
Abstract
Background
Thiopurine methyltransferase (TPMT) enzyme activity is measured before initiating thiopurine therapy to reduce the risk of severe drug-associated myelotoxicity in patients with low enzyme activity. TPMT activity may vary over time in relation to drug treatment and patient clinical condition. What constitutes a significant change in TPMT activity can be derived from biological variation and analytical imprecision.
Methods
A large national laboratory database was used to identify patients with three or more TPMT activity measurements. Variance of TPMT activity was analysed by determining the total coefficient of variation (CVTOT) of repeated measurements and by correlation with parameters including gender and follow-up time. Between-run analytical imprecision (CVa) was determined by replicate analysis (n = 314).
Results
Of 7383 patients with TPMT measurements, 136 were identified as having three or more measurements over time (range 3–14). Median CVTOT for individual patient results was 14.5% (range 2.5–36.7%). Analytical imprecision (CVa) was 10.3%. A reference change value (or critical difference) with 95% probability was calculated as 42%. Therefore, a change in measured TPMT activity above 42% should lead to considering sources of variation other than biological variation and analytical imprecision.
Conclusions
TPMT enzyme activity needs to change by at least 42% to determine that a true change has taken place beyond biological variation and analytical imprecision. A single measurement of TPMT activity is sufficient for most clinical purposes.
Keywords
Introduction
Azathioprine, 6-mercaptopurine and 6-thioguanine are thiopurines used in the treatment of a variety of clinical conditions, including haematological malignancies, organ transplantation, dermatological conditions and autoimmune disorders such as inflammatory bowel disease (IBD), rheumatoid arthritis and systemic lupus erythematosus. One of the most important enzymatic steps in the complex metabolic pathway of the thiopurines is S-methylation by thiopurine methyltransferase (TPMT).
The TPMT gene is subject to genetic polymorphism, leading to wide variation in enzyme activity. Red blood cell (RBC) TPMT enzyme activity has a tri-modal distribution among Caucasians. Approximately 90% of people have normal activity, 10% intermediate activity and 0.3%–0.6% low or absent activity. These phenotypes match with the homozygous *1/*1 wild-type, heterozygous *1/*3 and homozygous *3/*3 genotypes, respectively. 1 Patients with homozygous recessive and heterozygous variants of the TPMT gene with very low or undetectable RBC TPMT enzyme activity are predisposed to having high concentrations of the active metabolites 6-thioguanine nucleotides (6-TGN) and are thus at high risk of developing severe myelotoxicity on prescribed thiopurine drugs. 2 TPMT enzyme activity is therefore often measured routinely prior to thiopurine initiation to predict early drug-associated myelotoxicity. 3
Some studies have shown that the activity of TPMT may vary over time, with several factors leading to either induction or inhibition of TPMT. 4 In a study conducted by McLeod et al. 5 in children with acute lymphoblastic leukaemia (ALL) on stable therapy, the biological intra-individual coefficient of variation (CVi) was 13.5% over a one-year period on stable treatment. In healthy subjects, without disease, the mean long-term variability of TPMT enzyme activity was found to be only 6.5%. 6 The aim of our study was to determine the total variation of TPMT enzyme activity over time in patients with varying conditions and medical treatments. Second, by incorporating analytical imprecision of our TPMT assay, we aimed to calculate both intra-individual variation (CVi) and a critical difference and thus determine what represents a significant change in TPMT enzyme activity.
Materials and methods
Study design and patient selection
Canterbury Health Laboratories (CHL) in Christchurch, New Zealand, provides a national service for TPMT enzyme activity analysis. The CHL result database was searched for all TPMT enzyme activity measurements from March 2002 until October 2010. A total of 8523 TPMT enzyme activity results from 7383 individual patients were found. We selected patients with three or more TPMT enzyme activity measurements to determine the total variation (a composite of within-subject biological variation, analytical imprecision and pre-analytical factors). The rationale for repeated TPMT enzyme activity measurements in some patients is not known, but was thought most likely to be due to unintentional repeated requests associated with other routine blood test monitoring. One patient with three TPMT enzyme activity measurements was excluded because no gender was specified. The indication for thiopurine therapy was ascertained in a sample of patients where these data were available from case records. We derived the analytical imprecision of our assay by replicate (n = 174) TPMT enzyme activity measurements of samples taken every four months from a healthy subject on no medications over a two-year period. The between-run analytical imprecision (CVa) was 10.3%, calculated by averaging between-run imprecision data from a single individual whose blood was collected at intervals periodically over a four-year period. The mean TPMT enzyme activity was 11.4 IU/mL and the total number of measurements was 314. A random selection of request forms (n = 250) indicated that 45% of requests for TPMT were received from specialist gastroenterologists, 7% from rheumatologists, 15% from dermatologists, 3% oncologists, 20% general medicine or community general practitioners and 10% of unknown clinical speciality. We have no knowledge, however, of current drug therapies or when thiopurines might have been commenced or dosage altered.
