
Abstract
Background
Non-cardiac surgery is associated with major vascular complications and higher incidences of elevated plasma troponin (cTn) concentration. Goal-directed therapy (GDT) is a stroke volume (SV)-guided approach to intravenous (IV) fluid therapy that improves tissue perfusion, oxygenation and reduces post-operative complications. In patients undergoing major gastro-intestinal surgery, we compared high sensitive and contemporary troponin assays and correlated results with patient outcome.
Methods
Patients (n = 135) were randomized to receive IV fluid, guided by either the central venous pressure (CVP group, n = 45) or SV (± dopexamine inotrope, n = 45 per group). Serum was obtained pre- and post-operatively (0, 8 and 24 h) for troponin analysis by a prototype hs-cTnI assay (Abbott Laboratories), hs-cTnT (Roche Diagnostics) and contemporary cTnI (Beckman Coulter) assays.
Results
All troponin measurements were increased (P ≤ 0.05) post-operatively but there was no difference (P > 0.05) amongst treatments. Post-operative increases were reported more frequently (P ≤ 0.05) and earlier with hs-cTnI. Temporal increases (P ≤ 0.05) were reported in patients with and without complications for hs-cTnI/T assays but only in the complications group for cTnI measurements. Elevations ≥99th centile occurred most often (P ≤ 0.05) for hs-cTnT measurements but with similar frequency for both outcome groups (all assays). Only the hs-cTnI assay showed an increased relative risk of mortality (P ≤ 0.05) for elevations ≥99th centile
Conclusions
Our study may suggest a possible preference for the hs-cTnI assay in the peri-operative setting; however, our findings should be verified for larger cohort studies where emerging reference range data is incorporated for improving risk prediction with hs-cTn assays.
Introduction
Cardiac troponin T and I (cTnT and cTnI) are well-established cardiac-specific markers of myocardial cell damage. Superior sensitivity and specificity has augmented their universally preferred use, compared to other biomarkers, in the diagnosis of acute myocardial infarction (AMI). 1 Prognostic value can also be obtained from peri-operative troponin measurements, as shown for asymptomatic patients in the VISION study (Vascular Events in Non-cardiac Surgery Patients), where the peak post-operative cTnT concentration was reported to be significantly associated with 30-day mortality. 2 In this patient cohort, where major vascular complications and a higher incidence of cTnT elevations (>99th centile) are reported post-operatively, 3 such elevations were detected more readily using the high-sensitivity (hs) cTnT assay. The possibility of evolving myocardial injury may also be determined for those patients with post-operative troponin elevations showing a temporal increase of more than a defined relative change (%). Evaluating serial troponin measurements against such changes may be used to improve the differentiation of any troponin elevations due to acute coronary syndrome from those due to chronic disease and non-cardiac conditions. 4
The latest generation of hs-cTnT and cTnI assays now detect concentrations below the 99th centile with acceptable imprecision (CVs of ≤10%) and can therefore allow sub-clinical monitoring of possible myocardial remodelling and myocyte turnover. hs-cTn assays can also offer improved risk stratification by identifying patients with troponin concentrations greater than the limit of detection (LOD) but <99th centile, who are at an intermediate risk of major adverse cardiac events 5 and for whom intervention may alter risk and improve prognosis.
We have extended previous work in the surgical setting for a cohort of patients undergoing major gastro-intestinal surgery. Patients were assigned to one of three post-operative interventions, two of which involved the goal-directed therapy (GDT) technique for intravenous (IV) fluid delivery, with or without inotropic support (Dopexamine (DOP)), as described by Jhanji et al. 6 GDT involves the measurement of cardiac output or of closely related variables such as oxygen delivery or stroke volume as treatment end points for the administration of IV fluid and/or inotropic support. GDT has thereby been shown to improve tissue perfusion, oxygenation, and reduce post-operative complication rates by possibly preventing tissue oxygen debt and organ dysfunction. 7 The vasoactive agent DOP has both vasodilatory and inotropic properties which may be used additionally to improve microvascular flow and further ameliorate outcome. In the current study, serial troponin measurements were obtained using the hs-cTnT assay (Roche Diagnostics), a contemporary cTnI assay (Beckman Coulter) and a prototype hs-cTnI assay from Abbot Laboratories, which we verified initially. All assays were compared for the detection of any peri-operative changes, treatment effects as well as their prognostic utility including risk prediction.
Materials and methods
Subjects
This was a randomized, controlled, single-blinded intervention study involving adult patients (n = 135) who were admitted to the intensive care unit (December 2007 to February 2009) following major elective gastro-intestinal surgery at the Barts and the London NHS Trust Royal, UK. Patients with a known history of acute myocardial ischaemia or acute arrhythmias were excluded. Other exclusion criteria are described previously. 6
Ethical approval, consent and patient data
Details of ethical approval, consent, treatment allocations and clinical follow-up are described previously. 6 Approval for the analysis of cardiac markers at the Mater Misericordiae University Hospital (MMUH), Dublin (Ireland) was obtained from the hospital’s ethics committee. Single-blinded analysis of cardiac markers was achieved using pseudo-anonymized (coded) samples and the transfer of patient-specific information to the MMUH following sample analysis.
