
Abstract
The International Headache Society (IHS) diagnostic criteria for headache improved the accuracy of primary headache diagnoses, including migraine. However, many migraineurs receive an ‘atypical migraine’ diagnosis according to the IHS nosology (IHS 1.7), indicating that they approximate but do not fully meet all IHS criteria. This study characterized and sub-classified patients with atypical migraine. Within a clinical sample of 382 headache sufferers, 83 patients met IHS criteria for ‘atypical migraine’. Patients receiving the IHS 1.7 designation did not converge to form a homogeneous group. Rather, distinct and clinically relevant subgroups were empirically derived (e.g. migraine with atypical pain parameters, brief migraine, chronic migraine). The results call for revisions of the IHS diagnostic criteria for migraine that would minimize the number of patients receiving an atypical diagnosis. Revisions would include decreasing the minimum headache duration criteria from 4 h to 2 h, and developing a classification for ‘chronic migraine’ for migraine greater than 15 days per month. The proposed revision provides a means of diagnosing the daily and near-daily headache commonly observed in clinical populations.
Introduction
In 1988, the International Headache Society (IHS) proposed a revised headache classification system (1) that provided operational criteria for the diagnosis of headache disorders. Use of the IHS classification and diagnostic criteria for headache undoubtedly improved the accuracy of primary headache diagnoses including migraine (2–7). The majority of patients who present to headache clinics receive a migraine diagnosis; most are diagnosed as having migraine without aura (IHS 1.1) or migraine with aura (IHS 1.2 8). However, when IHS criteria are applied, a sizable proportion of headache patients with migrainous features fail to fully meet IHS migraine criteria (between 10% and 45%), and thus they receive an ‘atypical migraine’ diagnosis (IHS 1.7: migrainous disorder not fulfilling all criteria) (3, 7, 9).
According to the IHS nosology, a patient is diagnosed with atypical migraine if his/her headaches fulfil all of the diagnostic criteria for migraine except one (i.e. patients fail to meet criterion B, C or D). Thus, a 1.7 code is assigned when one of three symptom patterns exists: (a) migraine duration is either less than 4 h or longer than 72 h (criterion B: ‘duration’), but all other migraine criteria are met; (b) the required endorsement of at least two pain characteristics is not met (criterion C: ‘pain characteristics’), but all other migraine criteria are met; or (c) no associated non-pain features are present (e.g. nausea, photophobia) (criterion D: ‘associated symptoms’), but all other migraine criteria are met.
Since the introduction of the IHS classification, many clinic-based studies and population surveys evaluated the generalizability of the classification across primary headache diagnoses. A subset of these studies focused on patients with daily or near-daily headaches with migrainous features, labelled ‘transformed migraine’ by some, but none looked at the full clinical spectrum of the cohort of patients who fulfil the IHS 1.7 criteria. Thus, the present study was designed to characterize IHS 1.7 (atypical migraine) patients and to determine whether distinct patient subgroups could be discerned. A second goal of the present study was to derive empirically based revisions to the IHS criteria which would allow classification of a greater number of patients who are presently classified with the atypical migraine diagnosis (IHS 1.7).
Methods
The initial patient sample consisted of 382 adult headache sufferers presenting to an outpatient headache clinic for treatment. The Structured Diagnostic Interview for Headache or SDIH (10–14) was administered to obtain information on headache history and medication use. The information obtained during the interview was entered into the SDIH computer database and the SDIH software was used to generate an initial IHS diagnosis. An expert headache diagnostician confirmed the computer-generated diagnosis and disagreements were resolved through consultation with an additional headache expert. Multiple headache diagnoses were formulated for patients who presented with more than one type of headache (e.g. one patient could be diagnosed ‘migraine without aura’ as well as ‘episodic tension-type headache’, reflecting two distinct headache patterns). No attempt was made to diagnose every conceivable headache pattern; rather, these findings reflect the patients' primary presenting headache syndromes. In case of multiple headache diagnoses in the same patient, headaches were prioritized in order of importance with respect to treatment and the primary headache diagnosis was used in the subsequent analysis.
Results
A complete breakdown of headache diagnoses for the 382 patient sample is provided in Table 1. Of the 382 patients, 227 met IHS criteria for a migraine diagnosis (IHS 1.1–1.7 codes), including: 115 migraine without aura (IHS 1.1), 24 migraine with aura (IHS 1.2), five retinal migraine (IHS 1.4) and 83 atypical migraine (IHS 1.7: migrainous disorder not fulfilling all criteria). Thus the atypical migraine group accounted for 22% of the total sample and 36% of the migraine diagnoses. All patients classified as atypical migraine failed to meet IHS criteria for tension-type headache (IHS 2.1 to IHS 2.2).
