
Abstract
Measurement of serum angiotensin-converting enzyme (ACE) activity can be helpful in the diagnosis and disease monitoring of sarcoidosis. Elevated serum ACE activity is found in 60–70% of sarcoidosis patients. Usually, the ACE activity is mildly increased (<3-fold the upper limit of the reference range) in sarcoidosis patients. Extremely elevated ACE activity is suggestive of the benign condition known as ‘familial hyperactivity of ACE’. Familial hyperactivity of ACE is a relatively rare condition and can be confirmed by genetic testing. Considering a genetic cause of strongly elevated serum ACE activity is important to prevent possible overdiagnostics. Here, we highlight the factors that may complicate the interpretation of serum ACE activity measurements, and we present two cases that illustrate the importance of interdisciplinary consultation when extremely elevated serum ACE activity is measured.
Introduction
Sarcoidosis
Sarcoidosis is an inflammatory disorder of unknown aetiology. Sarcoidosis can potentially affect any part of the body, but lung involvement occurs most commonly. The clinical presentation is variable; many patients have mild symptoms at presentation, while others have signs of severe systemic involvement. Nonspecific symptoms include fatigue, night sweats, fever and weight loss. Worldwide, estimates of disease prevalence range from 5 to 40 per 100,000. Most patients are diagnosed before the age of 50, with a peak incidence at the age between 20 and 40 years.1–4
Diagnosis of sarcoidosis, which requires consistent clinical findings and results of radiological imaging, can be challenging and tissue biopsy should be performed whenever possible, since the presence of non-caseous epithelioid granulomas in involved organs is the pathologic hallmark. An exception can be made for Löfgren's syndrome (constellation of erythema nodosum, arthralgia, fever and hilar lymphadenopathy). However, as the finding of such granulomas is not entirely specific for sarcoidosis, other possible diagnoses must be excluded.2,4,5 No gold standard currently exists to confirm the diagnosis. Measurement of the angiotensin-converting enzyme (ACE) activity in serum of patients with suspected sarcoidosis is one of the few laboratory tests that may be helpful to support the diagnosis.3,4,6,7
ACE: physiology and measurement
ACE plays an important role in blood pressure regulation and vascular remodelling as part of the renin-angiotensin-aldosterone system (RAAS). ACE enters the circulation by its highly regulated proteolytic cleavage from the cell surface of mainly pulmonary and renal endothelial cells.8,9
Sarcoid granulomas may produce ACE, which explains the elevated serum ACE activity in about 60–70% of patients with active sarcoidosis. 3 Studies have found that the serum ACE activity level correlates with the granuloma burden. 1 Specificity of increased ACE concentrations for sarcoidosis is only 85%, as increased concentrations of ACE have been found in a number of other conditions, such as liver disease, diabetes mellitus and hyperthyroidism. 10 The lack of sensitivity and specificity, taken together with the low prevalence of sarcoidosis in both the general population and in patients with non-specific symptoms, makes the serum ACE activity not suited as a screening test for sarcoidosis. 1 Therefore, the role of serum ACE is limited to a supportive, but not decisive, role in the diagnosis of sarcoidosis, and disease activity monitoring.
Different enzymatic assays, with very different reference intervals, are routinely used to measure ACE activity in serum. The reference interval of colorimetric assays is in the range of 8–21 U/L, and that of kinetic methods is 12–68 U/L.6,11 Because these methods measure the ACE activity rather than the ACE concentration, use of an ACE inhibitor will lead to a low measurement of serum ACE activity.