Clinical management: Intervention, monitoring and clinical outcome
Post-operatively, IV fluid therapy (8 h) was guided by measurements of central venous pressure (CVP: control group, n = 45) or stroke volume (SV). In this latter GDT group (n = 90), 0.5 µg/kg/min of DOP was infused in half of the patients (SV + DOP group: n = 45, SV – DOP group: n = 45). Details of all peri-operative therapeutic interventions, routine critical care, tissue perfusion and oxygenation monitoring have been described previously. 6 Assessment of patient outcome included recording the occurrence of any pre-defined post-operative complications (up to day 28): Renal (infection, acute kidney injury), gastro-intenstinal (paralytic ileus, ischaemia, anastomotic leak/stricture, peritonitis, infection [clostridium difficile], abdominal sepsis and GI haemorrhage), hepato-biliary (ischaemia, bile leak), respiratory (infection [pneumonia], pulmonary oedema/embolism, pleural effusion), circulatory (arrhythmia, angina, myocardial injury, cardiac arrest, heart failure, sepsis, shock and stroke), tissue (wound infection, haematoma). Mortality within 28 days (short term) and 180 days (intermediate term) of surgery was also recorded.
Blood and plasma collection
Patient blood (20 mL) was collected into serum separator tubes (Becton Dickinson, Cowley, UK) at several time points: pre-operatively, at baseline (0 h) and at 8 and 24 h post-operatively. Blood was centrifuged at 10,000 g, for 10 min, at room temperature. Serum was aliquoted and stored (−70℃) until analysis.
Laboratory methods (troponin analysis)
Assay specifications
Assay specifications for cTnI, hs-cTnT and prototype hs-cTnI assays.
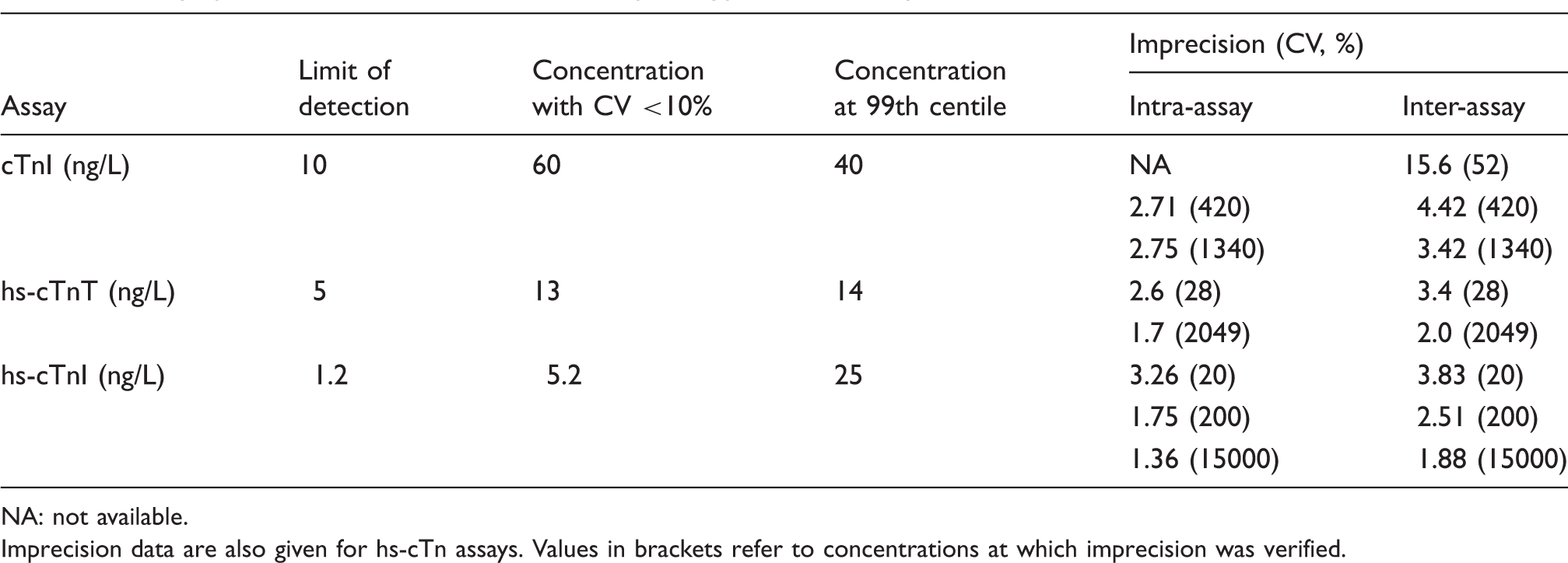
NA: not available.
Imprecision data are also given for hs-cTn assays. Values in brackets refer to concentrations at which imprecision was verified.
Sample analysis
Patient samples were mixed for 30 min (Rotamix) while thawing at room temperature (r.t.p.). Samples were centrifuged (10,000 g, 10 min at r.t.p.) and the supernatant was transferred to a secondary tube which was vortex-mixed before analysis.
Assay reference ranges
The manufacturer’s quoted 99th centile concentrations were used for the hs-cTnT and cTnI assays (Table 1). For the hs-cTnI assay, a 99th centile concentration of 25 ng/L was used. This was established in our laboratory from a different cohort of cardio-healthy patients (n = 109) comprising 66 males and 43 females (median age [inter-quartile range (IQR)] of 37 years [29–49]), who were selected following a cardiology consult and with normal electrocardiography and echocardiography results (McGorrigan C, personal communication, January 2011). Data were assessed for normality (D’Agostino + Pearson omnibus test), and non-parametric analysis was used to determine the 99th centile concentration (Graphpad software, version 5).
