
Abstract
We set out to assess the prevalence during the previous year of migraine in a rural area surrounding the Mnero Diocesan Hospital in Southern-Tanzania. A door-to-door survey from August until December 1999 using a questionnaire based on the criteria of the International Headache Society (IHS), including 1047 households with 3351 persons, was done, consisting of a screening dialogue with a representative family member followed by a face-to-face interview with the affected subject. Of the 3351 participants (female 1876; male 1475; age > 10 years), 23.1% had suffered from headache during the past year; overall prevalence of migraine was 5.0% (female 7.0%; male 2.6%); 1.4% reported migraine without aura (female 1.8%; male 0.9%); and 3.6% reported migraine with aura (female 5.2%, male 1.6%). The peak prevalence was found in female persons in the fourth (11.1%), in male persons in the third decade of life (3.8%). Compared with other African surveys, the prevalence rate of migraine headache in South Tanzania is slightly higher than among Ethiopian and Zimbabwean Africans.
Introduction
Headache is a widespread symptom of several diseases and a frequent cause of medical consultation (1). Eighty percent of the general population in developed countries have been reported to suffer from headaches (2–4), but also in the population of developing countries, e.g. among university students in Nigeria, approximately 70% report recurrent headaches (5).
Among the different types of headaches, migraine is one of the most debilitating, adolescents and young adults being at highest risk. Recurrent headache is found to interfere with normal daily activities and productivity, results in absence from work, and constitutes a major health problem to every country in the world (6).
The prevalence of migraine and other headache types has been estimated in more than 70 population-based studies. As a result, the body of knowledge about the prevalence of migraine in developed countries has grown considerably. However, little is known about the prevalence and distribution of headaches in rural areas of the African continent (5–13).
Several difficulties exist when comparing the prevalence of headache in Africa with developed countries. For example, in addition to the small number of studies carried out in Africa, a major problem inherent to these studies is the use of different headache classifications (AHC, IHS, etc.) and in general the lack of objective laboratory parameters for correlation of headache data. Very few series used the Diagnostic Criteria and Classification of the International Headache Society (IHS) (14), which established the international guidelines for classification of headache used in epidemiological and clinical studies. Therefore, it is difficult to interpret and compare the results of African studies with those of other parts of the world. Moreover, most of the previously published African studies dealt with selected populations, such as hospital patients or university students. Those conducted in Tanzania investigated patients from hospitals and selected groups of the general population (6, 13). However, none has yet been focused on the general rural population.
The objective of this study was to report the prevalence of migraine headache in a rural African population. A door-to-door survey was carried out and involved a total of 3351 participants living in four distinct villages in rural Tanzania. IHS criteria were used to classify the presence of migraine.
Methods
Sample
The rural villages Mnero, Kitandi, Miembeni and Ruvumu, located 25 km north-west of Nachingwea, Lindi-Region in the south of Tanzania with a stable population of approximately 10 000 inhabitants, were selected for the survey. Due to its geographical isolation and the low rate of population fluctuation, this region was chosen to limit selection bias.
The data were obtained by a team of a well-trained last-year medical student from Austria, a local senior nursing officer serving as interpreter who was in charge of the nursing service of Mnero-Diocesan-Hospital, and finally the respective village executive officers from the participating villages. A local supervisor, working as a physician at the Mnero-Diocesan-Hospital, was available in a supportive and standby capacity. Members of the investigative team were selected based upon specific personal qualities to ensure maximum villager compliance in answering the questionnaire. The presence of an elderly, respected senior nursing officer as the translator and the village executive officer, who were both perceived as important authority figures, encouraged the villagers not only to participate but to give careful consideration to all questions.
Survey
The study was approved by the ethics committee of the Muhimbili University College of Health Sciences, Dar es Salaam, Tanzania.
Following approval of study participation by the village executive officers, 1047 households with 3351 people were investigated by the survey team in the 5-month period from August to December 1999. The procedure started with an informed consent to the representative head of the family or a substitute informing him about the voluntary character of his participation. He was then asked about the demographics of his family. Headache screening was conducted by posing the questions: ‘Are you or a family member subject to headache?’ and ‘Did you or a family member have headache in your lifetime?’. Receiving a positive headache history of any family member was followed by a personal interview and investigation of the respective patient by the team. For those very few individuals unable to understand or respond (e.g. due to mental retardation, dementia, psychosis or aphasia) an immediate family member living with the individual was used as a proxy. Children under 11 years of age were excluded from the study due to the complex nature of some of the questions in the survey and the need for reliable data.