IHS headache diagnoses for total sample of 382 patients

The total sample was predominantly female (77%) with a mean age of 37.7 years (
Subgroups of patients diagnosed with the IHS 1.7 code or atypical migraine
All patients receiving an IHS 1.7 diagnosis could be uniquely categorized into one of five distinct patient subgroups: (a) unremitting migraine (Unremitting); (b) migraine exceeding the 72 h duration criteria specified by IHS (Greater than 72 h) ∗ ; (c) migraine episodes that fell below the minimum duration criteria of 4 h (Brief headache); (d) migraine with atypical headache pain parameters with respect to location, quality, intensity and aggravation by activity (Pain characteristics); and (e) migraine without the usual associated non-pain symptoms, including nausea, vomiting, photophobia and phonophobia (Associated symptoms). Subgroups a, b and c above were atypical because they failed to meet the headache duration criterion for migraine (criterion B; headache episodes last 4–72 h), whereas the remaining two subgroups of patients were atypical either because of pain characteristics (criterion C; headache pain characteristics) or associated symptoms (criterion D; associated non-pain symptoms). Patients who fail to meet IHS criterion A (‘At least 5 attacks fulfilling B-D’) form another possible subgroup of atypical migraine patients. As this sample was comprised of patients who presented for treatment at a special headache centre, no such patients were included here.
Failure to meet the headache duration criterion was the most common reason for receiving the IHS 1.7 diagnosis (n = 58; 70% of all IHS 1.7 patients). The largest single subgroup among the IHS 1.7 patients consisted of 40 individuals who were deemed atypical because the duration of their headache episodes exceeded the 72-h upper limit; thus almost half (48%) of all IHS 1.7 patients fell within this subgroup. Of these patients, 31 described their headaches as ‘unremitting’, and nine reported headache episodes that were ‘greater than 72 hours’ but their headaches were not unremitting. An additional 18 patients (22% of all IHS 1.7 patients) exhibited ‘brief headache’, with headache episodes that typically remitted in less than the 4-h lower limit specified in the IHS nosology.
Sixteen patients with atypical migraine (19% of all IHS 1.7 patients) differed from other migraine patients on the basis of ‘pain characteristics’ because they did not report a minimum of at least two of the following: pulsating pain, unilateral location, moderate to severe pain intensity, and aggravation by activity. Of the patients in this subgroup, 11 (69%) met only the ‘severity’ criterion, one (6%) reported only a unilateral location, one (6%) reported only that her headache was aggravated by physical activity, and three (19%) reported none of the usual pain characteristics of migraine. The remaining nine patients with atypical migraine (11% of all IHS 1.7 patients) differed from other migraine patients on the basis of non-pain ‘associated symptoms’ (i.e. nausea, vomiting, photophobia and phonophobia). These patients did not report any of the associated symptoms listed in criterion D of the IHS nosology for migraine.
Comparison of atypical subgroups with migraine group (IHS 1.1–1.4)
Demographic characteristics
Patients from the total sample who met IHS criteria for either migraine without aura (IHS 1.1), migraine with aura (IHS 1.2) and retinal migraine (IHS 1.4) were combined into a single ‘Migraine’ group (n = 144). Analyses revealed that patients with an IHS 1.1 diagnosis did not differ from patients with an IHS 1.2 diagnosis with respect to gender, age, headache indices (severity, duration and frequency) or medication use (prescription and non-prescription; all Ps > 0.05); patients with an IHS 1.4 diagnosis were not included in the latter analyses because only five patients received the 1.4 diagnosis. Means and ranges for demographic (gender, age) and headache (frequency, duration and severity) variables for the various IHS 1.7 subgroups and the combined Migraine group are reported in Table 2.