Statistical analysis
Normality was assessed by the D’Agostino and Pearson omnibus test. The Student’s t-test was used for parametric data and the Wilcoxon Signed Rank or Mann-Whitney U tests (two-tailed) for non-parametric data. For non-parametric comparisons involving more than two groups, Friedman and Kruskal–Wallis tests were used for paired and unpaired observations, respectively, followed by Dunn’s Multiple Comparison test. Spearman rank was used for all data correlations. Troponin measurements were correlated to post-operative complications using logistic regression analysis. Categorical variables were analysed in contingency tables using Fisher’s exact test and was used to calculate the relative risk of mortality (days 28 and 280) associated with peak peri-operative troponin measurements. P ≤ 0.05 was considered significant for all analysis. For hs-cTnT measurements, data were adjusted (+7 ng/L for concentrations 3 to <8 ng/L; +5 ng/L between 8 and 20 ng/L) to reflect results obtained using reformulated new calibrated reagent lots. 8 Short-term increasing reference change values (RCVs) (log-normal), of 90% and 69% for the hs-cTnT and hs-cTnI assays, respectively, were used as described previously.9,10 Data were analysed using Prism (Graphpad software, version 5), Excel (Microsoft Office, 2007) and Medcalc (version 12.1.4).
Results
Verification of the hs-cTnT and hs-cTnI assays
Both assays showed acceptable imprecision (CV ≤10% [hs-cTnT], CV ≤5% [hs-cTnI]) for the range of concentrations assessed, including those comparable to the 99th centile (Table 1).
Patient outcome
The incidence of complications was similar (P ≥ 0.05) for each treatment group (67% [CVP], 58% [SV] and 69% [SV + DOP] of patients). Intra-operative tachycardia occurred more frequently (31% of patients) for the SV + DOP group (P ≤ 0.05, 4% and 8% of patients in the CVP and SV groups); however, the incidence of cardiac complications was similar across treatment groups (9% [CVP], 7% [SV ± DOP]).
Correlation of pre-operative troponin measurements with age and sex
Age- and sex-related differences in concentration were observed only for the hs-cTnT assay (Figure 1). Only 5% of patients aged ≤60 years (n = 2/36) had cTnT concentrations ≥the 99th centile compared to 55% (n = 52/99) of patients >60 years. The median (IQR) cTnT concentration was higher (P ≤ 0.01) for males (13.8 ng/L, [10–18.8 ng/L]) than females (10.2 ng/L, [10–14.3 ng/L]). For only one patient were pre-operative concentrations ≥respective 99th centile for all troponin measurements.
Pre-operative concentrations of cTnI (a), hs-cTnT (b) and hs-cTnI (c) for all patients. Median (inter-quartile range) age = 67 (60–76) years. The dashed line on each graph corresponds to the 99th centile concentration for each assay. Data were analysed using Spearman’s Rank correlation.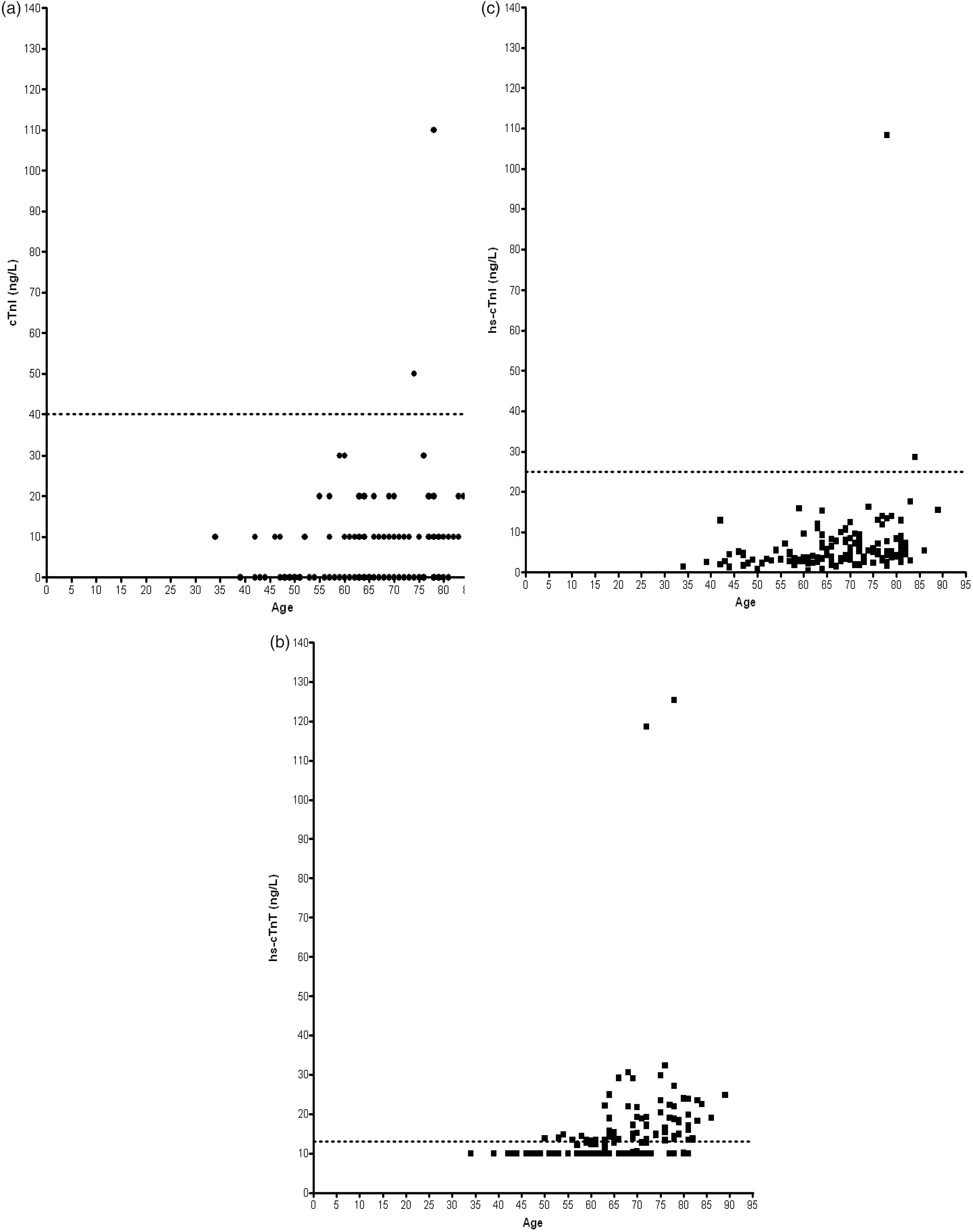
Changes in post-operative troponin measurements: Effect of time and treatment
For all treatment groups, troponin concentrations were greater (P ≤ 0.05) at 24 h post-operatively, compared with pre-operative measurements (Figure 2) but there was no treatment differences (P > 0.05). Significant changes (P ≤ 0.05) from pre-operative measurements were reported earliest (at 0 h) for the hs-cTnI assay, irrespective of treatment.
