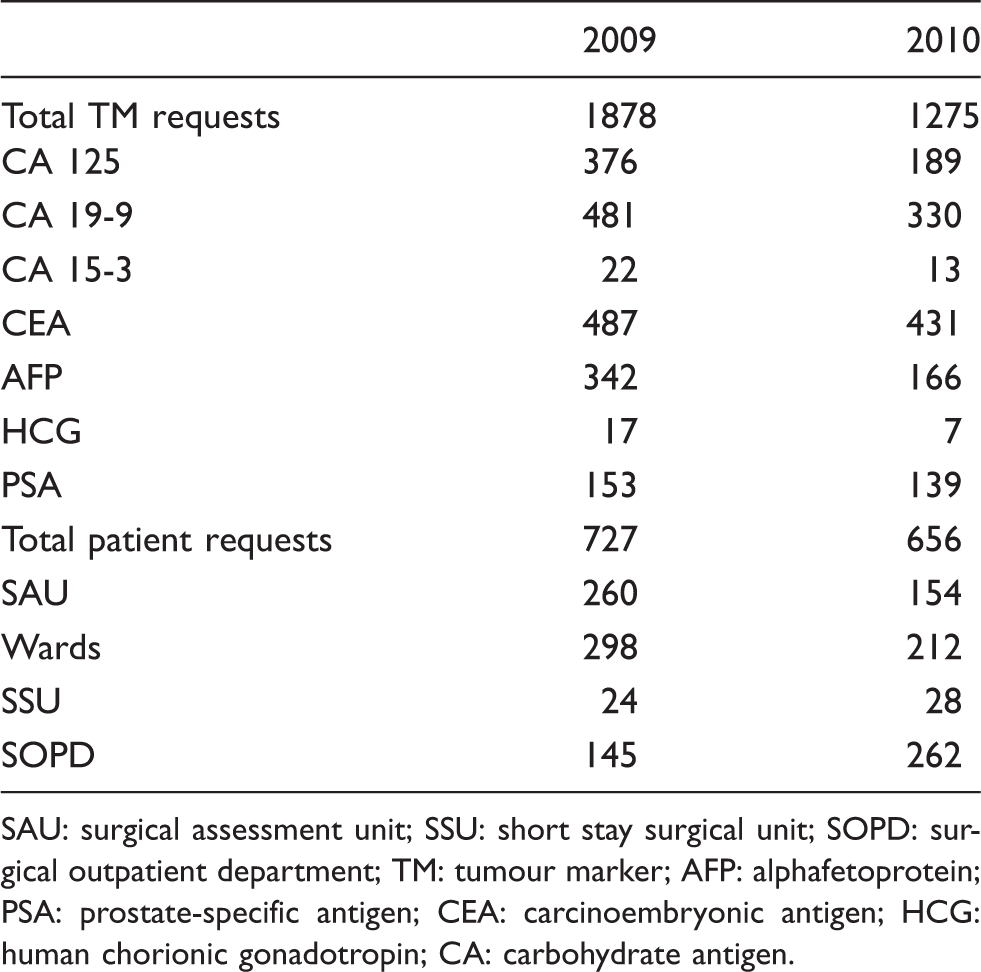
SAU: surgical assessment unit; SSU: short stay surgical unit; SOPD: surgical outpatient department; TM: tumour marker; AFP: alphafetoprotein; PSA: prostate-specific antigen; CEA: carcinoembryonic antigen; HCG: human chorionic gonadotropin; CA: carbohydrate antigen.
There was a significant decrease in the number of patients on whom panels of four or more TMs were requested from all locations, from 279 requests in 2009 to 60 requests in 2010 (Figure 2). Single TM requesting increased from all locations: 44% to 71% for SAU, 26% to 33% for the wards, 54% to 64% for SSU and 31% to 45% for SOPD (Figure 2).