Clinical features and case definition
Demographics, general headache symptoms, and symptoms suggestive of migraine with and without aura during the previous year were registered by using a standardized questionnaire to be completed by each study participant.
The initial step was to obtain demographic information regarding a certain family by interviewing the representative head of that family or a substitute. In the event that a positive history of headache for any family member was established, a face-to-face interview was done with the affected subject.
To quantify headache severity, its effect on activities of daily living (ADL) [according to Garcia-Pedroca et al. (15)] was recorded with the following two questions:
Have you had a severe or a very severe headache during the previous year?
In case of positive answer to this question: Did you decrease your ADL by half or more its normal amount?
The meaning of ‘severe’ or ‘very severe’ was left to the judgement of the subject and the interviewer was instructed not to attempt further definition. Positive answers to both questions were defined as ‘severe or very severe and incapacitating headaches’. A positive response to question 1 alone was defined as ‘severe but not incapacitation headaches’. Certainly the reduction of the ADL involves additional features besides those of pain severity and can not be reflected accurately in this manner (15).
Subjects were diagnosed in accordance to the most frequent type of headache experienced in the last year, using the IHS criteria (14).
Statistical analysis
All data were reported manually during the survey and evaluated afterwards in co-operation with the ‘Institute of Bio-Statistics and Documentation’ at the University of Innsbruck, Austria. For analysing data, Epi Info, Version 6.04b, a word-processing database and software for statistics for public health from the Centers for Disease Control & Prevention (CDC) (Atlanta; GA, USA), was used and the χ2 test with a 5% level of significance and 95% exact confidence intervals by binominal distribution was performed.
Results
The investigated population of the villages of Mnero, Kitandi, Miembeni and Ruvumu over the age of 11 years was composed of 3351 persons, equivalent to 1047 households (demographics are shown in Fig. 1). Including children up to 11 years old into the population structure analysis, > 50% were younger than 20 years, a situation reflecting the typical population structure of a developing country. There was a slight predominance of females (male 1475, female 1876). The examined village residents had a low standard of living compared with western standards. All women were housewives (with the exception of a few nurses, being employed by the hospital) and more than 90% of the households earned their living by farming on a subsistence level, without irrigation or modern farming methods. The remaining study participants were hospital employees, retailers, teachers, and workers in different skilled trades.
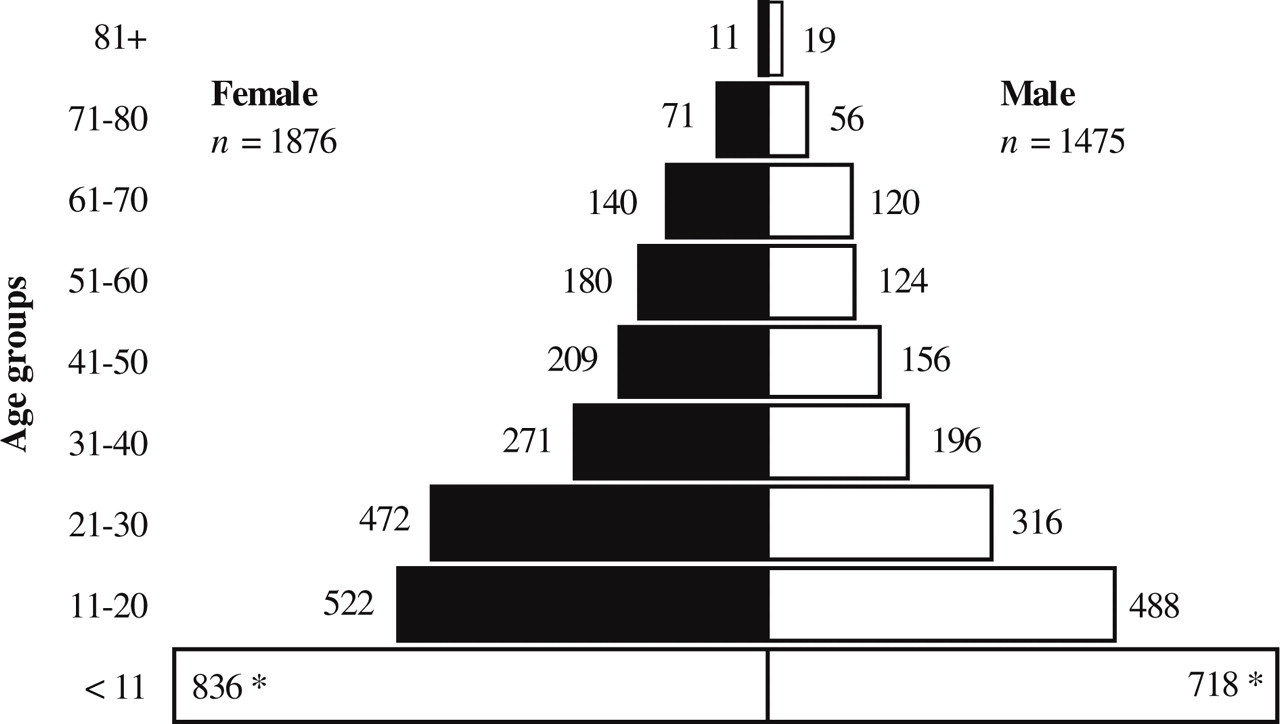
Distribution of study population by sex and age. ∗Children ≤ 10 years old were excluded.