cTnI (a-c), hs-cTnT (d-f) and hs-cTnI (g-i) measurements for CVP, SV and SV + DOP groups. Within each group, troponin concentrations were compared at each time point using Friedman and Dunn’s post-test analysis. Data are presented as the mean ± S.E.M. Dashed lines correspond to the 99th centile. *P ≤ 0.05, **P ≤ 0.01, ***P ≤ 0.001 vs. pre-op, #P ≤ 0.05, ##P ≤ 0.01, ###P ≤ 0.001 vs. 0 h.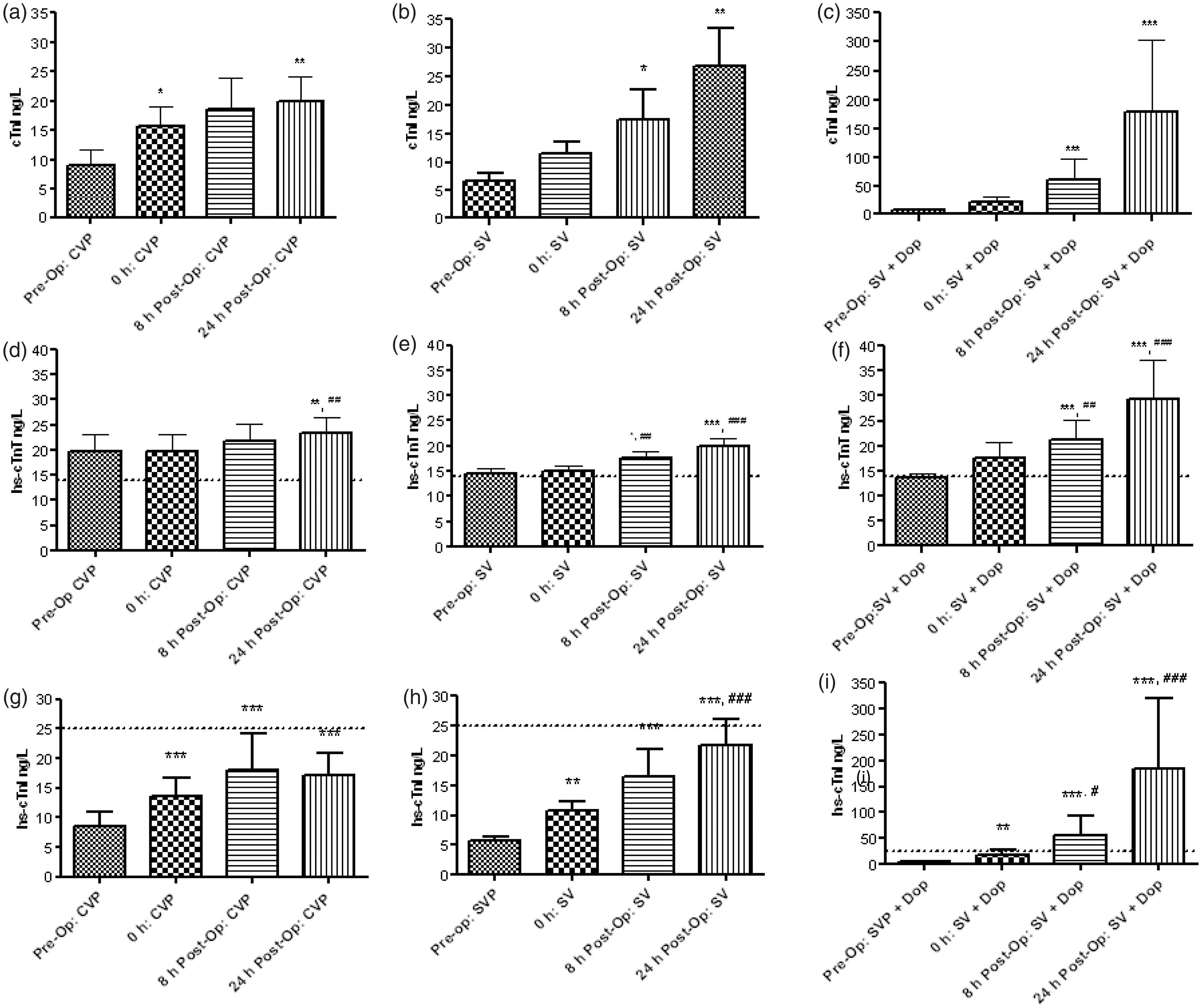
Characteristics of post-operative troponin changes and evaluation of measurements against the 99th centile
Peri-operative troponin changes and frequency of troponin elevations ≥99th centile.
