
Abstract
The aim was to assess the relative frequency of migraine and the headache characteristics of complex regional pain syndrome (CRPS) sufferers. CRPS and migraine are chronic, often disabling pain syndromes. Recent studies suggest that headache is associated with the development of CRPS. Consecutive adults fulfilling International Association for the Study of Pain criteria for CRPS at a pain clinic were included. Demographics, medical history, and pain characteristics were obtained. Headache diagnoses were made using International Classification of Headache Disorders, 2nd edn criteria. Migraine and pain characteristics were compared in those with migraine with those without.
Introduction
Complex regional pain syndrome (CRPS) and migraine are chronic and often disabling pain syndromes, which affect three times as many women as men (1–5). Both disorders are defined by clinical criteria. Migraine is characterized by moderate to severe, throbbing head pain that is often unilateral, aggravated by activity and associated with nausea, photo- and phonophobia and frequently allodynia (6). CRPS is characterized by pain, allodynia or hyperalgesia that is disproportionate to the inciting event and is associated with oedema, as well as vasomotor and sudomotor activity in the region of the pain (7). Although the full pathophysiology of both disorders is not known, both have been shown to be associated with neurogenic inflammation and systemic elevations of cytokines and neuropeptides, such as calcitonin gene-related peptide (CGRP) (8,9).
Several triggers of CRPS symptoms have been noted, including fractures or surgery, as well as inflammatory conditions such as varicella zoster, stroke and myocardial infarction (3,10). Two recent studies have suggested that the presence of headaches or migraines may be associated with CRPS. The first study was a clinic-based study that evaluated the occurrence of headache (of any kind) prior to development of CRPS symptoms in 23 CRPS patients compared with the relative frequency of headache in 69 controls. A total of 52% of the CRPS patients were found to suffer from headaches prior to the onset of CRPS symptoms, compared with 26% of the controls, P = 0.02 (11). The second study was a retrospective, general population study that evaluated 186 CRPS cases and 697 controls from the Integrated Primary Care Information database in the Netherlands. A primary care physician diagnosis of migraine was found to be associated with CRPS [odds ratio (OR) 2.43, confidence interval (CI) 1.18, 5.02]; however, a medical history of other headaches (OR 1.06; CI 0.56, 2.0) was not (12).
We have similarly noted that our CRPS patients appear to report a high frequency of migraine and that those with migraine more often report that the onset of their headaches occurred prior to the development of their CRPS symptoms. Thus, to explore further the potential of migraine as a risk factor for CRPS as well as to evaluate other potential associations between the two disorders, we evaluated the following parameters in a clinic-based population of CRPS sufferers: (i) the relative frequency of migraine and other headache disorders in those with CRPS, (ii) the reported age of onset of headaches and of symptoms of CRPS, and finally, (iii) the headache and pain characteristics in those CRPS sufferers with migraine compared with those without migraine.
Methods
We conducted a cross-sectional survey study of patients with CRPS presenting to an out-patient pain clinic between December 2007 and October 2008. The study was conducted after approval was obtained from the Institutional Review Board. All participants were examined by one of the authors (B.L.P. or R.J.S.). Participation was offered to consecutive patients using the following inclusion criteria: 18–75 years of age, physician diagnosis of CRPS I or II, and willingness to complete a self-administered written survey (13). Exclusion criteria included not being physically well enough to complete the survey or not being literate in English. CRPS diagnoses were made by one of the two pain specialists (B.L.P. or R.J.S.) utilizing the International Association for the Study of Pain (IASP) criteria; headache diagnoses were made by a headache specialist utilizing International Classification of Headache Disorders, 2nd edn (ICHD-II) criteria (B.L.P.).
Participants completed a standardized questionnaire constructed for this study. This questionnaire ascertained self-reported demographic information (including age, gender, race, marital status, education, and total household income), history of medical diagnoses, medication usage, self-reported height and weight, and migraine and pain characteristics.
CRPS questions
Diagnostic features and pain characteristics from CRPS were collected, including location and severity of pain, fingernail and hair growth changes, the presence of oedema, vasomotor symptoms, and mechano- and thermal-allodynia. Participants were asked to respond ‘yes’, ‘no’ or ‘I don't know’ to the presence of static allodynia (‘Do you experience pain when deep pressure or squeezing is applied?’), dynamic allodynia (‘Do you experience pain when you are touched or brushed lightly?’), deep joint pain (‘Do you experience deep joint pain or pain when pressure is applied to your joint?’) and thermal allodynia [‘Does an area of your body (such as your face or a hand or foot) feel colder or warmer than most other areas of your body?’]. Similar questions were asked with regard to skin colour and temperature changes, and swelling or fluid accumulation. Participants were also asked the age of onset of their symptoms attributable to CRPS, as well as the age of their diagnosis of CRPS by a physician. Finally, the following measurements were also evaluated in all participants.