Demographic and headache variables (mean, standard deviation and range)
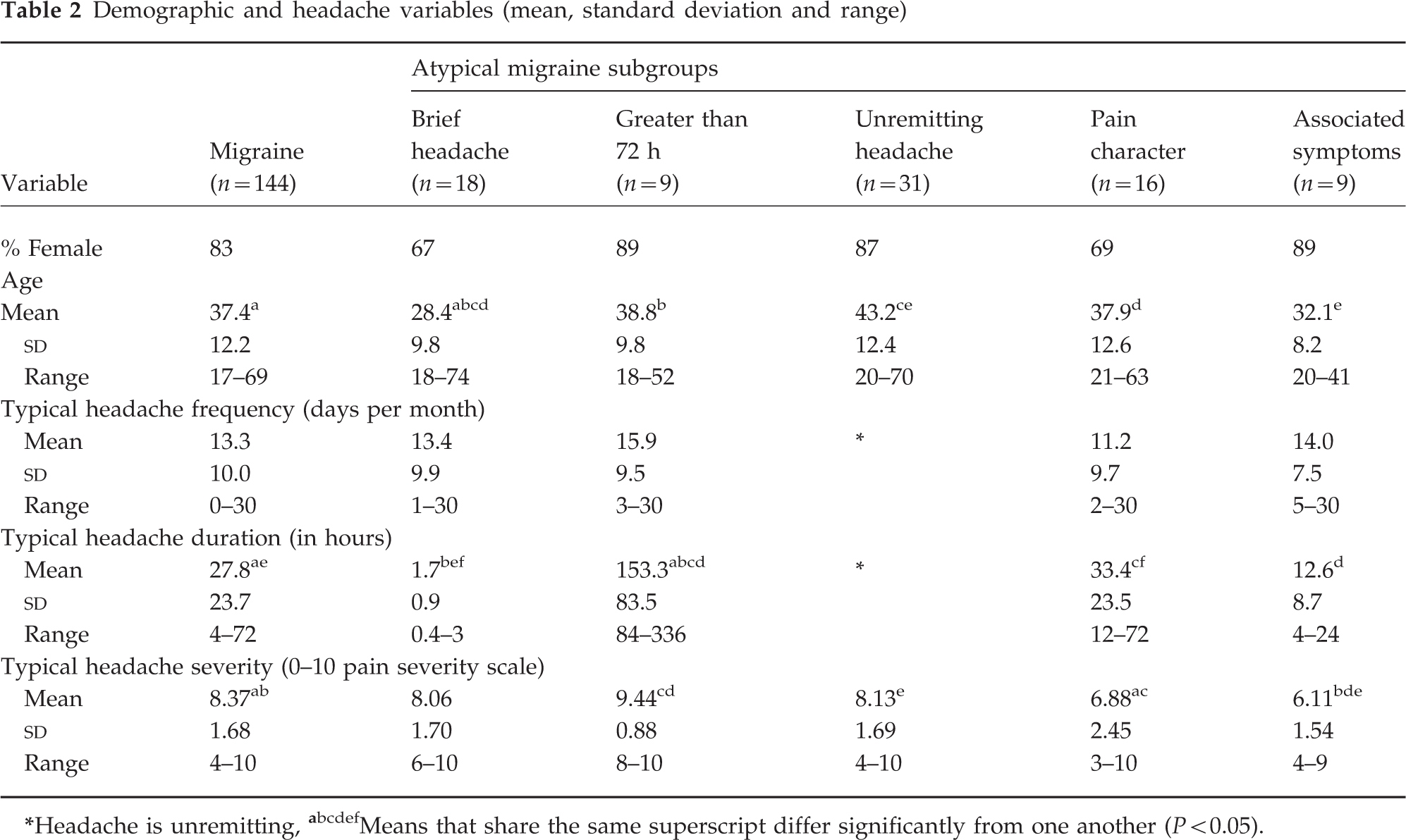
Headache is unremitting,
Means that share the same superscript differ significantly from one another (P < 0.05).
Comparison of the Migraine group with the five IHS 1.7 subgroups indicated that the groups did not differ with respect to gender composition (x2 ( d.f. = 5) = 5.77; ns). All diagnostic groups were predominantly women.
One-way analyses of variance (
Headache parameters
The headache frequency data (i.e. number of headache days per month) for each of the atypical subgroups and the Migraine group are reported in Table 2. By definition, patients in the Unremitting subgroup reported the highest possible monthly headache frequency (i.e. headache every day), while patients in the Pain Characteristics subgroup reported the fewest headache days per month (M = 11.25). The nature of the data precludes inclusion of the Unremitting subgroup in statistical analyses of headache frequency because the Unremitting group by definition has no variance in headache frequency. One-way
Headache duration was widely varied across the groups (see Table 2). Again, the Unremitting subgroup was excluded from this analysis because their headache duration was, by definition, unlimited and thus no duration figures were available. Although the Brief Headache and Greater than 72 h groups were formed in part based on headache duration, they were included in the subsequent analysis. Results were interpreted cautiously. One-way
Headache pain severity of the typical migraine episode (11-point scale ranging from 0 = no headache to 10=extremely painful headache) was compared among groups (Table 2). One-way
Medication overuse
The patients' history of medication use was investigated to determine if headaches were related to chronic substance use (IHS 8.2: Headache induced by chronic substance use or exposure). The conservative criteria recommended by the IHS to define substance overuse were employed: (a) typical daily dose of aspirin/acetaminophen for the past 3 months of 4 or more tablets; or (b) typical daily dose of prescription analgesics or sedatives for the past 3 months of 2 or more tablets.
The percentage of patients meeting IHS 8.2 criteria for medication overuse in the Migraine and atypical subgroups are reported in Fig. 1. Reported separately are percentages of patients in each group overusing non-prescription medications, prescription medications and combined medication overuse (use of either non-prescription, or prescription, or both). Chi-square comparisons of the Migraine group and atypical subgroups revealed significant differences in the proportion of patients overusing medications among the groups for non-prescription medications (x2 (d.f. = 5) = 14.05; P < 0.01), prescription medications (x2 (d.f. = 5) = 16.00; P < 0.01), and combined prescription and non-prescription medications (x2 (d.f. = 5) = 18.04; P < 0.01).

Percentage of patients in Migraine and Atypical Migraine subgroups meeting IHS 8.2 criteria for analgesic and sedative medication overuse (including non-prescription, prescription, and combined non-prescription/prescription medication overuse). □ Non-prescription prescription;  Combined.
Combined.
The highly variable sample sizes across groups and the small sample sizes for some groups precluded meaningful pair-wise comparisons between most of the subgroups. However, the Unremitting subgroup had a sufficient number of patients to permit appropriate statistical comparison with the Migraine group with respect to medication overuse using the x2 statistic.
The Unremitting subgroup (n = 31) is substantially smaller than the Migraine group (n = 144) and thus results must be interpreted cautiously. All statistical comparisons were significant, including the use of non-prescription medications (x2 (d.f. = 1) = 6.62; P = 0.01), prescription analgesics and sedatives (x2 (d.f. = 1) = 4.76; P < 0.05), and combined prescription and non-prescription medications (x2 (d.f. = 1) = 8.21; P < 0.01). In all cases, the Unremitting subgroup exhibited a higher percentage of medication overuse than did the Migraine group.