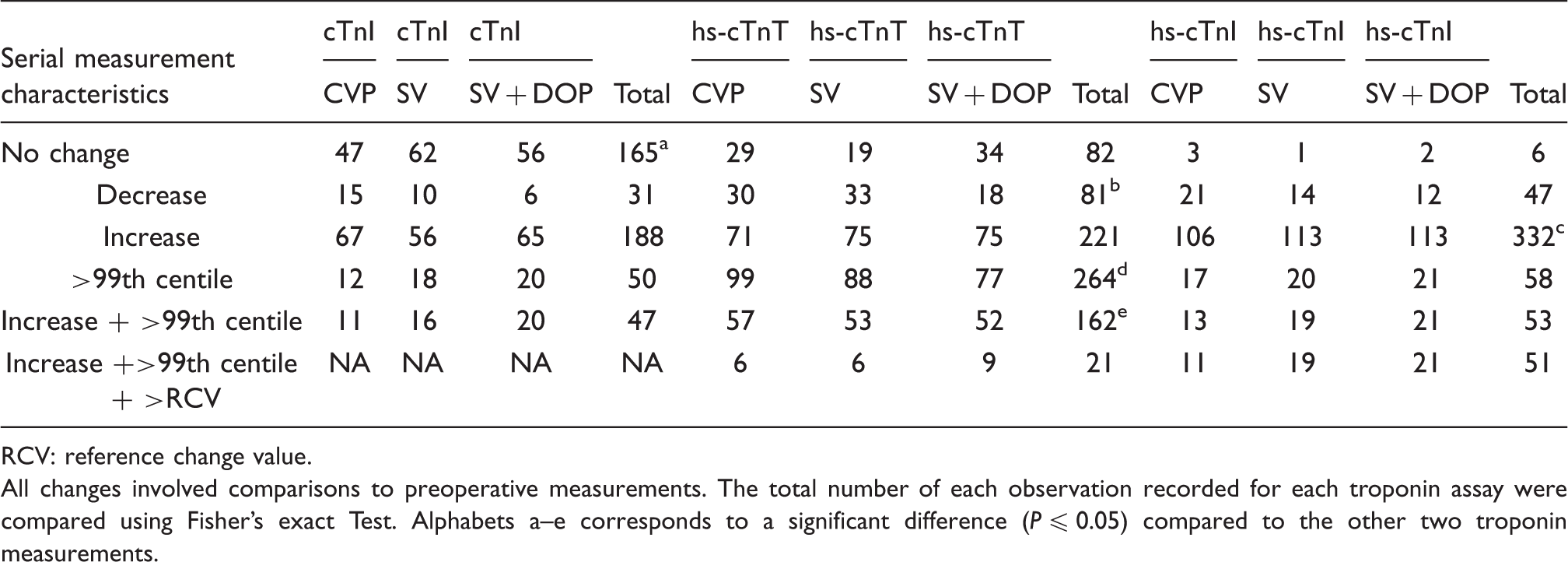
RCV: reference change value.
All changes involved comparisons to preoperative measurements. The total number of each observation recorded for each troponin assay were compared using Fisher’s exact Test. Alphabets a–e corresponds to a significant difference (P ≤ 0.05) compared to the other two troponin measurements.
Peri-operative troponin increases from pre-operative concentrations, to ≥the 99th centile (at one or both time points), occurred most frequently (P ≤ 0.05) for hs-cTnT (n = 162) and least so (P ≤ 0.05) for cTnI (n = 47) measurements (Table 2). Only 13% (21/162) of such hs-cTnT elevations were ≥the RCV whereas 96% of such hs-cTnI increases were also ≥the respective RCV. Troponin increases to ≥the 99th centile were again reported most frequently for the SV + DOP group, for hs-cTnI and cTnI assays.
Peri-operative troponin measurements and outcome
Temporally significant troponin increases (P ≤ 0.05) were observed for high-sensitivity assays, irrespective of outcome and occurred earliest (0 h) for hs-cTnI (Figure 3). For cTnI, only patients with complications showed significant increases, from 0 h onward. All troponin measurements tended to be higher at 24 h post-operatively for patients with than without post-operative complications in the GDT groups (Figure 3), particularly in the SV–DOP group (P ≤ 0.05).
