
Abstract
A 72-year-old woman presented with suspected parkinsonism and discolouration of the skin especially on sun-exposed areas. Thorough investigation revealed systemic zirconium intoxication due to intake of metallic colloids as a home remedy as a cause of the skin colour change. There may be an association between skin discolouration and her parkinsonism. This is unique in that various clinical manifestations developed following systemic ingestion of zirconium and this should serve as a warning on the risk of taking illicit dietary supplements.
Introduction
Zirconium is a lustrous, noncorrosive metal that resembles silver. It is mainly used for industrial purposes as a pure metal or alloy. 1 Zirconium is known to cause granulomatous lesions in the lung and skin.1–3 Colour changes in the skin are a not uncommon complication of cutaneous deposition of metallic particle of various aetiologies. Argyria is skin discolouration following the accumulation of silver substrate in the dermis. In this paper, we describe a patient who took illicit metallic colloids as a home remedy and presented with typical argyria mimicking skin manifestation and dopamine transporter imaging negative parkinsonism. We suggest that these findings were associated with systemic zirconium intoxication.
Case report
A previously healthy 72-year-old woman presented to our clinic with complaints of tremor and slowness of the body, which began three months previously. Neurologic examination revealed a bilateral resting tremor, rigidity and bradykinesia that are compatible with a diagnosis of parkinsonism (Unified Parkinson’s Disease Rating Scale part III motor score of 29, Hoehn and Yahr stage 2.0).
4
While not remarked upon by the patient herself, striking, widespread blue-grey discolouration of the skin and nails was visible. Physical examination showed that the discolouration of the skin was accentuated on the face and in the suprasternal notch and was prominent on sun-exposed areas with hand and nails (Figure 1(A) and (B)). The gums, oral mucosa, extremities, trunk and gastric mucosa were also affected (Figure 1(C)). The patient denied having any medical illness or taking any medication other than homemade silver-powder colloids daily for 12 months as a home remedy. She had discontinued the use of colloids due to gastric discomfort 18 months previously. Colour change of the skin and mucosa began one year prior to presentation and had progressed. She had no history of industrial employment or exposure to other toxic materials. She denied taking any kinds of medications that might cause systemic dopamine inhibition. Routine laboratory analyses of the serum and urine were all within the reference range.