As indicated in Fig. 1, the Unremitting group exhibited the highest percentages of analgesic overuse, with a full 74% of patients in this group overusing prescription and/or non-prescription medications. A large percentage of patients in the Greater than 72 h (56%), Associated Symptoms (56%) and Migraine (46%) groups also overused medications.
Revision of IHS diagnostic criteria for migraine
Based on the initial findings of this study (as described above) and earlier literature, a proposed revision to the IHS diagnostic criteria for migraine was developed. The revisions are summarized in Table 3 and the rationale supporting the revisions is addressed in the Discussion section below. The revised criteria propose two principal changes from the original IHS classification (1): a decrease in the minimum duration criteria for migraine from 4 h to 2 h; and (2) a differentiation of episodic migraine (less than 15 headache days per month) and chronic migraine (equal or greater than 15 headache days per month). This revision would leave the remaining diagnostic criteria for migraine (IHS 1.3–1.7) unchanged from the original IHS specification.
Proposed revisions to the IHS headache classification and diagnostic criteria for migraine∗

IHS codes 1.3–1.7 remain unchanged.
Revised diagnostic classification of episodic migraine, chronic migraine and atypical subgroups
Configuration of revised groups and demographic characteristics
Using the revised diagnostic criteria, all patients with migrainous headaches were classified into one of three groups: episodic migraine (n = 92), chronic migraine (n = 98) or atypical migraine (n = 37). With the revised criteria, 16% of migrainous patients would continue to receive the Atypical (1.7) designation (as opposed to 36% using the standard IHS criteria). The Atypical subgroups now include: brief headache (n = 9), greater than 72 h (n = 3), pain characteristics (n = 16) and associated symptoms (n = 9). The Unremitting Headache group from the earlier analysis is now subsumed under Chronic Migraine, and the Chronic Migraine group also now includes some patients originally classified in the Greater than 72 h or the Migraine groups. The revised criteria left the Pain Characteristics and Associated Symptoms subgroups unchanged, and 50% of the patients formerly classified as Brief Headache were reclassified as Migraine according to the revised criteria.
Demographic (gender, age) and headache (frequency, duration, severity) variables for the groups are reported in Table 4. All diagnostic groups were predominantly women and did not differ on gender composition (x2 (d.f. = 5) = 3.30; ns). Groups also did not differ on age (F (5, 221) = 1.51, ns).
Revised groups—demographic and headache variables
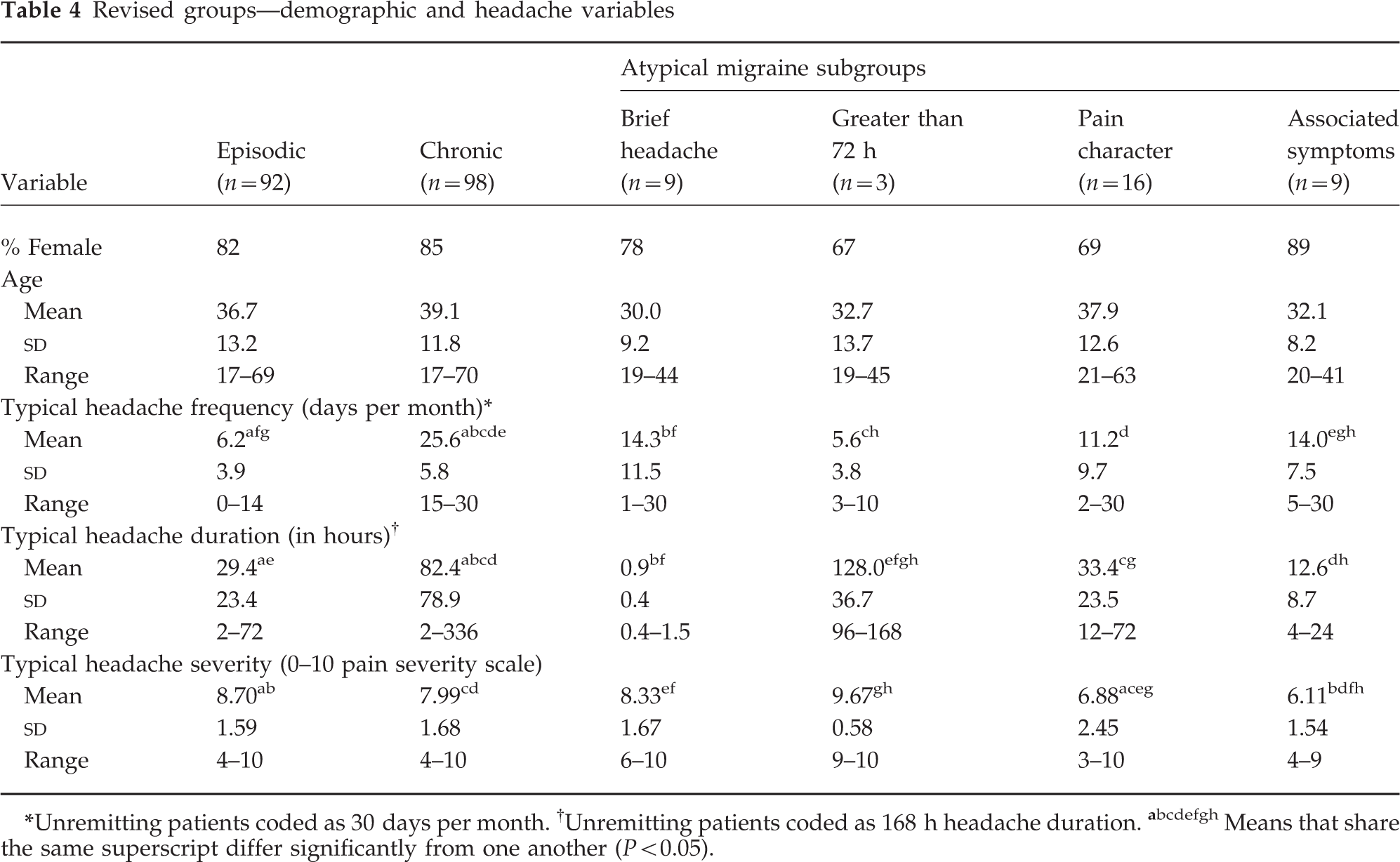
Unremitting patients coded as 30 days per month.