Troponin analysis for patients with (striped bars) and without (solid bars) post-operative complications. Data are presented as the mean ± S.E.M. For combined treatment groups (top panel), times points were compared by Friedman (Dunn’s post-test) and between outcome groups by two-way ANOVA (Bonferroni post-test) analysis. *P ≤ 0.05, **P ≤ 0.01, ***P ≤ 0.001 vs. pre-op within each group. ##P ≤ 0.01 vs. 24 h (non-complications).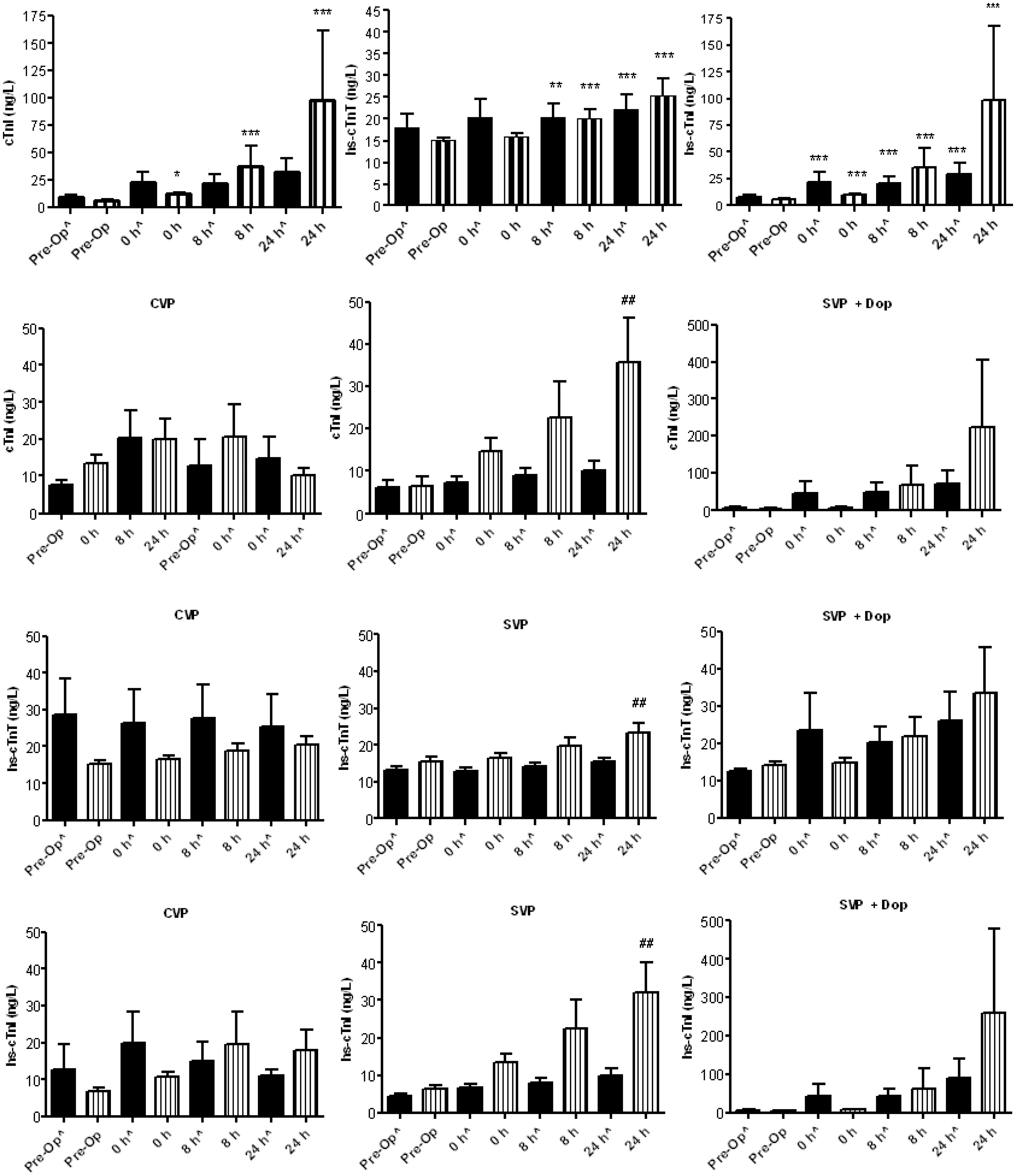
Summary of peak peri-operative troponin observations evaluated against the limit of detection (LOD) and 99th centile for patients presenting with and without complications.
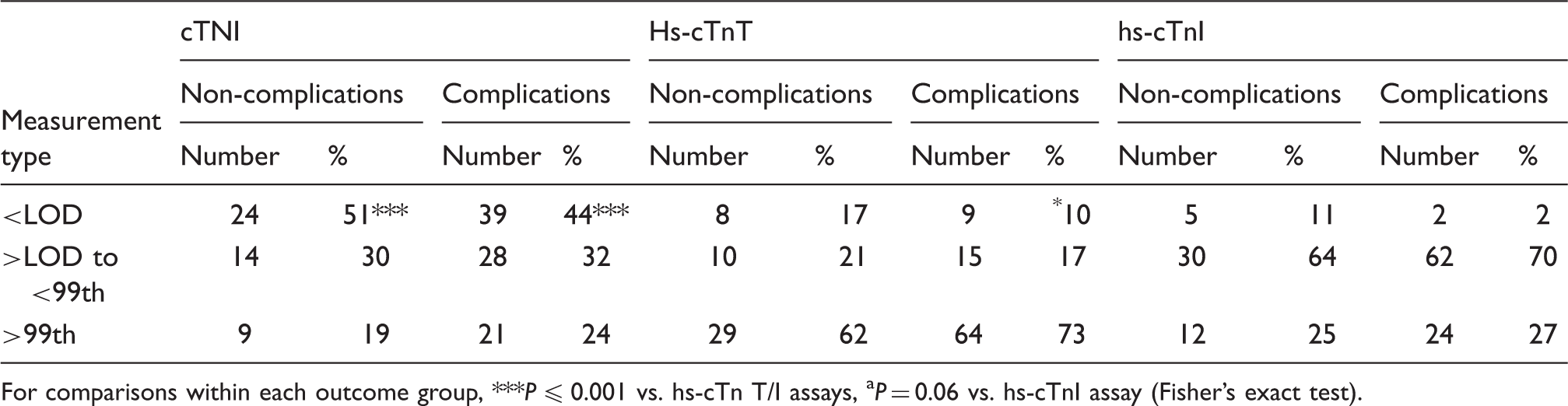
For comparisons within each outcome group, ***P ≤ 0.001 vs. hs-cTn T/I assays, aP = 0.06 vs. hs-cTnI assay (Fisher’s exact test).