Patient Healthcare Questionnaire
The Patient Healthcare Questionnaire (PHQ-9) is a self-reported diagnostic measure for current depression that utilizes the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria (14). As it has been shown that a score of ≥ 15 on the PHQ-9 is associated with a 68% sensitivity and 95% specificity in diagnosing ‘major depressive disorder’ using the DSM-IV criteria, major depression was defined as a score of ≥ 15.
Short Form-12
The Short Form (SF)-12 is a validated measure of health-related quality of life (15). It contains 12 items to evaluate eight concepts that relate to physical health (including physical functioning, role of physical abilities in accomplishments, body pain and general health) as well as mental health (including vitality, social functioning, role of mental health in accomplishments and overall mood). Physical and mental health composite scores range from 0 to 100, with a zero score indicating the lowest level of health and 100 indicating the highest level of health. Scoring of the SF-12 is standardized so that a representative sample of the US population will have a mean of 50 with a standard deviation of 10.
Body mass index
As body mass index (BMI) has been shown to be associated with chronic pain and migraine chronification, BMI was calculated for all participants (16–18). The following formula was used: BMI = wt(pounds)/ht(inches)2 × 703. Six categories were defined on the basis of the World Health Organization categories: underweight (< 18.5), normal weight (18.5–24.9), overweight (25–29.9), obesity grade I (30–34.9), obesity grade II (35–39.9) and obesity grade III (≥ 40) (19).
Headache questions
Headache questions covered all the diagnostic features of tension-type headache (TTH) and episodic migraine (EM) with and without aura, as specified by the ICHD-II (6). Each participant who responded affirmatively to having headaches in the past year was asked more detailed questions with regard to the duration, severity, location, aggravating factors, quality of pain, frequency, migraine-associated symptoms and visual and sensory aura, as previously described (20). The response options included never, rarely, less than half the time, and half the time or more. Responses of ‘never’ or ‘rarely’ were considered to be negative. In addition, those who reported headaches on < 15 days of the month were classified as episodic migraineurs and those with headache on ≥ 15 days of the month were defined as chronic daily headache (CDH) sufferers.
The following information was also gathered: the age of onset of the participants' first headache that was not caused by a head injury, hangover or an illness, as well as the age of onset of their most severe headaches and age of diagnosis of migraine by a physician, if given one. Finally, all participants who answered affirmatively to having headaches also completed the following questionnaires.
Headache Impact Test-6
The Headache Impact Test (HIT)-6 is a validated, brief questionnaire that demonstrates good reliability and validity across various levels of headache impact. The scale consists of six items that cover various areas reflected in health-related quality of life: pain, social functioning, role functioning, vitality, cognitive functioning, and psychological distress (21,22). Each of the six questions is responded to using one of five response categories: ‘never’, ‘rarely’, ‘sometimes’, ‘very often’ or ‘always’. For each item, 6, 8, 10, 11 or 13 points, respectively, are assigned to the response provided. These points are summed to produce a total score, ranging from 36 to 78. Higher scores indicate a greater impact of headaches on daily life.
Allodynia Symptom Checklist
Allodynia symptoms and scores were evaluated utilizing the Allodynia Symptom Checklist (ASC), as previously described (23,24). In brief, the ASC is a validated survey that includes 12 questions to evaluate the frequency of allodynia symptoms in association with headaches. Response categories were: never, rarely, less than half the time, half the time or more, and does not apply to me. Scores ranged from 0 to 24. Never and rarely responses were scored as 0, while less than half the time was scored as 1 and half the time or more was scored as 2. Categories based on the scores were defined as: no allodynia for scores ≤ 2, mild for scores between 3 and 5, moderate between 6 and 8 and severe for scores ≥ 9.
Statistical analysis
Results
Demographics
Demographic and clinical characteristics of complex regional pain syndrome participants

P ≤ 0.05 compared with the total group of those with no headache (No HA) or tension-type headache (TTH).
Numbers may not add to total due to missing data.