Unremitting patients coded as 168 h headache duration.
Means that share the same superscript differ significantly from one another (P < 0.05).
Headache parameters in revised groups
The Episodic Migraine, Chronic Migraine and Atypical subgroups were compared on headache parameters (headache frequency, duration and severity; see Table 4). Because the groups were formed in part based on headache frequency, the variance for the Episodic and Chronic Migraine groups is artificially constrained on that variable. One-way
Likewise, one-way
Analgesic overuse among revised groups
The percentages of patients within each of the revised groups meeting IHS criteria for analgesic overuse (IHS 8.2) are reported in Fig. 2, with data representing non-prescription medication, prescription medication and combined medication overuse presented separately. Chi-square comparisons of the Episodic Migraine, the Chronic Migraine and the four Atypical subgroups revealed significant differences in the proportion of patients overusing prescription medications (x2 (d.f. = 5) = 30.55; P < 0.001) and combined prescription and non-prescription medications (x2 (d.f. = 5) = 23.99; P < 0.001). There were no differences in the proportion of patients overusing non-prescription medications (x2 (d.f. = 5) = 8.41; P = ns).
Percentage of patients meeting IHS 8.2 criteria for analgesic and sedative medication overuse (including non-prescription, prescription, and combined non-prescription/prescription medication overuse) among patients meeting diagnostic criteria for Episodic Migraine, Chronic Migraine, and the Atypical Migraine subgroups with proposed migraine classification revisions. □ Non-prescription; prescription; Combined.
Because of the highly variable sample sizes among groups and subgroups, meaningful pair-wise comparison statistics could only be conducted on the Episodic Migraine and the Chronic Migraine groups. Pair-wise chi-square comparisons revealed significant differences in the use of prescription analgesics and sedatives (x2 (d.f. = 1) = 23.17; P < 0.001) and combined prescription and non-prescription medications (x2 (d.f. = 1) = 16.52; P < 0.001); in both cases the Chronic Migraine group exhibited greater proportions of patients with medication overuse than did the Episodic Migraine group. In the Chronic Migraine group, 42% overused prescription medications and 64% overused some combination of prescription and/or non-prescription medications, compared with 11% and 35%, respectively, for the Episodic Migraine group. The Chronic Migraine (39%) and Episodic Migraine (28%) groups did not differ on the percentage of patients overusing non-prescription medications (x2 (d.f. = 1) = 2.34; P = ns).
The small sample sizes amongst the revised Atypical subgroups (Greater than 72 h, Brief Headache, Associated Symptoms, Pain Characteristics) precluded statistical analysis. Nevertheless, as can be seen in Fig. 2, one of the three patients (33%) remaining in the reclassified Greater than 72 h subgroup overused prescription medications, and no patient overused non-prescription medications. Within the Brief Headache subgroup only one of the nine (11%) patients overused medication; that individual overused both prescription and non-prescription medications. The group composition of the remaining subgroups (Pain Characteristics, Associated Symptoms) was unchanged from the earlier classification and their medication overuse patterns are described above in the earlier section on analgesic overuse.
Discussion
This study revealed that 36% of the patients with migrainous headache in the large clinical sample of adult headache patients received an IHS diagnosis of migrainous disorder not fulfilling above criteria (IHS 1.7) or ‘atypical migraine.’ Thus, over one-third of the adult migrainous patients who presented for treatment to the specialty clinic setting failed to fully meet IHS criteria for migraine or any other IHS diagnosis (with the exception of the IHS 8 codes reflecting substance use or withdrawal). This finding was similar to that reported in an earlier study of the IHS headache nosology that examined questionnaire data from 410 adult headache sufferers with headache of at least 2 years duration; 120 of 271 total migraine diagnoses (44%) were classified as IHS 1.7 or atypical migraine (29% of the total 410 headache sample would have been 1.7) (9). In contrast, another recent investigation examined structured diagnostic interview data from 103 headache patients who presented to specialty clinics; approximately 10% of all patients and approximately 12% of all migraine patients received an IHS 1.7 diagnosis (3).