RBC TPMT enzyme activity assay
In our laboratory, TPMT enzyme activity is measured by a radio-chemical method based on the conversion of 6-mercaptopurine (6-MP) to radio-labelled 6-MMP, using radio-labelled S-adenosyl-L-14C-methionine as the methyl donor. 7 Blood (2 × 5 mL) is collected in ethylenediaminetetraacetic acid (EDTA) tubes and transported to the laboratory under refrigerated conditions. Upon arrival samples are centrifuged to separate plasma from the blood. The RBCs are washed with saline. After lysis in ice-cold water, an aliquot of the lysate with 6-MP in dimethylsulfoxide (DMSO) and another aliquot with DSMO only are incubated with a potassium phosphate buffer of pH 7.5, S-adenosyl-L-14C-methionine, dithiothreitol and allopurinol for 60 min at 37℃. The reaction is stopped by the addition of a borate buffer of pH 10. Radioactivity is determined in a liquid scintillation counter with a mixture of absolute ethanol and toluene. TPMT enzyme activity with this measurement is considered to be low at <5.0 IU/mL, intermediate at 5.0–9.2 IU/mL and normal/high at 9.3–17.6 IU/mL. 8
Statistical analysis
Statistical analyses were conducted using GraphPad Prism version 4.01 (2004) for Windows (GraphPad Software Inc., San Diego, California, USA). To analyse variance of TPMT enzyme activity, total coefficient of variation (CVTOT) of repeated TPMT measurements was determined. Mann–Whitney tests were performed to compare subsequent TPMT measurements to the first one, which was expected to be measured before initiation of therapy. We also compared CVTOT between male and female patients. Spearman (non-parametric) rank correlation coefficients were derived. Between-run analytical imprecision (CVa) was determined by replicate analysis (n = 174) of a sample from a single subject over a period of two years. Statistical significance was assumed using P < 0.05.
From CVTOT, we calculated the reference change value (RCV) or ‘critical difference’ at 95% confidence level with the formula
9
:

Intra-individual variation (CVi) for TPMT was derived by the formula:

Results
The between-run analytical imprecision (CVa) using samples from a single individual (n = 174) was 10.3% (95% CI, 10.1–10.5).
A total of 7383 patients with TPMT measurements were identified from the laboratory database. One hundred thirty-six of those patients (1.84%) had three or more TPMT measurements done over time and were selected for analysis. For the 136 selected patients, the median (range) number of measurements done was 3 (3–14) over a median (range) follow-up period of 48 (0.7–332) weeks. Ten (7.4%) patients had eight or more measurements over a period of 129 (57–252) weeks.
For the total biological variation (CVTOT), the median value (range) was 14.5% (2.5–36.7). In general, there was no clear pattern in decrease or increase of TPMT enzyme activity over the period of follow-up within patients. Variance of TPMT enzyme activity was not different in male patients (n = 60) vs. female patients (n = 76) when CVTOT was compared (median 14.3 vs. 15.2 respectively; P = 0.37). In 35 patients (25.7%), TPMT enzyme activity crossed the threshold from either intermediate (5.0–9.2 IU/mL) to normal phenotype (9.3–17.6 IU/mL) or vice versa with subsequent measurements. Those patients had median CVTOT of 21% (11.5–36.7). The calculated total intra-individual variation (CVi) had a median value (range) of 10.2% (0.0–35.2%).