Blue-grey discolouration of the skin, especially on sun-exposed areas (A) and on the hand and nails (B) (left: control subject). Colour change was detected in the gastric mucosa on gastroscopy (C).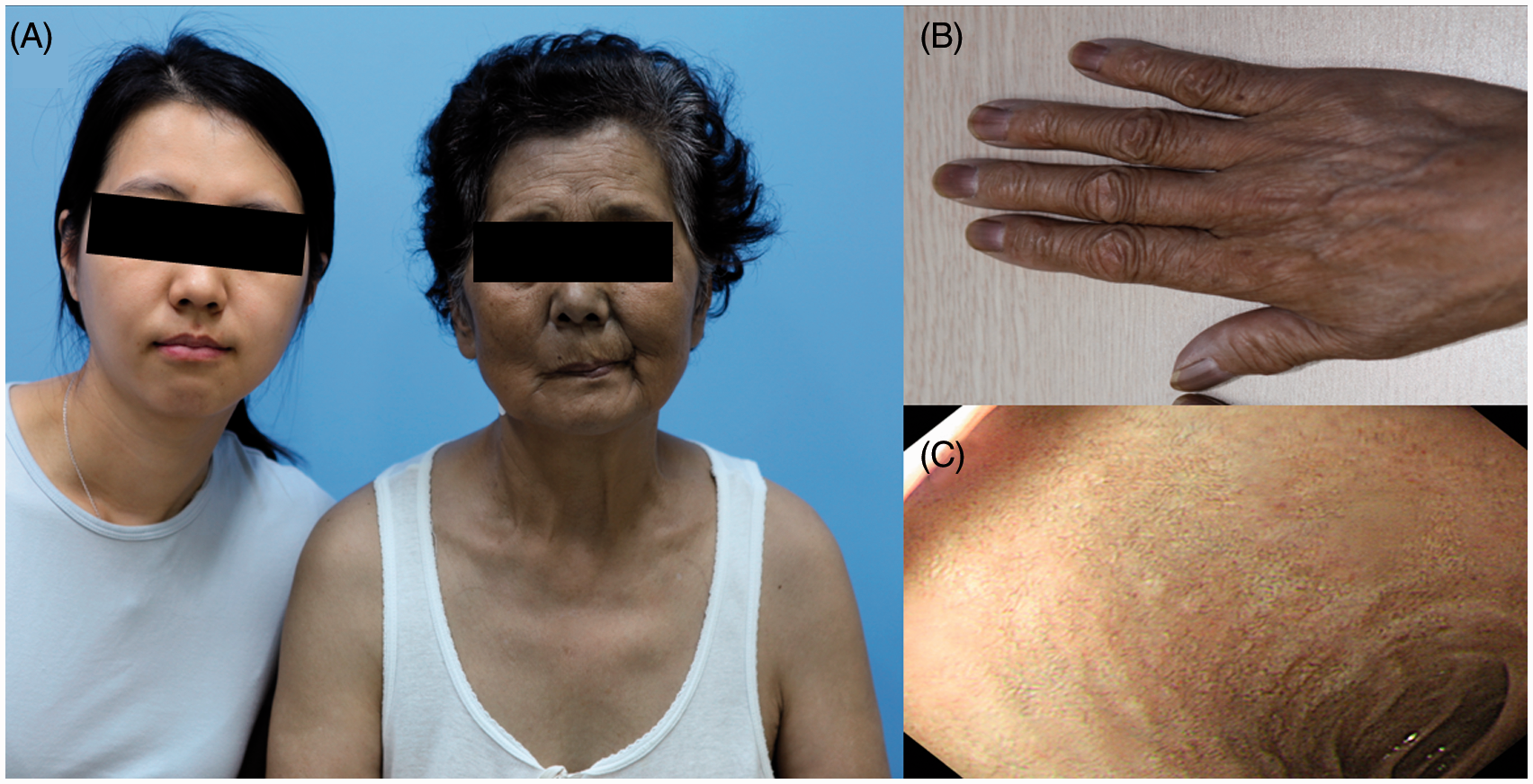
Magnetic resonance imaging of the brain was unremarkable other than mild age-related atrophy. Dopamine transporter (DaT) positron emission tomography performed to evaluate her parkinsonism was normal, with symmetric distribution of uptake in bilateral striatum. There was no clinical improvement of her parkinsonism despite maintenance of dopaminergic medications.
At first, we suspected typical presentation of silver intoxication based on her history and the typical skin discolouration. However, heavy metal toxicological study including the measurement of silver (Ag+), manganese, copper, mercury, aluminium, zinc and lead concentrations in the serum and urine were all within the reference range. Oxygen saturation, carboxyhaemoglobin and methaemoglobin concentrations were also unremarkable.
Light microscopy examination of a skin punch biopsy from the right neck revealed fine, small brown–black granules in the basement membrane of the eccrine glands and hair follicles and some melanophages in upper dermis. These findings were consistent with findings of argyria (Figure 2(A)). Scanning electron microscopy (SEM; S-4700, Hitachi, Tokyo, Japan) showed granule deposition in the eccrine glands and hair follicle (Figure 2(B)). SEM with energy-dispersive X-ray analysis (EDX; X-Max, Horiba, Japan) was performed to characterize the small granules, which demonstrated peaks for zirconium but not for silver (Figure 2(C)). Based on this result, we confirmed the diagnosis of zirconium intoxication as the cause of her skin discolouration. We assumed that the zirconium deposition might be associated with her parkinsonism as there were no dopaminergic deficits on DaT scan, nor was there a response to dopaminergic medications, and the onset of bilateral parkinsonism was relatively rapid compared to idiopathic Parkinson’s disease.