A total of 773 [23.1%; 95% confidence interval (CI) 21.2, 24.5) responded positively to the screening question concerning the presence of headache during the previous year; 278 (18.8%; 95% CI 16.2, 20.8) were males and 495 (26.4%; 95% CI 24.4, 29.0) females (Fig. 2). The general headache ratio between males and females was 1 : 1.4 (P < 0.001).

One-year prevalence of all headaches by sex and age group with 95% confidence intervals. ∗P < 0.05 (ratio male to female). ▪, All headaches in females; □, all headaches in males.
Amongst the 773 headache sufferers, a total of 167 respondents met the case definitions of migraine that also included chronic daily (migraine) headache (Fig. 3), resulting in a 1-year prevalence of 5.0% (95% CI 4.3, 5.7); 2.5% (n = 37; 95% CI 1.5, 3.6) in males vs. 6.9% in women (n = 130; 95% CI 5.4, 8.5) with a male : female ratio of 1 : 2.8 (P < 0.05). The peak age-specific prevalence rate was seen in males in the third decade of life (3.8%), in females in the fourth decade (11.1%) (Fig. 3).

One-year prevalence of migraine headache by sex and age group with 95% confidence interval. ∗P < 0.05 (ratio male to female). ▪, Migraine in females; □, migraine in males.
Of the rural Tanzanian population, 1.4% (n = 47; 95% CI 1.0, 1.8) suffered from migraine headaches without aura (Table 1). Females had been affected in 1.8 (n = 33; 95% CI 1.2, 2.4%) and males in 0.9% (n = 14; 95% CI 0.5, 1.4) of the cases, with a male : female ratio of 1 : 1.9 (P < 0.01).
Prevalence of ‘migraine without aura’ and ‘migraine with aura’ by sex and age groups in the population of Mnero, Kitandi, Miembeni and Ruvumu, Southern Tanzania

Of the investigated population, 3.6% (n = 120; 95% CI 3.0, 4.2) fulfilled the criteria of migraine with aura: 97 females (5.2%, 95% CI 4.2, 6.2) and 23 males (1.6%; 95% CI 0.9, 2.2) with a male : female ratio of 1 : 3.3 (P < 0.001). The peak age-specific prevalence rates occurred among males in the third, among females in the fourth decade (Table 1).
Three cases initially suggestive of migraine headache were later excluded because of the inability to conduct personal interviews.
Of the 167 respondents reported to be suffering from migraine, a total of 128 individuals (76.6%) indicated they had experienced ‘severe or very severe and incapacitating headaches’. The remaining 39 persons (23.4%), reported ‘severe but not incapacitating headaches’. Comparing the frequency of ‘severe or very severe and incapacitating headaches’ in aura-negative (35/47) and aura-positive (91/120) migraine sufferers revealed no significant difference (P > 0.05).
Discussion
This is the first ‘community-based’ prevalence survey of headache, especially migraine headache, in a rural population from Southern Tanzania. A low rate of population fluctuation, the isolated nature of the investigated area, short distances between the villages that afforded the possibility to reach the inhabitants by foot, and the ability to exclude selection bias by carrying out the study by employing a door-to-door survey all characterized the study population. The reliability of the evaluated data was guaranteed by employing the IHS classification system which offers a high level of objectivity within practical application. Since Southern Tanzania is the home of a typical East African rural native population with characteristic occupational and economical features, data collected in this region could be extrapolated to estimate the headache prevalence of East Africa.