Headache diagnoses
Of the total participants, 89.4% (111/124) reported headaches within the past year. Whereas migraine or probable migraine has been estimated to occur in 29.6% of the general population, in our study a total of 78/124 (62.9%) fulfilled ICHD-II criteria for definitive or probable migraine (of which 92.3% were definitive migraine). In addition, it has been estimated that 4.7% of the general population suffer from CDH, whereas in our study a total of 16.1% (20/124) of participants had CDH, of whom 90.0% (18/20) fulfilled ICHD-II criteria for migraine (26). Finally, 10.5% (13/124) reported TTH and 10.5% (13/124) reported no headaches in the past year.
Age-adjusted standardized morbidity ratio of migraine and chronic daily headache in CRPS participants compared with the general population
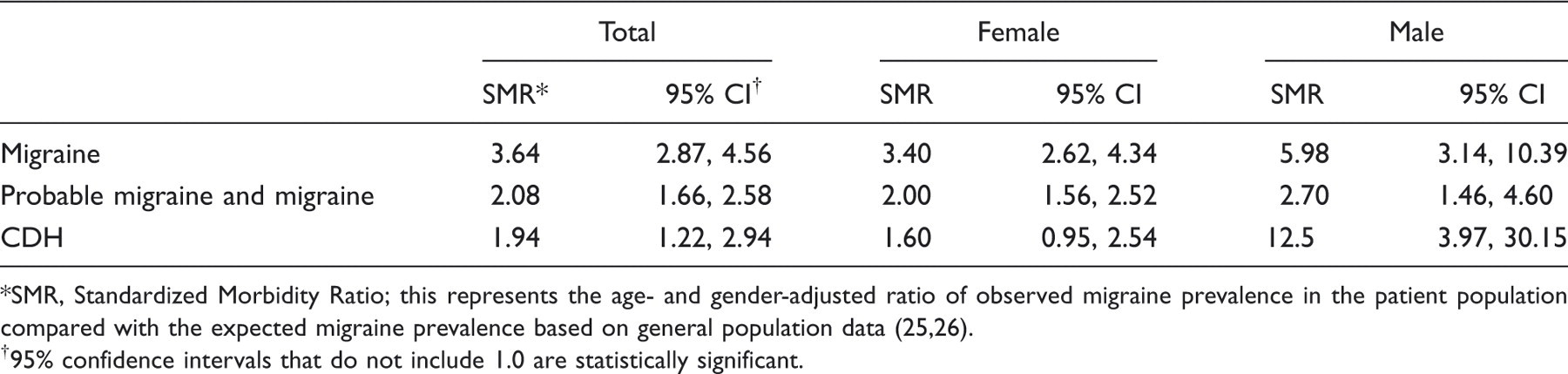
SMR, Standardized Morbidity Ratio; this represents the age- and gender-adjusted ratio of observed migraine prevalence in the patient population compared with the expected migraine prevalence based on general population data (25,26).
95% confidence intervals that do not include 1.0 are statistically significant.
Headache characteristics
Headache and general pain characteristics of complex regional pain syndrome participants

P ≤ 0.05 compared with the total group of those with no headache (No HA) or tension-type headache (TTH).
P ≤ 0.01 compared with the total group of those with No HA or TTH.
P ≤ 0.05 for comparison between definite migraineurs and those with chronic daily headache (CDH).
Numbers may not add to total due to missing data.
May also have face/torso pain.
% excludes those with no headache.
The majority of CRPS participants with any headache disorder reported the onset of severe headaches prior to the development of CRPS symptoms (Table 3). Of those CRPS sufferers with migraine, 82.1% (55/67) reported the onset of any headaches before the onset of CRPS symptoms, whereas 6.0% (4/67) of migraineurs reported the occurrence of symptoms attributable to their CRPS prior to the onset of headache; and 11.9% (8/67) reported that both the CRPS symptoms and headaches occurred within the same year.
Other pain syndromes
A total of 20 participants reported pain syndromes in addition to migraine and CRPS. A total of 18 participants reported only one other pain syndrome, while two participants reported both fibromyalgia and irritable bowel syndrome (IBS) and one person reported both IBS and osteoarthritis. A total of 10 participants noted a diagnosis of fibromyalgia, six reported IBS, four reported osteoarthritis, two reported thoracic outlet syndrome and one reported temporal mandibular joint dysfunction. There was no significant difference in the relative frequency of a physician diagnosis of other pain syndromes in those CRPS participants with headache (17.4%) compared with those without (8.3%), P = 0.69. Similarly, there was no significant difference in the relative frequency of a physician diagnosis of other pain syndromes in those CRPS participants with migraine (18.6%) compared with those without (10.8%), P = 0.45.