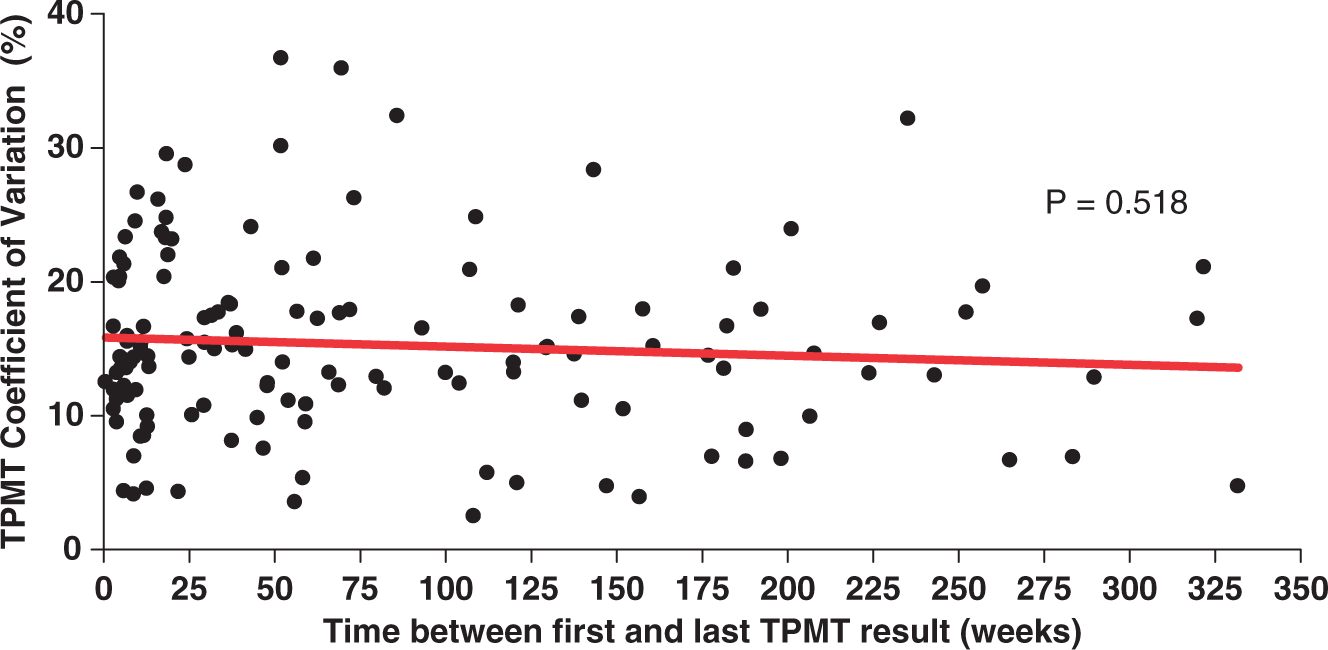
Overall, the median TPMT enzyme activity did not change over time with subsequent measurements compared with the first value (Figure 1). There was no significant correlation between patient CVTOT and time between first and last measurement (r = −0.056; P = 0.518; Figure 2), nor was patient CVTOT correlated with the number of measurements done (r = 0.13; P = 0.14). Repeated analysis with exclusion of patients with eight or more measurements showed similar results (r = –0.076; P = 0.40 for correlation of CVTOT with time between first and last measurement and r = 0.14; P = 0.11 for correlation of CVTOT with number of measurements). No correlation was found between number of measurements done and time between first and last measurement (r = −0.073; P = 0.40).
Median and interquartile range for red blood cell TPMT enzyme activity, using results from patients with three or more measurements, and showing results with each sequential measurement. Scattergraph showing TPMT activity coefficient of variation for every patient with 3 or more TPMT results, plotted against the time between first and last measurement. Linear regression line shown in red, with no significant correlation.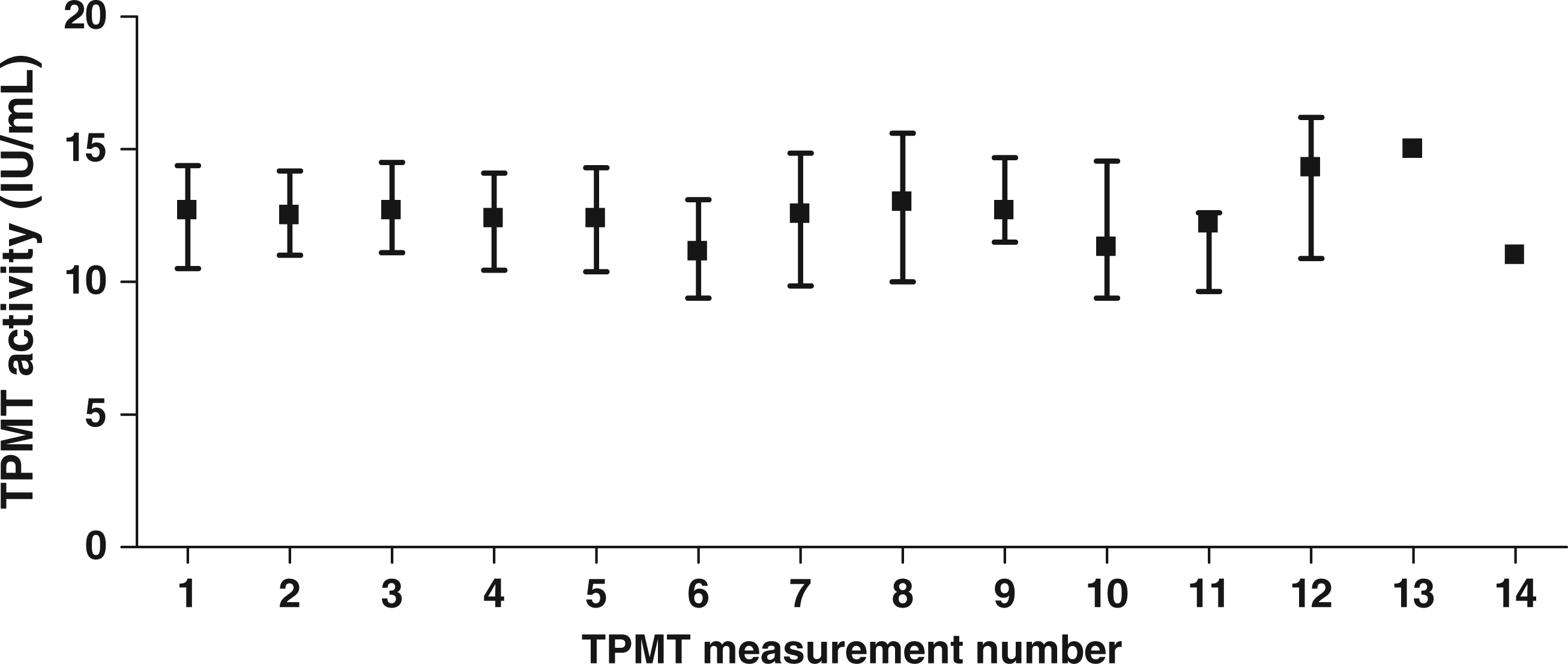
The calculated RCV, or critical difference with 95% probability, for a TPMT enzyme activity measurement to be significantly different from a previous measurement, was 42%. In our study population, 31 out of 136 patients (22.8%) had results that exceeded the RCV if subsequent measurements were compared to the first measurement, of which all but one showed an increase in activity. Of these patients, 20 (64.5%) crossed the threshold from intermediate to normal TPMT enzyme activity or vice versa. No patients crossed the threshold from intermediate to low.
Discussion