According to our study, the prevalence of migraine in Southern Tanzania is slightly higher than in other African countries: 5.0%, compared with 3.0% in Ethiopia (10), and 4.2% in Zimbabwe (12) (Table 2). Due to a lack of clear prevalence period definitions (5, 7–9) and the selective nature of the investigated populations, i.e. hospital patients (11, 13) and students (5), seen in prior surveys, data correlation or comparison with other African studies cannot be conducted in an objective manner. While hospital-based studies are able to obtain detailed clinical data by repeated observation and clinical examination, they might not reflect the actual prevalence in the general population.
Prevalence of migraine in various African countries

The prevalence of migraine in Southern Tanzania is lower than the rate seen in western countries. In Europe reports range from 7.5% in Hungary (16) to 27% in Germany (17), and in North America a rate of 12–15% in the USA (18) and Canada (19) was documented. This finding is similar to other studies originating from Africa, which also revealed lower migraine prevalence in Africa compared with western countries (10, 12). There are no sound scientific data to account for these differences; however, there are some possible explanations.
One reason for lower migraine prevalence in Africans might be the differing age distribution structure observed in developing countries. Since the highest incidence of migraine is observed in the third and fourth decades of life and more than one-third of our study participants were ≤ 20 years of age, a typical statistic for developing countries, a large proportion of ‘future migraineurs’ might have been lost in this survey. Therefore, population structures should be taken into account when comparing migraine prevalence in Africa and western countries.
Second, cultural reasons may account for this observed difference. People from developing countries may have a higher pain threshold because of more urgent concerns like starvation, the threat of more disastrous diseases such as malaria, meningitis, etc. Compared with these illnesses headache might seem a minor problem. From an economic and social point of view, it is probably not acceptable to complain about ‘minor sicknesses’ such as headache, because any illness might result in an immediate loss of income and/or food. Taking into account that over 75% of our migraine patients were suffering from ‘severe or very severe and incapacitating headaches’, this finding might support the hypothesis that ‘minor sickness’ in a population such as ours was not worth complaining about, due to its unacceptability in the family and community.
Third, several lines of evidence suggest that racial differences are responsible for variations of migraine prevalence throughout the world. Previous epidemiological studies concerning migraine have demonstrated the role of genetic (20–22) and socio-demographic (18, 23, 24) risk factors. Stewart and colleagues (25) compared migraine prevalence in Caucasians, African-Americans, and Asian Americans in the USA. They examined the impact of differences in racial origin and their possible influence on migraine prevalence. They found a remarkable variance in migraine prevalence amongst distinct racial groups, with high frequency among Caucasians (100%) and low prevalence in African (75%) and Asian Americans (50–60%). Therefore, Mnero and its surrounding villages comprise an individual group of native people reflecting a unique genetic aggregation, which could make them less prone to migraine in general. In the same way, this could explain the surprising finding that migraine with aura was more common than migraine without aura.
The particular finding of higher migraine with aura prevalence can also be explained by the methodology of our survey. As mentioned earlier, the head of the family or a substitute was asked to report on any headache symptoms in his family. A possible consequence of this technique was that only clinically and socially relevant symptoms were probably reported to this individual, which could have resulted in the underreporting of ‘less serious’ migraine without aura headaches. In the same way, since children and adolescents were the predominant study participants, they might be more inclined to recall the disturbing attacks with aura, leading to higher frequency of recordings of migraine headaches with aura. Another likely explanation for the high percentage of aura-positive migraine could be the possible existence of transcultural misunderstanding. However, due to the presence of a medically well-trained and experienced interpreter, the chance of such a misunderstanding occurring was reduced to a minimum.
In addition to a variety of differences, our survey revealed certain similarities with studies derived from developed countries. Consistent with western studies (1 : 2–3.5), women displayed a higher prevalence of migraine in all age groups (male : female ratio of 1 : 2.5), which is the peak prevalence of migraine in both men and women between 31 and 40 years of age, similar to results generated in studies from the USA (18), Canada (26), and Hungary (16).
In summary, this survey demonstrates that migraine headaches are not uncommon in a rural population of Southern Tanzania. It showed a lower migraine frequency than in western countries but higher than in China, where prevalence rates from 0.6 to 1.0% have been reported (26–28). However, due to the retrospective character of data collection and the lack of personal interview with each study participant, there are some limitations. Headache prevalence data from Africa remain scanty and the study therefore adds useful information regarding migraine prevalence on this continent. Many speculations regarding the differences in headache frequency in Africa, Asia and western countries have been voiced, but further investigation should lead to a better understanding of questions surrounding this topic.
Footnotes
Acknowledgements
We are indebted to Mzee Mkwela, Sister Emakulata, Mama Coletta and Dr E. Kasuluzu for their support and contributions, and to all participants who took part in this study.