
Abstract
Migraine is a very common neurological disorder worldwide. Its prevalence is lower in developing countries. There were no data concerning the general population in Benin. We aimed to determine the prevalence of migraine in a rural community of Benin. A cross-sectional study was conducted in a rural area of Abomey from February to April 2003 and included 1113 persons selected by a two-stage survey. A case was defined according to International Headache Society criteria (1988). Of the 1113 persons, 37 had migraine. The lifetime prevalence of migraine was 3.3% (male 2.2%, female 4.0%). The peak prevalence was found in persons in the second decade of life. Higher levels of education were associated with migraine. Migraine without aura was the more frequent form (67.5%). The most frequent triggers of migraine were annoyance (73.0%), exposure to the sun (73.0%), heat (65.0%) and anxiety (51.4%). The low prevalence rate of migraine in Benin confirmed the results of the few available African studies. The disease is severe and occurs in a young population and could lead to a high socio-economical burden.
Introduction
Migraine is one of the most common types of primary headache. It is considered to be a benign disease with a heavy impact on the quality of life and activities of patients.
Its diagnosis is based on history-taking and on the criteria defined by the International Headache Society (IHS) (1). Prevalence rates vary from 3.1 to 26.0% in Europe and the USA (2–7); it is lower in developing countries. The few studies in Africa found the prevalence to range from 3.0 to 7.2% (8–11). The study of Ogunyemi (12) among Nigerian students found a higher prevalence of 16.4%, but the study used the Ad Hoc Committee criteria.
In Benin, only one study has been conducted to estimate migraine prevalence among workers (unskilled workers, 59%) of five companies at Cotonou and found 8.9% prevalence (13). There are no data concerning the general or rural community in Benin.
The aim of this study was to evaluate the prevalence of migraine in a rural community in Benin as well as its clinical and demographic characteristics and triggering factors.
Methodology
Setting
This study was conducted from 20 February to end of April 2003 at Gbêcon-Hounli, one of the subdivisions of Abomey, a historical city in the centre of Benin, which is located some 140 km north of Cotonou, the capital city. The city is famous for its numerous palaces and their paintings relating to the royal lineage. The city has seven subdivisions over a 200-km2 area and its population is estimated to 80 000 persons, with Gbêcon-Hounli accounting for 16 590 inhabitants [8904 (53.7%) women] (14).
Type of study
This was a cross-sectional study including all residents > 15 years old.
Sampling
This was a door-to-door, face-to-face study. Two of the four districts of Gbêcon-Hounli were selected by simple random sampling: the districts of Agnangnan and Zassa with, respectively, 1159 and 890 inhabitants (people > 15 years old in each location 703 and 489) were selected (14).
Sample size
The sample size was computed for an expected prevalence of 8.9% (average prevalence of migraine in a previous study among workers in Benin (13)) with a precision of results of 0.018 and α risk of 5%. The minimal number of subjects was 1001.
Diagnostic criteria
Migraine diagnosis was based on the IHS criteria of 1988 (1). The questionnaire has not been previously validated in our population. It listed criteria of migraine with and without aura and was the same as that used by Henry et al. (6), which has established validity (15,16). This questionnaire was translated and back translated by Beninese neurologists.
Data collection
The study was conducted during the season of rural activities. Therefore, there was very little population movement, which increased the reliability of the study. Interviewers went to houses early in the morning and late in the evening after the day's activities. The six interviewers were medical students trained before the study on the questionnaire and diagnostic criteria for migraine, and selected for their ability to talk the local language (fon) in order to ensure good communication with the interviewees. A standardized data collection sheet was used. It included, in addition to the questionnaire based on IHS migraine diagnostic criteria, all other sociodemographic information (age, sex, profession, level of education, matrimonial status) and all the clinical characteristics (intensity, frequency, duration and type of migraine) as well as triggering factors.