We investigated the total variation and intra-individual biological variation of activity of the TPMT enzyme, and assay variation. In our population, with a significant proportion of IBD patients, we found a low variance in TPMT enzyme activity. The total variation was calculated as 14.5%. The calculated CVi of 10.2% is somewhat lower than the CVi of 13.5% found by McLeod et al. 5 in paediatric patients with ALL over a one-year period on stable therapy. The reported CVi of 6.5% of TPMT enzyme activity in healthy subjects 6 is about two-thirds the variability observed in our study, suggesting that the variation in healthy populations cannot necessarily be applied to patient groups. Given that we studied a relevant reference group, our estimate of biological variation is therefore more likely to be clinically relevant.
Some studies during thiopurine treatment have shown differences from initial TPMT values that are either increased or decreased. 4 Several factors have been proposed to account for this TPMT variability on treatment. Thiopurine therapy itself induces the TPMT enzyme5,10 and similar results have been shown for diuretics. 5-aminosalicylic acid (5-ASA) compounds, which are often co-prescribed with thiopurines in IBD, have been reported to inhibit TPMT enzyme activity in vitro 11 and significantly increase 6-TGN concentrations in vivo with dose-dependent effects. 12 However, other studies have not shown decreased TPMT enzyme activity in association with 5-ASA treatment.4,10,13
We found low intra-individual biological variation of TPMT enzyme activity which did not vary significantly over longer follow-up or with number of measurements done. Approximately 23% of patient results exceeded the RCV on subsequent measurements, of which the majority (26 out of 31) showed an increase. It could be postulated that these patients are showing evidence of TPMT enzyme induction on therapy with thiopurines or other medication, although we do not have details of concomitant therapies to corroborate this further. The variation in TPMT enzyme activity in other patients did not exceed the RCV, and there was no clear pattern of increase or decrease in TPMT enzyme activity.