For the hs-cTnI assay, the relative risk (RR) of mortality within 28 days (3.67 [CI: 1.37–9.8]) and 180 days (2.06 [CI: 1.08–3.93]) of surgery was significantly greater (P ≤ 0.05) for patients with a peak troponin concentration ≥99th centile. This was also true for unadjusted hs-cTnT measurements (28 days: 2.94 [CI: 0.97–8.92]; 180 days: 2.12 [CI: 1.06–4.25]) but not when data were adjusted to reflect reformulated, new calibrated lots. For cTnI, the RR only trended to significance over both time periods (28 days, P = 0.08: 2.62 [CI: 0.99–6.98], 180 days, P = 0.07: 1.94 [CI: 1.01–3.75]).
Discussion
In a cohort of patients undergoing major gastro-intestinal surgery, troponin was measured peri-operatively using a prototype hs-cTnI assay and compared to contemporary cTnI and hs-cTnT assays. Post-operative increases were reported more frequently with the hs-cTnI assay and although all assays showed temporally significant increases, these occurred earliest for the hs-cTnI assay. Significant changes were reported irrespective of post-operative outcome for hs-cTnI (and hs-cTnT) measurements but only in patients with complications using the cTnI assay. Although this may indicate discriminatory capability for the contemporary cTnI assay, only the hs-cTnI assay showed a significantly increased relative risk of mortality for elevations ≥99th centile. Measurements ≥99th centile were more frequent for the hs-cTnT assay but are likely confounded by age- and sex-related differences.
Effects of GDT
In an earlier report from this study, 6 improvements to oxygen delivery, microvascular flow and tissue oxygenation were observed for patients receiving stroke volume (SV)-guided fluid and DOP (SV + DOP group). SV-guided therapy alone gave modest improvements in microvascular flow. Authors reported a possible improvement in renal function for both GDT groups (SV ± DOP) compared to the CVP-guided fluid group. Perhaps consistent with its beta adrenoreceptor effect, intra-operative tachycardia occurred most frequently in the SV + DOP group. The incidence of cardiac complications was equal for both GDT groups. GDT did not reduce the overall complication rate in this study in contrast to previous similar studies; however, this study was not powered to identify differences in clinical outcomes. We did not find any significant treatment effect on troponin concentration, as Jhanji et al. 6 reported for serum inflammatory markers. This latter observation does not support a role for cardiac output-guided haemodynamic therapy in favourably influencing the systemic inflammatory response to tissue injury.
Age- and sex-related effects with high-sensitivity troponin assays
From pre-operative troponin measurements, age- and sex-related (male > female) differences were observed for the hs-cTnT assay (only) and agrees with previous reports.11,12 Only 5% of patients ≤60 years of age had cTnT concentrations ≥the 99th centile, compared to 55% of patients aged >60 years. Studies by Koerbin et al. 11 similarly reported a higher median cTnT for patients ≥60 years of age. Despite such demographic effects, we used only a single 99th centile concentration for the hs-cTnT (and cTnI) assays, as quoted by the manufacturer. When our laboratory previously established the 99th centile concentration (25 ng/L) for the hs-cTnI assay, age- or sex-related differences were not observed. Sex-related effects are though reported elsewhere for this hs-cTnI assay, involving larger cohorts of subjects powered to detect gender differences. 13 Our 99th centile is though in good agreement with the Gutenberg Health Study (n = 4139) 14 where a 99th centile of 24 ng/L was obtained, after excluding individuals with elevated N-terminal B-type Natriuretic Peptide (>95th centile).
The effect of patient demographics reported using high-sensitivity troponin assays has raised concern regarding the correct interpretation of results, as part of the diagnostic options for patients presenting with ACS and in other clinical uses including the current setting. Rigorous definition of population reference ranges by age, sex and ethnicity has been proposed 15 with selection of cardio-healthy individuals based on physical examination, cardiac history, electrocardiogram and chest X-ray. 16 hs-cTn measurements are also required for patients who are clinically stable, with cardiovascular (CV) risk factors but no acute CV disease. Although such studies would be demanding, the information provided should promote optimal deployment of high-sensitive assays and reduce potentially inappropriate investigations.
Peri-operative troponin monitoring
The Vascular events In non-cardiac Surgery patients cOhort evaluatioN (i.e. VISION) involves the study of patients with vascular complications following non-cardiac surgery. This study has recently reported a significant association between the peak post-operative cTnT concentration and mortality, within 30 days of surgery. 2 This significant finding underpins the latest consensus on the universal definition of myocardial infarction, which recommends routine monitoring of cardiac biomarkers in high-risk patients, pre- and post- (48–72 h) major surgery. 17 In a sub-study of the VISION cohort, a higher incidence of cTnT elevations (>99th centile) was also reported in patients post-surgery and was detected more frequently using the hs-cTnT assay than its less-sensitive predecessor. 3 In our intervention study, we have extended work involving non-cardiac surgery patients, through a three-way comparison of hs-cTnT, cTnI and hs-cTnI assays and correlation of data to post-operative complications and mortality. Consistent with the findings by Kavsak et al., 3 we also report higher troponin concentrations post-operatively, irrespective of troponin measurement or treatment group. Temporally significant troponin increases were observed for all assays but occurred earliest for the hs-cTnI assay. This finding may offer potential translation to therapeutic and prognostic benefit.