Studies of child and adolescent headache sufferers also have classified large numbers of patients as IHS 1.7, including 24.3% of 395 migraine headache patients in one study (15) and 20.5% of 409 headache patients in a second study (16). Although there have been few additional investigations of the IHS 1.7 classification in clinical samples of headache patients, population-based analyses of the IHS criteria have classified between 11% and 16% of migraine sufferers as 1.7 (7, 17). Thus, between 12% and 44% of migraine headache patients receive an IHS 1.7 or ‘atypical migraine’ diagnosis.
Atypical migraine subgroups
Results of the present study indicated that patients who received the IHS 1.7 designation did not converge to form a homogeneous group of patients with migrainous headaches. Rather, five distinct and clinically relevant subgroups could be distinguished within the IHS 1.7 category: (a) unremitting migraine (Unremitting); (b) migraine exceeding the 72-h duration criteria specified by IHS (Greater than 72 h); (c) migraine episodes that fell below the minimum duration criteria of 4 h (Brief Headache); (d) migraine with atypical headache pain parameters (Pain Characteristics); and (e) migraine without the usual associated non-pain symptoms (Associated Symptoms).
A small subgroup (Associated Symptoms; n = 9) among the IHS 1.7 patients denied symptoms of nausea, vomiting or photophobia and phonophobia that customarily are associated with migraine. Another small subgroup of patients with atypical migraine (Pain Characteristics; n = 16) failed to endorse the pain characteristics typical of migraine. The Associated Symptoms and Pain Characteristics subgroups tended to exhibit lower pain severity than Migraine patients (IHS 1.1, 1.2 and 1.4) and the other atypical migraine subgroups (Unremitting, Greater than 72 h duration and Brief Headache). Thus, patients falling in the Associated Symptoms and Pain Characteristics subgroups may genuinely experience atypical migrainous headaches and be aptly classified with an IHS 1.7 code.
Brief migraine
Another subgroup of patients reported migraine attacks that were shorter than the 4–72 h headache duration defined by IHS (Brief Headache; n = 18). These patients tended to be younger than the patients who fell within the other atypical migraine subgroups or patients who fully met IHS migraine criteria (without and with aura). The observation that headache tends to be of shorter duration in children and adolescents than in adults has been well documented in the paediatric migraine literature (15, 16, 18–22). It is possible that migraine of brief duration may reflect a developmental phenomenon and the headaches of patients in the Brief Headache subgroup may, on average, increase in duration with advancing age. Future longitudinal studies would test this hypothesis. Accordingly, a provision has been made in the IHS criteria to allow for brief migraine attacks among children and adolescents under the age of 15 years with migraine (2–48 h for paediatric headache vs. 4–72 h for adults) (1). Some researchers have suggested that the minimum headache duration criterion for paediatric migraine should be reduced to: (a) below 2 h (15); (b) 1 h (19, 23–25); or (c) 30 min (22). In fact, Gherpelli and colleagues (26) found that entirely excluding the headache duration criterion increased the sensitivity without decreasing the specificity of paediatric migraine diagnoses.
With respect to adults, one investigator has suggested that brief migraine attacks lasting between 2 h and 4 h should be diagnosed as ‘Borderline Migraine’ (27). However, it may prove sufficient to simply modify the IHS criteria for adult migraine disorders to include patients with brief headache episodes that are otherwise migrainous in nature, thus allowing many patients who presently fall into the 1.7 ‘Brief Headache’ subgroup to fully meet IHS migraine criteria. The latter approach appears to be favoured by Rasmussen, Jensen and Olesen (7) who have argued in favour of reducing the lower limit of the IHS migraine duration criterion from 4 h to 2 h, and it was the approach adopted in the revision proposed herein. That criterion revision allowed half of the patients originally assigned to the Brief subgroup (9 of 18 patients) to be reclassified as experiencing Episodic Migraine. Furthermore, the revised Brief Headache subgroup no longer differed from other groups on mean age, thus the revision effectively integrated younger migraine patients having shorter headaches into the Migraine classification. After the revision, nine patients remained in the Brief Headache subgroup with an average headache of less than 2 h duration. These remaining patients appear to experience particularly brief migraine attacks that may be considered truly atypical, and thus an IHS 1.7 diagnosis appears warranted.
Chronic migraine
The largest subgroup of patients with atypical migraine in the present study was the 48% of IHS 1.7 patients who reported headaches that exceeded the 72-h IHS headache duration criterion for migraine (i.e. the Unremitting and Greater than 72 h subgroups). These two subgroups did not differ on clinical variables such as age, pain characteristics, medication overuse or other headache variables. Since the Greater than 72 h subgroup exhibited an average of more than 6 headache days per week, at least some patients in the Greater than 72 h subgroup, along with all of the patients in the Unremitting subgroup, could be characterized as experiencing ‘near daily’ or ‘chronic daily headaches’.