Depression (PHQ-9)
The mean PHQ-9 score was significantly greater in those CRPS suffers with CDH (15.2 ± 7.3) compared with those with no headaches or non-migraine headaches (9.0 ± 7.9), P < 0.05 (Table 1). However, there was no significant difference in the mean PHQ-9 between those CRPS sufferers with CDH and those with migraine.
CRPS characteristics
The mean duration of CRPS symptoms in those with migraine was 10.1 ± 7.4 years, compared with 5.8 ± 3.2 years for the combined group of those with no headache or TTH, but was not significant. However, the mean age of onset of CRPS was significantly earlier in those with migraine (34.9 ± 11.1 years) and CDH (32.5 ± 13.4 years) compared with those with no headaches (46.8 ± 14.9 years) and those with TTH (39.9 ± 9.9 years), P < 0.05. In addition, a significantly greater number of extremities were reported to be affected by CRPS in those participants with definitive migraine (median of four extremities involved) compared with the combined group of those CRPS sufferers with no headaches or TTH (median 2.0 extremities involved), P < 0.05. Furthermore, CRPS participants with CDH also had a median of four extremities involved; however, this association did not reach significance, probably due to small numbers.
There were no differences in reported vasomotor symptoms, oedema or fingernail growth between headache groups (Table 2). However, changes in hair growth were more frequently noted in those CRPS participants with migraine (82.5%) than in those with no headaches or TTH (53.8%) (P < 0.01, Table 2).
There were no differences between headache groups in those reporting thermal allodynia. Although no one type of mechano-allodynia was present in statistically higher proportions among CRPS participants with definitive migraine than in those with no headache or TTH, the presence of all three (static, dynamic and deep joint mechano-allodynia) was reported by more CRPS participants with definitive migraine (72.2%) than by the combined group of those with no headaches or TTH (46.2%); P ≤ 0.05.
Disability (SF-12)
The mean physical component survey (PCS) and mental component survey (MCS) scores of the SF-12 did not differ significantly between headache groups. The average PCS for the entire CRPS group was 1.3
Discussion
A recent case report on ‘migrainous corpalagia’ dramatically described three migraineurs who developed symptoms potentially consistent with CRPS (29). Even more recently, migraine has been implicated as potential risk factor for the development of CRPS (11,12). In the current study we further investigated the association between migraine and CRPS.
Specifically, we investigated the relative frequency of migraine and other headache disorders in a relatively large clinic-based population of CRPS sufferers. Our study confirms deMos et al.'s findings that migraine is associated with CRPS (12). It also supports their finding that non-migraine headaches are not associated with CRPS; and we more specifically define this group as those with TTH. Furthermore, we found an association between CDH and CRPS. This finding, while new, is not surprising, as it is likely that the majority of those classified as CDH in our study would be classifiable as transformed migraineurs by the Silberstein–Lipton criteria or as chronic migraineurs or medication overuse headache sufferers by ICHD-II criteria (6). Unfortunately, due to limitations of our survey we could not further classify our CDH participants.
Our findings also support the suggestion by Toda et al. that headache may be a risk factor for CRPS (11). Toda et al. found that 52.2% of CRPS participants reported headaches before an occurrence of CRPS. In our study, 82.1% of CRPS participants with migraine reported the onset of any headaches before the onset of CRPS symptoms; and 61.2% of those with migraine reported the onset of severe headaches before the onset of CRPS symptoms. Further supportive evidence that migraine may be a risk factor for CRPS in our study is that we found that the mean age of onset of CRPS symptoms was reported significantly earlier in those CRPS participants who reported definitive migraine (mean onset at 34.9 ± 11.1 years) or CDH (mean onset at 32.5 ± 13.4 years) than in those with no headaches (46.8 ± 14.9 years) or with TTH (mean onset at 39.9 ± 9.9 years).
We also evaluated the headache and general pain characteristics of those CRPS participants with headaches. Perhaps the most notable headache characteristics reported by our CRPS participants was the presence of aura. In the general population, approximately 2–4% of men and 4–9% of women have been estimated to have migraine with aura. This substantially increases among subjects with migraine, with 41% of migraineurs reporting aura in one study (28). In our current study, > 80% of CRPS participants with definitive migraine or CDH reported an aura. Even if we evaluated aura more conservatively (requiring it to be present in over half of their migraine attacks), > 60% reported an aura with their migraines.