Histologic examination of a skin biopsy from the neck showed tiny brownish-black particles around eccrine glands (A) and tiny particles on scanning electron microscopy (B). Energy dispersive X-ray analysis revealed peaks for zirconium (white arrow) (C).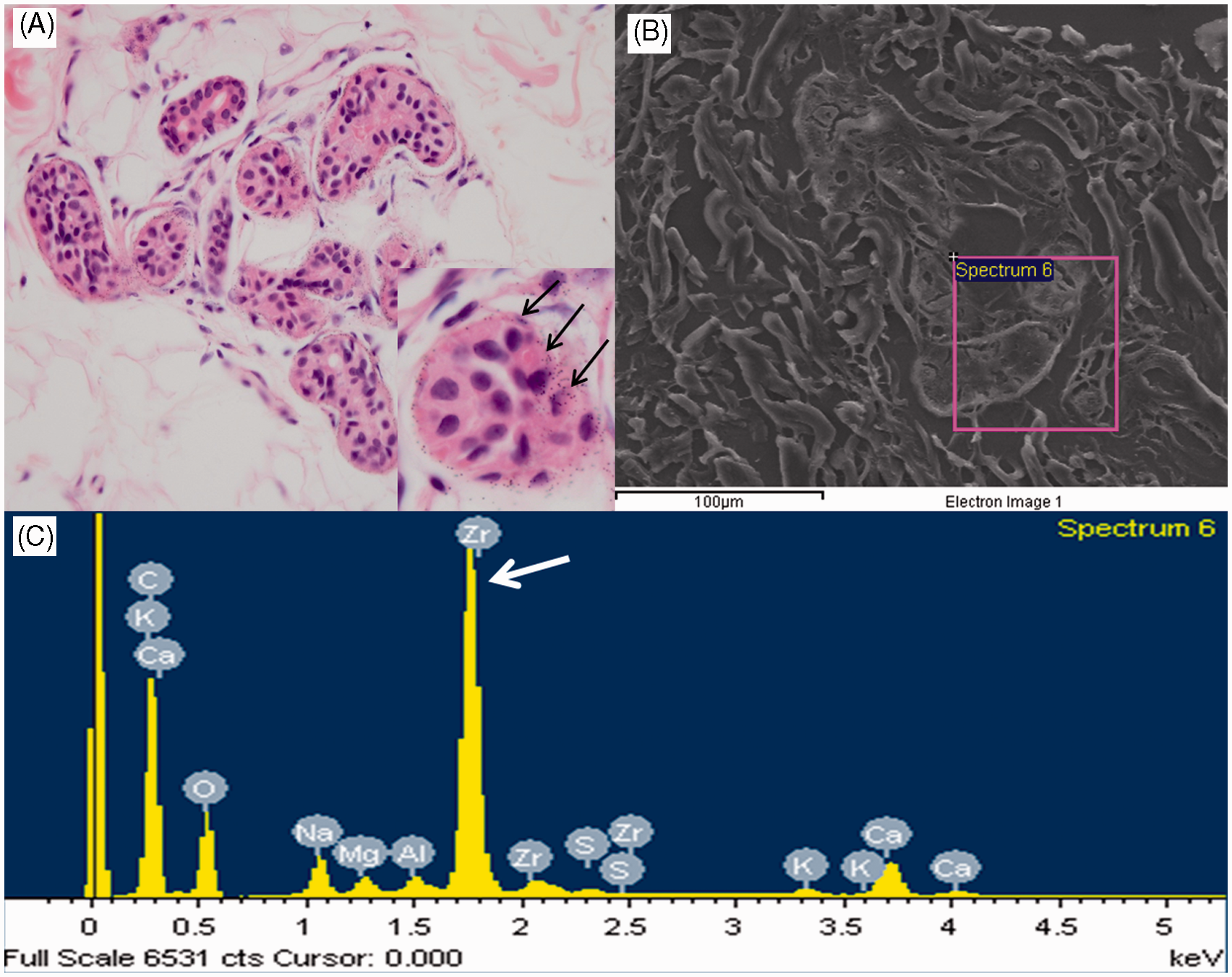
Discussion
Because of the belief that drinking silver is an effective remedy for various diseases, many people worldwide still take silver-containing dietary supplements. Thus, argyria as a result of taking silver-containing supplements has been reported many times.5–11 Because of the striking appearance of the blue-grey discolouration of sun-exposed area, argyria is easily suspected clinically. However, causative agents should be confirmed by analysis of EDX through SEM examination. The first clinical impression of the presenting case was argyria due to the typical skin discolouration, biopsy findings of tiny brown-black particles in the basement membrane region of the eccrine glands and hair follicles, and a history of consumption of colloidal silver. Although the Food and Drug Administration has issued a warning to consumers about the risk of developing argyria when taking silver-containing dietary supplements, 12 the ingestion of colloidal silver appears to be increasing among patients using alternative medicine. This patient also believed that the colloidal silver (in fact, zirconium) was a ‘cure-all’ and drank what she thought as silver liquids whenever she was tired. A major problem with alternative medicines and homemade remedies is that the exact composition is often uncertain. The colloids that this patient took did not contain silver, but rather zirconium. The impact of zirconium on human health has not been well investigated. There was one report of a woman who worked in the nuclear industry and was exposed to zirconium who developed granulomatous pulmonary, breast and axillary lymph node change. 1 Granulomata induced in the axilla due to the use of zirconium-containing deodorant was occasionally reported prior to its use in deodorants being banned in 1978.2–3,13 This case is unique in that systemic zirconium intoxication was associated with skin discolouration and parkinsonism, as confirmed by peaks for zirconium on SEM/EDX. The skin manifestations of this case resemble typical argyria: blue-grey discolouration of the skin and mucosa that is most prominent in sun-exposed areas and involvement of the nail. A blue-grey skin colour can develop from deposition of heavy metals other than silver, such as gold, mercury, bismuth, arsenic and lead. This patient denied any other exposure to those heavy metals, and serum/urine heavy metal concentrations were unremarkable, with no associated peaks on SEM/EDX.