Among headache specialists in the United States and in Europe, the diagnosis of patients with daily or near daily headache has been a topic of debate. Some researchers have proposed revisions to the IHS nosology to help account for the substantial proportion of patients with migrainous headaches that do not conform to the IHS characterization of episodic migraine because their headaches are unremitting or of long duration. Additional diagnostic categories have been proposed that attempt to account descriptively for the chronic migraine phenomena (in some cases with a presumed aetiology of analgesic overuse), including ‘chronic daily migraine’, ‘transformed migraine’, ‘near-daily headache’ or ‘chronic migraine’ (4, 28–35), and a few systematic efforts have been made to develop and test operational criteria for this headache phenomenon (4, 31, 36, 37).
Other researchers have disputed attempts to alter the IHS diagnostic criteria to include chronic daily headache (38). They have contended that there is no compelling evidence to classify daily or near-daily headaches in a diagnostically distinct category. Rather, they have asserted that these headaches can most appropriately be classified using multiple diagnoses available within the existing IHS nosology. They might argue, for example, that what others would label ‘transformed migraine’ might better be diagnosed using separate IHS diagnoses of migraine and chronic tension-type headache; when analgesic overuse also is present, it is represented with the addition of the IHS 8.2 diagnosis. Olesen and Rasmussen (38) asserted the multiple diagnosis approach may facilitate effective management because each headache diagnosis identified may require a different therapeutic intervention.
In the present study, none of the patients within any of the IHS 1.7 subgroups met diagnostic criteria for tension-type headache (IHS 2.1–2.2). The headaches of patients in the sizeable Unremitting subgroup were migrainous in nature but unremitting in duration. Thus, the Unremitting group in this study could not be correctly classified using a combination of IHS tension-type and migraine diagnoses. Whereas some of the Unremitting patients met criteria for medication overuse (IHS 8.2) that may have contributed to their ‘atypical migraine’ presentation, certainly not all Unremitting patients overused medications, thus demonstrating that daily or near daily migrainous headache can occur in the absence of medication overuse.
Many studies implicate daily analgesic use in the ‘transformation’ or ‘evolution’ of headache from episodic to daily or near daily (28, 30, 31, 39–41). In the present study, 74% of the patients within the Unremitting subgroup met medication overuse criteria for IHS 8.2 (Headache induced by chronic substance use or exposure). Indeed, Unremitting patients were significantly more likely than individuals with episodic migraine (i.e. the Migraine group including IHS 1.1, 1.2 and 1.4) to overuse both prescription and non-prescription medications. It is notable, however, that even though their headaches remained episodic, 46% of the Migraine patients also met diagnostic criteria for possible analgesic overuse. Thus, medication overuse could not completely account for the differences in symptom presentations among patients with migraine vs. unremitting migrainous headache. Hence, findings in the present study would not be explained solely on the basis of a transformational concept.
Revision of IHS criteria pertaining to chronic migraine
The diagnosis of patients with daily or high frequency migraine headache has troubled clinicians and researchers for many years. The diagnostic debate seems to stem largely from differences of opinion regarding aetiology or pathophysiology of frequent headache rather than whether or not the phenomenon of chronic migraine exists. Olesen (42 p. 94) lamented the difficulties of the nosology development process because ‘… nosographic knowledge in the headache field is very limited’, and he cited ‘chronic daily headache’ as an issue that required specific clarification.
Nappi and colleagues (43) reviewed three proposed revisions to the IHS diagnostic criteria offered to account for chronic daily migrainous headache. The first by Solomon and colleagues (37 p. 367) proposed the diagnostic category of ‘1.8—Chronic daily headache evolved from migraine’, with a third digit sub-classification for those headaches without and with medication overuse (1.8.1 and 1.8.2, respectively; p. 367). Their 1.8 diagnosis would pertain to those cases in which headaches occurred on at least 6 days per week. Silberstein and colleagues (34 p. 4) also proposed criteria for ‘1.8—Transformed migraine’ that employed a third digit designation for medication overuse, and specified that headaches must occur ‘daily or almost daily (more than 15 days/month), head pain for > 1 month’. Manzoni and colleagues (44 p. 42) recommended that the present 1.7 IHS code should instead be termed ‘1.7—Evolution of migraine’ with a third digit coding for ‘Migraine with interparoxysmal headache’ (1.1.7) vs. ‘Chronic migraine’ (1.7.2). Their ‘chronic migraine’ sub-classification included patients with headache fulfilling IHS 1.1 criteria, but with ‘headache for at least 6 days a week for at least 1 years’ (44 p. 42). Each of these various proposed revisions to the IHS criteria is predicated upon a history of evolution or transformation from episodic migraine to chronic migraine.
The authors of the present study proposed still another approach to revising to the IHS diagnostic classification of migraine. The proposed revisions included two principal alterations of the original IHS criteria including: (a) decreasing the minimum headache duration criterion from 4 h to 2 h, and (b) the development of ‘episodic migraine’ and ‘chronic migraine’ classifications that parallel the present IHS ‘episodic tension-type’ and ‘chronic tension-type’ headache. Furthermore, an attempt was made to formulate a revision that would be in keeping with IHS attempts to provide operational diagnostic criteria that avoid presuppositions about pathophysiology in the absence of clear empirical evidence. Within this scheme, medication overuse would continue to be represented by the IHS 8.2 code.