One factor that could result in an increased RCV is reduced TPMT activity in samples with a delay until TPMT analysis. In this study, 98% of samples were analysed within seven days and exclusion of samples with delayed analysis did not alter the RCV.
TPMT testing is generally required only once per individual, usually prior to the initiation of thiopurine therapy to guide dosing. Multiple tests are therefore usually unnecessary, and it is likely that most of those performed in our study were not done with the intent of examining the serial TPMT activity in the individual patient. However, repeat testing, prior to thiopurine therapy, may be useful to clarify the result of an initial TPMT test that was performed in the setting of transient factors that affect TPMT activity, such as acute renal failure with uraemia, a recent blood transfusion or recent change in medication. When repeat TPMT measurements are preformed, whether intentionally or inadvertently, knowledge of the RCV can help clinicians interpret results that might appear discrepant. In most situations, the repeat result will be within the RCV, which reassures the clinician that there is unlikely to be a true difference between results.
The measurement of TPMT activity is mostly used to detect those with a low or intermediate TPMT enzyme activity, of which the latter may require three-fold lower thiopurine dose. 14 These patients have an increased risk on severe myelotoxic events upon commencement of thiopurine therapy. However, low or intermediate TPMT enzyme activity accounts for only 10% of overall thiopurine toxicity. 15 Therapeutic drug monitoring by measurement of the metabolites 6-TGN and 6-methylmercaptopurine (6-MMP) is used to predict therapeutic efficacy, non-compliance, under-dosing, adverse effects, therapy resistance and toxicity in IBD. 6-TGN concentrations >235 pmol/8 × 108 RBCs are associated with therapeutic efficacy and 6-MMP concentrations >5700 pmol/8 × 108 RBC increase the risk of hepatotoxicity.16,17 Thus, although TPMT enzyme activity measurement is a useful clinical tool to identify homozygous deficient or heterozygous patients, repeated measurements of TPMT do not further influence clinical decision making.
The CVi derived from our study helps to set quality specifications for assay analytical precision as stipulated by Fraser. 9 It has been proposed that a minimal performance is defined by CVa < 75% CVi. Desirable CVa is considered to be <50% CVi and optimal <25% CVi, although quality specifications depend upon the analyte and its clinical purpose. The calculated CVa in this study was 10.3% with a CVi of 10.2%. Thus, our CVa was > 75% CVi and our TPMT assay therefore does not strictly meet what are considered to be minimal criteria for analytical performance, although precision is a property that is more important for monitoring purposes. Accuracy is more important, however, for TPMT and, in particular, for the detection of homozygous deficient cases.
The calculated RCV in our study is approximately 40%. A difference between TPMT results of 40% or greater therefore shows a true inhibition or induction of TPMT that cannot be solely attributed to the effects of analytical imprecision or biological variation. Although 36 of our patients crossed the cut-off between intermediate and normal TPMT enzyme activity, application of the RCV suggests that this is unlikely to be a real difference in the majority of our patients. Occasional misleading results for TPMT enzyme activity have been seen, however, in patients who have received a recent blood transfusion 18 and this is another factor that needs to be taken into consideration.
In conclusion, the total and intra-individual variation of TPMT enzyme activity in this patient population is low, conferring a critical difference or RCV of approximately 40% in a normal operational setting. For most clinical purposes, a single measurement of TPMT enzyme activity prior to initiation of thiopurine therapy is sufficient.
Footnotes
Acknowledgements
We acknowledge Ms Linda Pike and the staff of Specialist Biochemistry, Canterbury Health Laboratories for the TPMT assays and Associate Professor Chris Frampton for statistical advice.
Declaration of conflicting interests
None.
Funding
RvanE received unrestricted educational grants for this research from Abbott, Schering-Plough (MSD), and Tramedico.
Ethical approval
No specific ethical approval was required as the research resulted from laboratory audit analysis of non-identified patient sample results.
Guarantor
MB.
Contributorship
RvanE researched literature, assessed the patient results database, analysed the data and wrote the first draft of the manuscript. PC assisted with preparing the results database and data analysis. CS supervised the TPMT assay and prepared the results database. MB conceived the study, supervised RvanE, and assisted with data analysis and manuscript drafting. All authors reviewed and edited the manuscript and approved the final version of the manuscript.