This patient had clinical findings compatible with a diagnosis of possible Parkinson’s disease at her initial clinic visit. However, since there were no dopaminergic deficits on DaT scan, there was no proper response to dopaminergic medications and the onset of parkinsonism was relatively sudden and bilateral with rapid progression, secondary parkinsonism was suspected instead of idiopathic Parkinson’s disease. Heavy metal poisoning is a well-known cause of secondary parkinsonism. Similar to our patient, manganese-induced parkinsonism does not involve degeneration of midbrain dopamine neurons on DaT scan, and dopaminergic drugs are not an effective symptomatic treatment. 14
In the present case, the assumption that systemic zirconium intoxication caused her parkinsonism was reasonable because there were no structural abnormalities on brain imaging, no evidences of inflammation of the nervous system, no exposure to other neurotoxic agents and no history of taking medications that could block dopaminergic transmission. Furthermore, the timing of the development of symptoms correlated with the ingestion of the homemade remedy. However, since the exact composition of the ingested colloid was uncertain, it is possible that other components caused the symptoms and clinical signs observed.
To the best of our knowledge, this is the first report of both skin discolouration secondary to dermal deposition of zirconium and parkinsonism as neurological manifestation following zirconium ingestion. This should serve as a warning of the risk of taking illicit dietary supplements, and physicians should know there are various aetiologies for argyria type skin discolouration. Further studies are needed to elucidate the nature of the presumed zirconium-induced neurological manifestation.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This study was supported by a Korea University Grant in performing Laboratory study.
Ethical approval
The written informed consent from the patient has been obtained.
Guarantor
D-YK.
Contributorship
HJR: wrote first manuscript, researched literature and conceived the study; SJY: patient recruitment and searched manuscript; J-TP: protocol development and data analysis; YHK: data analysis; JMJ: data collection and researched literature; M-HP: conceived the study; D-YK: structured manuscript, wrote and revised manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.