The significance of aura in CRPS sufferers is not known. However, aura has been described as the clinical manifestation of cortical spreading depression (CSD) in migraineurs. Specifically, functional imaging studies of migraineurs have shown regions of focal hyperperfusion followed by hypoperfusion that spreads gradually in all directions (30–32). This spreading oligaemia has been primarily shown to start in the posterior region of the brain, but has been reported to start in the frontal region also (30,31). CSD has not been described in complex regional pain syndrome sufferers. However, functional imaging of CRPS sufferers has shown higher regional cerebral blood flow (rCBF) in the frontal and parietal lobes and decreased thalamic rCBF (33–35). Future studies evaluating multiple positron emission tomography or single photon emission computed tomography scans separated over time in individual CRPS sufferers with and without migraine with aura may be of interest to determine if CSD may occur in CRPS sufferers. Finally, as migraine with aura has been shown to be associated with an increased risk of vascular disease including ischaemic stroke, myocardial infarction and angina, our finding implies that the cardiovascular risk profile may be similarly increased in CRPS sufferers (36). Future studies to evaluate the cardiovascular risk profiles in CRPS sufferers are likewise warranted.
Of the general pain characteristics evaluated, three significant finding are of note. The first is with regard to the presence of allodynia. Over 70% of migraineurs seeking tertiary care have been shown to exhibit allodynia in both cephalic and extracephalic locations (37,38). In our study, those CRPS participants with definitive migraine were significantly more likely to report the presence of all three forms of mechano-allodynia (including dynamic, static and deep joint) than those with no headache or TTH. Second, we also found that the median number of painful extremities from CRPS was significantly greater in those with migraine (four extremities) compared with those with no headache (2.5 extremities) or TTH (two extremities).
Finally, although the mean headache-related disability and depression scores (PHQ-9) were greater in those CRPS sufferers with definitive migraine and CDH than in those with no headaches, TTH or probable migraine, the mean SF-12 scores were not significantly different between headache groups. This suggests that although those CRPS sufferers with migraine may have a more severe form of the disease (earlier onset, greater extent of limb involvement, more mechano-allodynia), neither migraine nor CDH substantially adds to the general physical or mental disability from CRPS.
How migraine is associated with CRPS is not known. It is possible that central sensitization plays a role, as previously suggested by Toda et al. (11). In addition, there are several pathophysiological similarities between the two disorders. Neurogenic inflammation plays a significant role in both migraine and CRPS (8,9), and several biochemical factors (including nitric oxide, CGRP and substance P) as well as cytokines [such as interleukin (IL)-1 and IL-6] have been shown to be significantly associated with the inflammation seen in both disorders (39,40).
Our study has several strengths. First, it included a relatively large number of CRPS patients. Second, the diagnosis of CRPS was made by pain specialists utilizing the IASP criteria; and the diagnoses of migraine, probable migraine and TTH were made utilizing the ICHD-II criteria. However, caution is required when interpreting our data. First, we did not evaluate non-pain controls. Furthermore, all participants came from a tertiary clinic and may represent those with more severe forms of CRPS. Finally, this study is subject to both sampling and measurement biases common to questionnaire studies, particularly recall and volunteer bias. Longitudinal studies following a large population of migraineurs, to identify what percentage of migraineurs develops CRPS compared with the general population, is needed to clarify these possibilities.
Conclusions
Our current study supports that migraine may be a risk factor for CRPS and that the presence of migraine may be associated with a more severe form of CRPS. As such, our findings imply that aggressive management of those who suffer from migraine may be warranted. Longitudinal studies evaluating the relative frequency of CRPS in migraineurs are needed. Finally, as we also found that the presence of aura is reported in a higher percentage of CRPS sufferers than in the general population, and as migraine with aura is a cardiovascular risk factor, further evaluation of the cardiovascular risk profile of CRPS sufferers is also warranted.
Footnotes
Appendix A International Association for the Study of Pain (IASP) Diagnostic Criteria for Complex Regional Pain Syndrome
The presence of an initiating noxious event, or cause of immobilization Continuing pain, allodynia, or hyperalgesia with pain which is disproportionate to any inciting event Evidence at some time of oedema, changes in skin blood flow, or abnormal sudomotor activity in the region of pain No evidence of conditions that would otherwise account for the degree of pain or dysfunction.