Using our proposed nosology revision, only 16% of the clinical sample of migraine patients received an atypical designation compared with 36% using the IHS criteria as presently written. The revised minimum headache duration criterion of 2 h allowed 9 of 18 of the headache patients in the Brief Headache subgroup to be reclassified as ‘Episodic Migraine’. Likewise, with our revised criteria the majority of the patients with frequent migrainous headaches could be assigned an actual migraine diagnosis rather than being relegated to the 1.7 category.
The new ‘Chronic Migraine’ diagnosis subsumed the patients whose headaches met all existing IHS 1.1 migraine criteria with the exception of duration. This included all of the patients in the original Unremitting subgroup and two-thirds of the patients in the original Greater than 72 h subgroup, those with headaches 15 days per month or more. Three of nine patients in the Greater than 72 h subgroup retained a 1.7 ‘atypical’ code according to the revised classification because their headaches lasted more than 72 h but occurred fewer than 15 days per month (including, for example, patients with ‘menstrually related migraine’). Notably, some patients previously diagnosed as having IHS 1.1 or 1.2 according to the original criteria were reclassified as having ‘Chronic Migraine’ under the revised system. The reclassification from IHS ‘migraine’ to ‘chronic migraine’ was considered justified and appropriate for patients with migraine headaches occurring 15 days per month or more for at least 6 months. In such instances, the diagnosis of ‘chronic migraine’ reflecting long-standing, high-frequency headache appropriately draws attention to clinical issues that are often less pertinent for patients with episodic migraine (e.g. increased risk of prescription analgesic overuse, consideration of prophylaxis rather than analgesic or abortive treatment, higher index of suspicion for pain-related disability and other psychosocial sequela of chronic pain). With the reclassification, a relatively large proportion of migrainous patients in the present study (43%) received a ‘Chronic Migraine’ diagnosis, with 41% diagnosed ‘Episodic Migraine’ and the remaining 16% receiving an ‘Atypical Migraine’ designation. Given that the present sample consisted of patients drawn from a headache specialty clinic, the fact that a substantial proportion of patients were diagnosed ‘Chronic Migraine’ is not surprising. It is worth noting, however, that epidemiological studies suggest that the proportion of individuals with chronic daily headache and the number with analgesic overuse are much smaller in the general population than in clinical populations (45).
The stability of these findings and the practical impact of the proposed revisions to the IHS criteria have yet to be determined as this work has not yet been replicated with additional patient samples. Furthermore, although we expect that the diagnostic issues confronting clinicians treating headache patients are similar across clinical settings, the generalizability of these findings has yet to be established. Most particularly, it remains to be determined how well these findings obtained with patients in a specialty headache centre will generalize to primary care settings. Of practical necessity, this headache nosology research is hampered by the need to rely upon information from patients' self-reports and the attendant difficulty that patients often encounter in accurately recalling and reporting their symptoms and symptom patterns.
In sum, with greater than one-third of unselected migraineurs in a large clinical sample receiving an IHS diagnosis of atypical migraine, it is clear that more systematic attention should be directed towards refining the IHS migraine nosology, more specifically to determining why such a large proportion of clinical patients cannot be assigned a standard diagnosis within the IHS scheme. The majority of the patients initially classified as 1.7 or atypical according to the present IHS system received their diagnosis because the duration of their headaches exceeded the limits imposed by the IHS criteria. This study supports earlier literature calling for the re-examination of the headache duration cut-off points used in the IHS diagnostic criteria for migraine. Revising the IHS migraine duration criterion to include migrainous headaches as brief as 2 h for adult (especially younger adult) migraine appears to be a logical extension of diagnostic provisions already accepted for paediatric migraine. Furthermore, the development of an IHS diagnosis for ‘Episodic and Chronic Migraine’ paralleling the present IHS Episodic and Chronic Tension-Type Headache (IHS 2.1 and 2.2) warrants further investigation and consideration. In the present clinical sample, these diagnostic revisions allowed the majority of patients initially classified as IHS 1.7 to receive a standard migraine diagnosis, hence increasing the generalizability of the diagnostic criteria scheme. For each reclassified patient, a standard migraine diagnosis was deemed appropriate in that their headache presentations were indeed ‘typical’ of migrainous patients with respect to pain location, pain quality, severity and associated symptoms. With the proposed revisions to the IHS migraine criteria, the 1.7 ‘atypical’ designation is more precisely reserved for those patients with headaches that are truly atypical in clinically meaningful ways.
Footnotes
∗The ‘Greater than 72 hours’ subgroup is distinct from IHS ‘Status Migrainosus’. According to the IHS criteria, ‘Status Migrainosus’ (1.1.6) is subsumed under the heading ‘Complications of Migraine’ (1.6) and characterizes an ‘attack of migraine with headache phase lasting more than 72 h despite treatment’, presumably in patients who otherwise meet diagnostic criteria for episodic migraine of typical (4–72 h) duration. For the ‘Greater than 72 hours’ subgroup, the lengthy attack duration does not reflect a complication of migraine in the form of an attack of unusually long duration for that patient; instead the long headache duration is typical of the patient's headache episodes.