In our study, post-operative troponin increases were also reported most often for hs-cTnI and least so for the cTnI assay where no detectable change was reported most frequently. These findings are supported by another study by Kavsak et al., 18 involving patients with ACS, where increases (significant) were reported more frequently for the hs-cTnI assay (Beckman Coulter) compared to the contemporary cTnI assay used currently, particularly for concentrations <99th centile. The ability of high-sensitivity assays to detect troponin at concentrations between the LOD and the 99th centile can offer additional prognostic value and risk stratification compared to less sensitive assays, by identifying patients who are at an intermediate risk of future cardiac events. 5
Troponin evaluations against the 99th centile and the RCV
Unlike the earlier report by Jhanji et al.,6 where inflammatory markers were not evaluated against respective reference ranges, in the current study we considered all troponin measurements against each assay’s 99th centile concentration. Such elevations were reported most frequently for the hs-cTnT assay, even prior to surgery, and are likely influenced by the age- and sex-related effects on concentration. By comparison, the hs-cTnI and cTnI assays were in closer agreement with each other, for all treatment groups, and showed discordant treatment effects compared to hs-cTnT measurements. These findings imply that assay concordance was dependent on the analyte, not assay sensitivity. Disparity between cTnT and cTnI assays is not an isolated finding since in a previous study of dialysis patients, cTnI was elevated (≥99th centile) less frequently (and less predictive of outcome) than cTnT. 19 In a subsequent study,20concordance between cTnT and cTnI assays was shown to be concentration-dependent and better for comparisons at the LOD than at higher concentrations (i.e. CVs ≤10%). Authors also described how agreement between commercial cTnI immunoassays for predicting outcome was dependent on the epitope specificity of capture and detection antibodies. By contrast with the present study, there were no comparisons at the respective 99th centile concentration. When we examined only those patients showing troponin increases from pre-operative values, to ≥99th centile concentration, again such increases were reported most frequently for the hs-cTnT assay. However, any assay comparisons at the 99th centile must be interpreted with caution since the cTnI assay does not achieve desirable imprecision (i.e. ≤10% CV) at this threshold concentration.
High sensitivity cardiac troponin assays are well documented for their ability to show evolving myocardial injury earlier than less sensitive assays and show greater diagnostic sensitivity even for baseline measurements.18,21,22 However, since troponin may be raised in acute and chronic conditions affecting the myocardium, and by cardiac or non-cardiac related mechanisms, it is conceivable how this increased sensitivity may be offset by reduction in diagnostic specificity
Peri-operative troponin and outcome
Previous studies have shown that any troponin increase is associated with worse patient outcome 24 and higher risk for subsequent adverse events. 5 In the present study, troponin concentrations tended to be higher for patients with than without complications after 28 days of post-operative follow-up. However, logistical regression analysis did not show significant correlation of any troponin measurement to outcome. Patients showing peak elevations ≥the respective LoD or 99th centile concentration (at ≥1 time point) were also similar between outcome groups, for all measurements, implying that troponin elevations were not predictive of such short-term outcome measures. However, when we considered the incidence of mortality within 28 days (10%) and 180 days (21%) of surgery, troponin concentrations ≥99th centile were associated with a significantly greater risk of mortality but only for hs-cTnI measurements. This finding should though be verified for a larger cohort of patients. Although statistical significance was not obtained for the cTnI assay, a recent meta-analysis involving vascular surgical patients and measurements with contemporary cTnI assays show elevations (≥99th centile) to be strongly predictive of all cause mortality at 30 days post-surgery. 25 Our data support the recent recommendation 17 for routine post-operative troponin monitoring of patients post-surgery and the requirement for intervention studies to examine any potential for risk reduction in patients with post-operative troponin elevations.
In conclusion, peri-operative troponin increases were detected earlier using the hs-cTnI assay which may potentially confer therapeutic and prognostic advantage with this assay. Although the cTnI showed discriminatory capability over both hs-cTn assays for patients with and without complications, only the hs-cTnI assay predicted a significant risk of mortality for peak troponin elevations ≥99th centile. For hs-cTnT measurements, age- and sex-related effects possibly preclude the reliable routine use of a single 99th centile concentration and exemplify the need for reference range studies to inform optimal deployment of hs-cTn assays together with use of RCVs for serial measurements to enable appropriate patient stratification and intervention.
Footnotes
Acknowledgements
We thank Ms Kathleen Cafferkey and Mr Conor Russell (Department of Clinical Biochemistry + Diagnostic Endocrinology, MMUH) for their technical support. SJ acknowledges UK National Health Service funding to the Royal Marsden/Institute of Cancer Research National Institute for Health Research Biomedical Research Centre.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
London Multi-Centre Research Ethics Committee, Medical and Healthcare products Regulatory Agency (UK), Mater Misericordiae University Hospital Ethics Committee, Trial registration number: ISRCTN 94850719.
Guarantor
MF.
Contributorship
GL wrote the manuscript; HT was involved in analysing patient samples and GL was involved in data analysis; RMP and MF were involved respectively in conceiving the interventional protocol and analytical components of the study; SJh and RMP were involved in ethical approval, patient recruitment and collating patient data. SJa assisted patient data analysis. All authors reviewed and edited the manuscript and approved the final version of the manuscript.