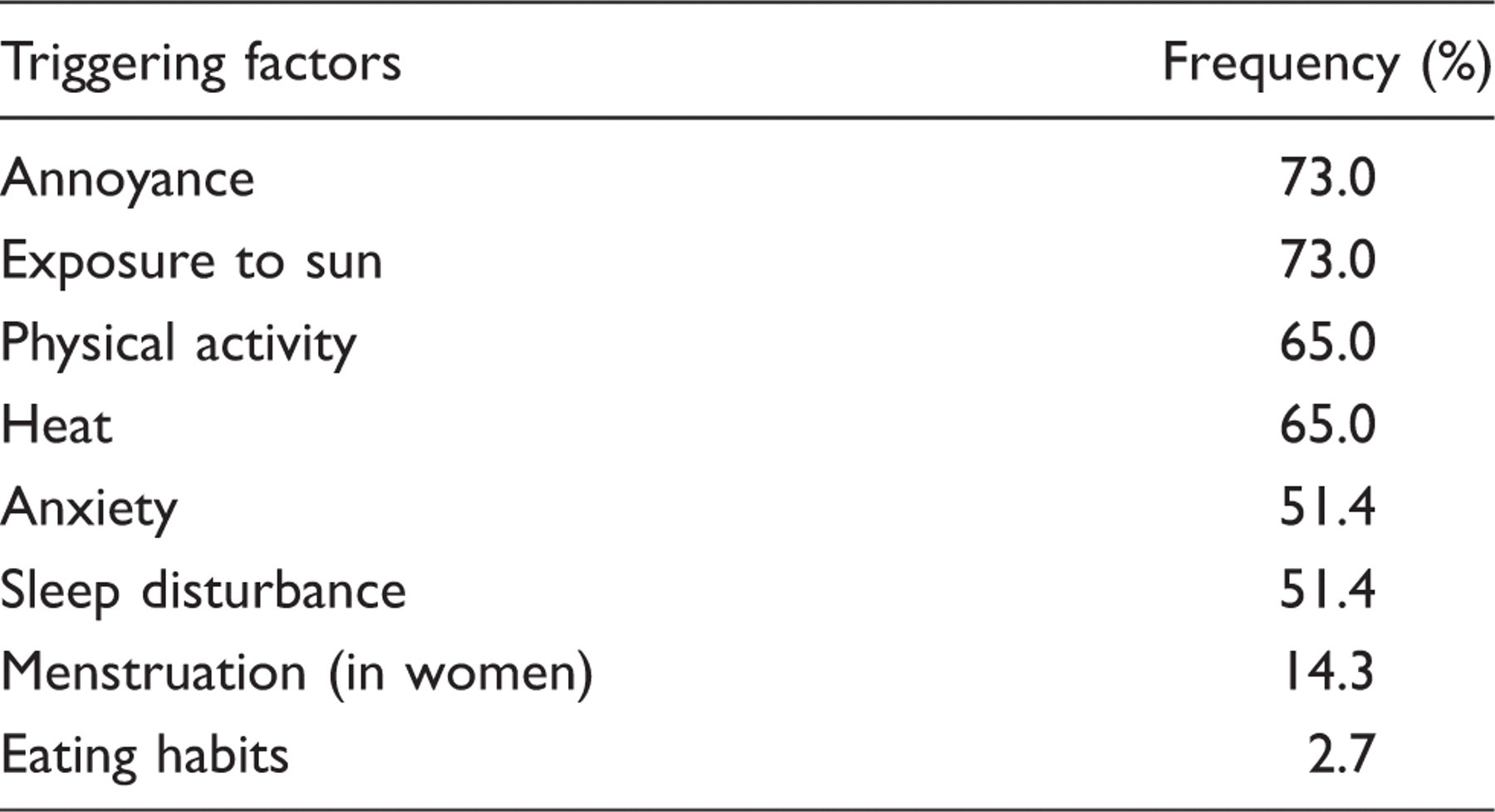
Subjects were asked to mention spontaneously triggers for their headaches or indicate them among those listed (exposure to sun, stress, eating habits, annoyance, sleep disturbance, physical activity, heat, changes in weather conditions and temperature, alcohol, menstruation, anxiety). Data were collected by face-to-face interview. Level of education was defined by illiterate (never went to school and could not read or write), elementary, or college and upwards. We asked people for the frequency of recurrent headaches in the last year.
Subjects considered to have migraine by screening questionnaire secondarily underwent a full neurological examination conducted by a neurologist at the local dispensary to confirm the diagnosis of migraine.
Ethical considerations
The study was authorized by the state health authorities. Subjects were informed before being included in the study and oral consent was obtained.
Data analysis
Statistical analysis was performed by using Epi-Info 6.04C (Ecole Nationale de Santé Publique, Paris, France, and CDC, Atlanta, GA, USA).