Genotypes influencing ACE concentrations
In both healthy controls and sarcoidosis patients, the serum ACE concentration is affected by genetic factors. The best studied example is the insertion (I) or deletion (D) of an Alu-repeat sequence of 287 base pairs in intron 16 of the ACE gene. Although usually not exceeding the upper limit of the reference interval, the homozygous D/D genotype is associated with 40–60% higher serum ACE activity than the I/I-genotype. The I/D-genotype shows intermediate serum ACE activity.6,9
More recently, polymorphisms in the ACE gene have been identified that cause extremely elevated ACE activity levels of at least 3-fold the upper limit of the reference interval, without apparent clinical symptoms.9,12,13 One of these mutations is the Pro1199Leu (rs121912703) missense mutation. This mutation causes a conformational change in the juxtamembrane stalk region of the ACE protein, making it more accessible to ACE secretase. This leads to increased ACE shedding and thus to increased serum ACE activity.7,9 Interestingly, hyperactivity of ACE is not associated with clinical abnormalities and thus appears to be a benign condition.7,9
Cases
We briefly present two cases of patients who were evaluated for sarcoidosis. In the diagnostic work-up, both patients and some of their family members were shown to be carriers of the Pro1199Leu mutation that causes hyperactivity of ACE. In our laboratory, serum ACE activity is measured by a colorimetric method (supplied by Fujirebio Inc.). The reference interval for this assay is 8–21 U/L. ACE genotyping was performed by PCR amplification and sequencing as described by Eyries et al. 8
Patient 1
A 41-year-old female patient was referred to a rheumatologist because of complaints of painful, warm, red toes and stiff fingers, particularly in the morning. The differential diagnosis included sarcoidosis, and as part of the diagnostic work-up, the serum ACE activity was determined. Whereas other laboratory results were unremarkable, the serum ACE activity was 125 U/L, which is about 6-fold greater than the upper limit of our reference interval. Other diagnostic tests did not support the diagnosis of sarcoidosis. The rheumatologist consulted with the laboratory about the possibility of the patient being a carrier of a mutation in the ACE gene that causes the hyperactivity of ACE. Indeed, DNA sequence analysis of part of the ACE gene revealed that this patient is a heterozygous carrier of the Pro1199Leu mutation, which is known to cause familial hyperactivity of ACE. The patient’s father and