Different panels as a percentage of total requests per location before (2009) and after (2010) implementation of local guidelines. SAU: surgical assessment unit; SSU: short stay surgical unit; SOPD: surgical outpatient department; TM: tumour marker.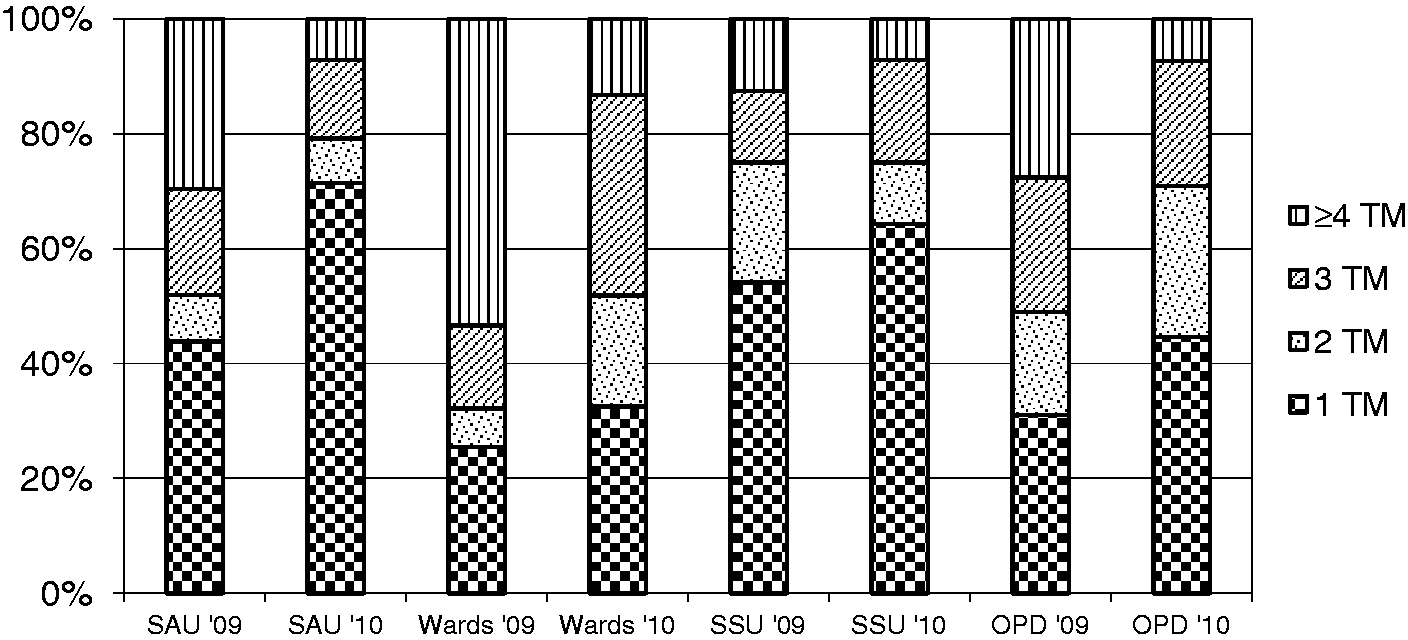
Two and three TM panel requests decreased from SAU and SSU (77 requests to 41 requests), but increased from SOPD and the wards (123 requests to 242 requests). Requests forms from these two locations were scrutinized in detail over a two-month period (June and July 2010). Of the 105 requests received from these two locations during this period, 47 (45%) were for two or three TM panels. Out of these 47 requests, 28% had illegible or no clinical details, 13% were for screening or diagnosis, 51% were requested in patients with a known malignancy but the TMs requested were either organ inappropriate or multiple TMs were requested not in keeping with the guidelines and 6% were requested in keeping with the guidelines.
The average number of TMs requested per patient decreased from 2.4 to 1.5 in SAU, 2.9 to 2.2 on the wards, 1.8 to 1.6 on SSU and 2.5 to 1.9 in SOPD.
The number of patients on whom five or six TMs were requested decreased from 17 to only one patient in 2010. In 2009, 123 out of the 376 (33%) CA 125 requests were on male patients. The number decreased to 14% in 2010.
During the 2010 audit period, 59 out of 1275 (4.6%) TM requests were rejected due to a breach in the five-day minimum retest interval.