Usual descriptive analysis was used: means and standard deviations, proportions, and confidence intervals (CI). χ2 test or Fisher's exact test was used to compare the different proportions. P < 0.05 was considered to be statistically significant.
Results
Of 1192 eligible persons, 58 refused to participate, 21 were not seen, 1113 responded to interviewers. The participation rate was 93.4%. The mean age was 36.8 years (± 17.8) and ranged from 15 to 80 years. Four hundred and seven were male (36.6%) and 706 female (63.4%).
Lifetime prevalence of migraine in a rural community in Benin, 2003

Among the 1113 interviewees, 49 were screened as migraine suffererers and 37 cases of migraine were confirmed. The lifetime prevalence of migraine was 3.3% (95% CI 2.4, 4.6).
Table 1 shows the prevalence of migraine according to sex, age, matrimonial status and level of schooling.
Clinical characteristics of migraine, Benin 2003

The types of aura are not mutually exclusive: one migraineur had visual aura and aphasic, another had sensory and visual aura.
For 16 patients (43.2%), the age at onset was 15 years.
Of the 37 patients, 15 thought that their headaches resulted from one or several factors. Six (16.2%) often recognized those factors, whereas eight (21.6%) recognized them sometimes.
Main triggering factors of migraine in a rural community, Benin 2003
Discussion
Some migraine prevalence studies among populations

AHC, Ad Hoc Committee Criteria; IHS, International Headache Society.
Outside of cultural and racial variations, those differences could be explained by
(20): Sampling methods vary from study to study Data collection through phone survey and self questionnaire is less
reliable The diagnostic criteria for migraine are not the same in all studies Greater tolerance to pain in rural communities and in African culture
than in Western countries Diseases are perceived as of magico-religious significance Low medical accessibility Headaches are not considered as a major health problem compared with
infectious diseases and poverty The triggering factors were not the same in Africa, where exposure to sun
and heat is often reported Possible genetic factors (5).
The prevalence of migraine among the women of Gbêcon-Houégbo was higher than among men, in accordance with other literature data (6,21), but the difference was negligible. This could be explained by the low number of migraine patients in our study. Other reasons could also explain it:
- a high proportion of women in our sample (different from other studies on migraine)
- tolerance to pain is probably higher in women than in men
- the education level is lower in women than in men
- most rural female migraine sufferers are from a low socioeconomic background and are less educated.
Subjects < 20 years old had a higher prevalence of 6.4% and then as age increased the prevalence of migraine surprisingly decreased. Henry et al. (6) found a peak in prevalence in subjects aged 30–40 years. Similar results were obtained by Bigal et al. (21). His study of > 145 335 people living in three large American cities found a high prevalence in the age range 30–39 years regardless of sex or type of migraine (IHS or probable). In a rural community in Ethiopia (9) the authors find a high prevalence in the fourth decade, and in Tanzania Dent et al. (8) find a high prevalence in the fourth decade in women and in the third decade in men. The difference from our study can be explained by the lifetime difference. In our study people were questioned regarding lifetime headache. Elderly migraineurs who had had mild or moderate migraine in their youth and rare occurrences could have forgotten their headaches. Abu-Arafeh and Russel (22) noted a prevalence of 10.6% among school children aged 9–15 years. The same study also observed that migraine occurrence was higher among boys < 12 years and higher among girls > 12 years old.
The prevalence of migraine differed also by level of schooling in our study. Migraine prevalence was higher among people with secondary level schooling. Level of schooling can be a possible confounding factor. Among workers in Cotonou in Benin, Adoukonou (13) find a high prevalence in senior executives. Henry et al. (6) observed a high prevalence among teachers and nurses, whereas low-level workers had a lower rate of prevalence. The majority of individuals had at least one attack per month. This is quite high, and it is possible that the study was not able to capture the milder form of migraine, which could have an impact on the overall prevalence.
Of the migraine patients of Gbêcon-Houégbo, 75.7% had more often severe to incapacitating occurrences of migraine. That number is comparable to the 76.6% of Dent et al.'s study (8) in a rural community in Tanzania. The prevalence of aura was also comparable to other studies in rural communities in Africa. In summary, even if the prevalence of migraine is low in rural Benin, it affects young people and is severe with frequent and incapaciting attacks. This leads probably to a high burden on society.