daughter had normal ACE activity levels of 8 U/L and 18 U/L, respectively, and are not carriers of the Pro1199Leu mutation. The patient’s mother had an elevated ACE activity level of 120 U/L and was also shown to be a heterozygous carrier of the Pro1199Leu mutation. See Figure 1(a) for a family tree. At presentation, the patient showed no signs of arthritis, and the arthralgias were successfully treated with low-dose NSAIDs. During the follow-up period, no signs of inflammatory pathology were observed, and the patient was discharged from the outpatient clinic.
Family trees of two families with hyperactivity of ACE. Arrows indicate the patients who are described in the main text (index cases). Squares indicate males and circles indicate females. Family members indicated by filled symbols are heterozygous carriers for the Pro1199Leu mutation. Family members indicated by symbols with question marks were not tested. The value below the symbols is the measured serum ACE activity (reference values: 8–21 U/L). Note the family member in (b) who is heterozygous for the Pro1199Leu mutation, yet has normal serum ACE activity.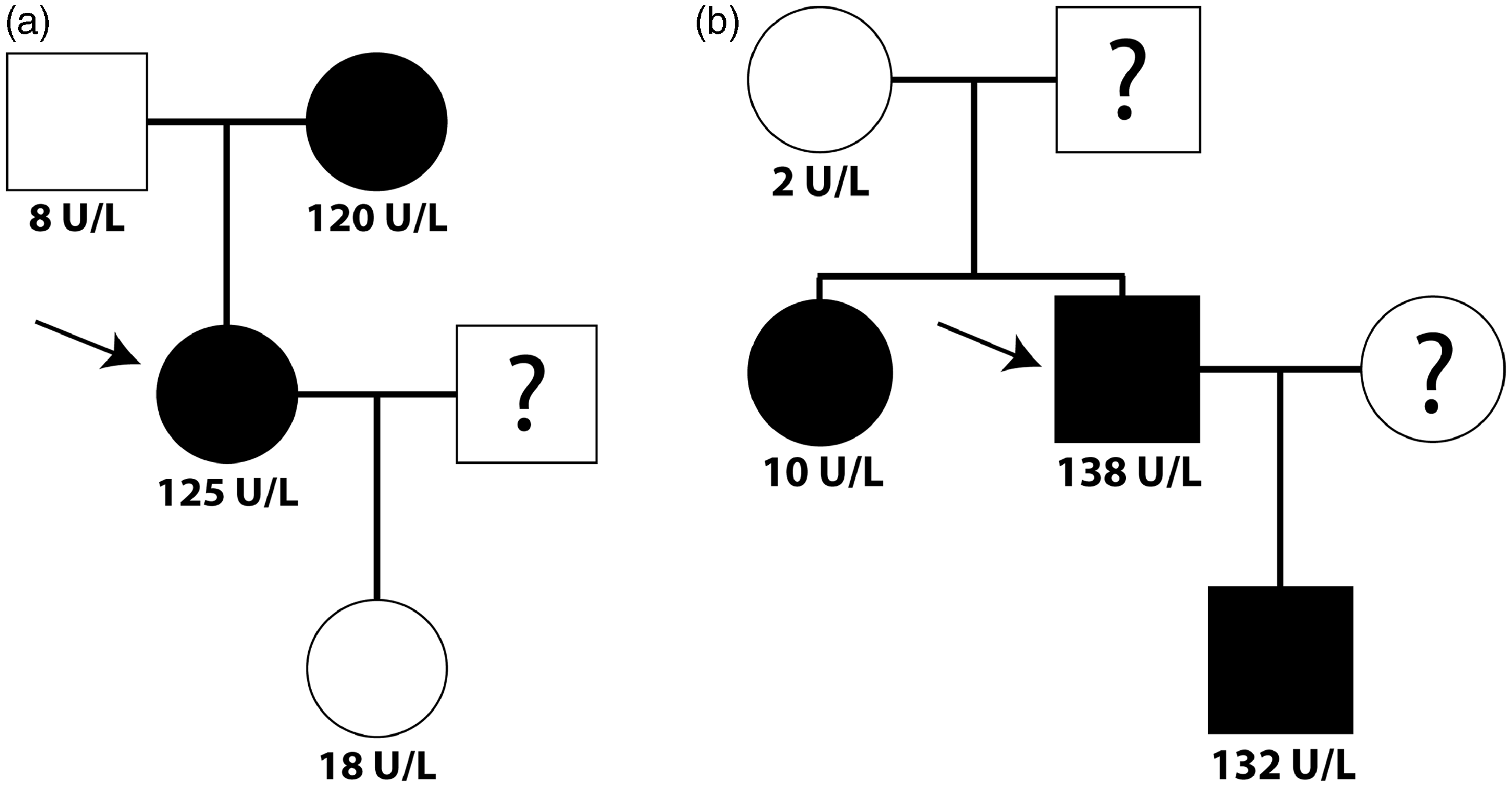
Patient 2
A 56-year-old male patient was referred to a neurologist with complaints of tingling feet and calves. No neurological cause for the tingling was found. However, the serum ACE activity was determined, and due to an extremely elevated ACE activity level of 138 U/L, the patient was referred to a pulmonologist for further evaluation. None of the subsequently performed diagnostic tests, including chest X-ray, bronchoscopy, pulmonary function tests and bronchoalveolar lavage analysis, indicated the presence of sarcoidosis. In consultation with the laboratory, both the patient and some of his family members were screened for DNA mutations that cause hyperactivity of ACE. The patient was found to be a heterozygous carrier of the Pro1199Leu mutation. The mother of the patient had an ACE activity level of 2 U/L and does not carry the Pro1199Leu mutation. The son of the patient had an ACE activity level of 132 U/L and is also a heterozygous carrier of the Pro1199Leu mutation. Surprisingly, the sister of the patient had a normal ACE activity level of 10 U/L, yet was found to be a heterozygous carrier of the Pro1199Leu mutation. Inquiry with her primary physician learned that she was taking the ACE inhibitor lisinopril (20 mg), which provides a likely explanation for these paradoxical findings. Figure 1(b) shows the family tree. The cause of the patient’s symptoms has yet to be determined.