Discussion
TMs are valuable adjuncts in patient care when used in the appropriate clinical setting. When used inappropriately they can be not only unduly alarming, resulting in further testing or investigation and patient anxiety, but also falsely reassuring. Despite international guidance2,3 inappropriate use continues to be a problem. A recent audit evaluating the appropriateness of TM requests from primary care found that up to 84% of multiple TM requests were inappropriate when audited against the National Academy of Clinical Biochemists guidance. 6 The most common reason for requesting a multiple TM panel was for screening of patients with non-specific symptoms such as weight loss or tiredness.
A survey of 28 clinical laboratories in Italy revealed that TM requesting patterns were neither influenced by type of hospital nor the availability of specialized oncology care. It also illustrated the informal and mostly poor communication between laboratories and users with regard to the correct use of TMs. Eighteen percent of the laboratories surveyed did not know whether clinical guidelines were in place or not. 7
A Northern Ireland audit found that 54% of TMs were requested to screen for suspected malignancy. 4 In 35% of cases, there was a low index of suspicion. Distribution of an information booklet containing guidelines and audit feedback failed to change requesting practice.
In our hospital, implementation of local requesting guidelines has had a significant effect on the TM requesting patterns of the General Surgery Department. Collaboration, rather than request restriction or prescription has resulted in local ownership by the users. Total patient requests decreased by 9.8%, whilst total TM requested decreased by 32%. This indicates that fewer TMs are now being requested per individual patient. Single TM requests increased and panels of four or more TM requests decreased from all locations.
Unexpectedly two and three TM panel requests increased from two locations, SOPD and the wards. In the SOPD, this was mainly due to the correct TM being requested for the purpose of cancer monitoring or follow-up but in addition to unnecessary markers not recommended by the guidelines. The reasons for this are unclear but may reflect a group of requestors who are either unaware of the guidelines or who are reluctant to change their practice. It was not possible to ascertain whether such multiple requests were made predominantly by junior or senior medical staff. These findings demonstrate the need for continuous education and audit focusing on these locations.
During the baseline 2009 audit period, the number of SAU requests exceeded SOPD requests. This was an unexpected finding given TM’s predominant role in monitoring and follow-up rather than screening and diagnosis. Following the implementation of the guidelines, SAU requests decreased by 41%.
A further problem identified by the baseline audit was the high number of requests for CA 125 on male patients. PSA requests on females were not identified as a problem. Thirty-three percent of all CA 125 requests in 2009 were on males. Papillary adenocarcinoma of the testis is an example of a rare indication for CA 125 monitoring in males, but this would not explain this high number of requests. This suggested that either the use of CA 125 is unfamiliar to requesters or that it is automatically included alongside other TM requested without thought. Although still not optimal, CA 125 requests on males decreased from 127 to 27 requests after the implementation of the guidelines. Since the re-audit we have set up our laboratory information system to automatically reject male CA15-3 or CA 125 requests, as well as female PSA requests.
After guideline implementation, less than 5% of TM requests were automatically rejected by the laboratory due to breaching the minimum retest interval, suggesting more considered requesting.
Conclusion
Improving the quality use of laboratory tests is an increasing challenge to clinical laboratories. The process of successful implementation of local guidelines would not have been possible without a collaborative effort between the Surgical and Medical Biochemistry Departments. The Surgical Department’s willingness to recognize factors leading to inappropriate requesting, and implement change, made it possible to implement a strategy to change requesting behaviour.
Although we did not evaluate whether changing TM requesting behaviour has affected patient management or outcome, the significant change in numbers that we have seen suggest that many TMs were inappropriately requested in the past.
Good interdepartmental relationships and local ownership by the users were key to agreement, acceptance and implementation of change in practice.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Guarantor
SZ.
Contributorship
DS-B, SZ and NK researched the literature. DS-B and SZ performed the two audits. NK and SZ produced the local guidelines. NK implemented the guidelines. DS-B wrote the first draft of the manuscript. All authors reviewed, edited and approved the final draft of the manuscript.