Discussion
Serum ACE activity tests are mainly ordered as part of the diagnostic work-up of (suspected) sarcoidosis and to monitor the disease. Elevated serum ACE activity is found in 60–70% of sarcoidosis patients, as well as in a number of other conditions.3,6 ACE elevations due to sarcoidosis usually do not exceed the value of three times the upper limit of the reference range. This range cannot be expressed in absolute values, because different methods with profoundly different reference ranges are used to measure ACE activity in serum. If an ACE activity level of over 3-fold the upper limit of the reference interval is measured, the benign condition known as ‘familial ACE hyperactivity’ should be considered. 7 Several DNA-mutations in the ACE gene that cause hyperactivity of ACE have been reported.8,9,12,13 In the Netherlands, the Pro1199Leu missense mutation seems not uncommon. The prevalence is not known; however, on average we identify one patient with familial ACE hyperactivity per 600 ACE measurements. Kramers et al. 9 also reported similar data. The Pro1199Leu mutation has an autosomal dominant pattern of inheritance with complete penetrance. Thus far, only heterozygous carriers have been described in literature.8,9
Extreme elevations of ACE may go unnoticed if the ACE activity is reported by the laboratory in the form of ‘larger than’ a certain threshold, which is common practice in a number of laboratories. For example, when a kinetic method is used to measure the ACE activity, the exact value lies within the nonlinear range of the test. Therefore, it is important for clinicians to be aware of the lack of standardization concerning the measurement of ACE activity in serum, and it may be useful to request the laboratory to determine the exact value of the ACE activity by dilution. 9 This is specifically important when the serum ACE activity is used as a marker of disease activity. Obviously, if a patient is carrier of a mutation associated with hyperactivity of ACE, the elevated serum ACE activity should not be interpreted as being related to disease activity. Also, it should be clear that the finding of an extremely elevated ACE activity level does not rule out sarcoidosis. In recent years, we have seen one patient who was diagnosed with asymptomatic sarcoidosis and who was also a carrier of the Pro1199Leu mutation. This patient’s serum ACE activity was continuously extremely elevated, independent of the sarcoidosis.
The two cases we present here illustrate the importance of interdisciplinary consultation between clinicians and the laboratory. This way, unnecessary delay of the diagnostic process and expensive, unnecessary diagnostic follow-up tests may be prevented. When family members taking ACE inhibitors are screened for ACE hyperactivity, serum ACE activity can be normal even when a patient is carrier of an ACE hyperactivity mutation. To our knowledge, this is the first reported case of a carrier of the Pro1199Leu mutation displaying a non-elevated serum ACE activity level, which is most likely due to the use of an ACE inhibitor. This shows that ACE inhibitors should be temporarily discontinued prior to testing, or, alternatively, molecular diagnostics can be used to confirm that a patient is carrier of a mutation associated with hyperactivity of ACE. ACE genotyping is still not widely available, but molecular tests become increasingly affordable and incorporated into routine diagnostics.
Conclusion
Familial ACE hyperactivity is a benign condition that should always be considered when elevated serum ACE activity levels are measured that exceed 3-fold the upper limit of the reference range. To identify these extreme elevations with the current ACE activity assays, it is required to dilute the samples that have an ACE activity level that exceeds the linear range of the assay. Familial hyperactivity of ACE can be confirmed by molecular diagnostics. Family screening can be helpful to confirm the diagnosis of familial hyperactivity of ACE and may prevent future overdiagnostics. If screening is done by measuring the serum ACE activity only, it is important that ACE-inhibiting medication is discontinued prior to testing. Once familial hyperactivity of ACE has been established, ACE should not be used as a biomarker for the diagnosis of sarcoidosis and should not be interpreted to indicate increased disease activity. Interdisciplinary consultation between the laboratory and clinicians is important whenever a remarkably elevated serum ACE activity is measured.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Written informed consent to publication has been obtained.
Guarantor
FMJ.
Contributorship
KS designed and wrote paper, MW performed the laboratory measurements, MS and IT supplied patient history and clinic, EV and FV designed and edited paper and RC wrote and edited paper.