
Abstract
We conducted a 3-year annual questionnaire survey of the International Headache Society (IHS) migraine diagnoses among 2414 adolescents aged 13. For those with migraine without aura (IHS 1.1) at the baseline survey (n = 89), 28% and 24% retained the IHS 1.1 diagnosis at the 2nd and 3rd surveys. Only 0.5% of adolescents had a persistent IHS 1.1 diagnosis for 3 years. Of those with IHS 1.1 or migrainous disorder (IHS 1.7) (n = 449), 43% and 48% retained the IHS 1.1 or IHS 1.7 diagnosis at the 2nd and 3rd surveys. Conversion between IHS 1.1 and IHS 1.7 was common. About 5.6% of the adolescents suffered from IHS 1.1 or IHS 1.7 for all 3 years. Independent predictors for persistent IHS 1.1 or IHS 1.7 diagnosis included frequent headache (> 5 days/month) (relative risk (RR) = 1.8) and pulsatile headache (RR = 1.5). The diagnosis of IHS 1.1 in adolescents was quite unstable. Conversion between IHS 1.1 and IHS 1.7 was an important cause. Factoring IHS 1.7 into the spectrum of migraine diagnoses during epidemiological surveys provides a realistic impression of the disease burden in this age group.
Introduction
Migraine is a common headache disorder in adolescents and frequently causes disability and school absence (1, 2). The standard classification criteria for migraine outlined in the 1st edition of the International Headache Society (IHS) in 1988 (3) have been adopted in all recent epidemiologic surveys; revisions of the criteria for children and adolescents have been suggested (2, 4, 5). The diagnostic criteria for migraine in children and adolescents were not changed significantly in the 2nd edition of the International Classification of the Headache Disorders (ICHD-II), published in 2004 (6). In the notes, it is mentioned that ‘in children, attacks may last 1–72 hours’ as compared with ‘2–48 hours’ in the 1st IHS edition (3, 6). Moreover, ‘migrainous disorder not fulfilling the criteria’ (IHS 1.7) is renamed as ‘probable migraine without aura’ in the new edition (coded as ICHD-II 1.6.1) (6). IHS 1.7 is diagnosed if one of the diagnostic criteria of migraine is not fulfilled (3). In previous studies, the most common unfulfilled criterion in the diagnosis of IHS 1.7 is short duration of headache. Children and adolescents frequently report headache duration of less than 2 h (2, 7). IHS 1.7 is seldom included in the migraine spectrum in epidemiologic surveys of migraine in adolescents (2, 8) even though many patients with migraine and IHS 1.7 frequently convert to the other diagnosis at follow-up (9, 10).
The evolution of migraine diagnoses over time in adolescents has not been fully investigated. The prognosis in juvenile migraineurs is generally considered to be favourable; nevertheless, there is a subgroup of patients who suffer from a protracted course of the illness (1, 11). In our pilot study, we validated a headache questionnaire that was used to survey migraine among 13- to 15-year-old adolescents in 4 junior high schools (12). In the present study, we used the same paradigm to diagnose migraine in a cohort of 7th graders from 5 junior high schools over a period of 3 years. Our goal for this study is to report (1) the evolution of adolescent IHS migraine diagnoses over time (2), the predictors for the persistence of migraine diagnoses in this age group, and (3) the significance of the addition of IHS 1.7 to the migraine spectrum at follow-up.
Subjects and methods
Study design
A population-based questionnaire interview was conducted for 3 consecutive years among all students in 5 sampled public junior high schools during the study period of 1999–2001. Since the study focused on the trend of migraine diagnosis, we surveyed the 1-year prevalence (i.e. the headache profile in the previous year).
Targeted population
In order to obtain a nationally representative sample, we chose 5 junior high schools in different geographical regions of Taiwan, including 2 schools located in northern (Shi-Pai, Ta-Chi), 1 in central (Yun-Lin), 1 in southern (Nei-Pu), and 1 in eastern Taiwan (Yu-Li). Tai-Chi and Shi-Pai, which are located in Taipei City, represented the urban regions of Taiwan. We sampled 2 urban schools because 69% of Taiwanese live in cities. In contrast, Yun-Lin, Nei-Pu, and Yu-Li are rural areas. In Taiwan, education is obligatory between the ages of 6 years and 15 years and includes elementary (age 6–12 years) and junior high schools (age 13–15 years). More than 90% of junior high students are enrolled in pubic schools, and the others attend private schools. Of the 867 junior high schools in Taiwan, 107 are private and they represent 9.4% of the total students.
Sampling method and survey
For logistic reasons, all of the 7th grade students who were enrolled at the 5 sampled schools in 1999 were invited to participate in the baseline study. Two consecutive annual follow-up surveys were conducted using a similar method for case-finding and identical questionnaires.
Letters describing our study objectives and methodology were first mailed to the school principals of the sampled schools for their approval. The students completed a self-administered questionnaire. Data from completed headache questionnaires were analysed by computer algorithm for headache diagnosis.
Headache questionnaire and diagnoses of migraine disorders
A validated self-administered questionnaire developed in our previous study was modified to diagnose migraine in the previous year (12). The questionnaire was based on the 1988 IHS diagnostic criteria for migraine (3), and part of the questionnaire has been published elsewhere (12). A student was diagnosed with migraine without aura (IHS 1.1) if the headache attack lasted 2 h to 48 h (duration) with any 2 of the following 4 pain characteristics: unilateral location, pulsating quality, moderate-to-severe intensity, and aggravation by routine physical activity. Moreover, the attack had to be associated with at least 1 accompanying symptom, including nausea, vomiting, or photophobia plus phonophobia. As in our previous study (12), criterion A (at least 5 attacks) was not mandatory in this study. In addition, subjects were defined to have ‘migrainous disorder not fulfilling the criteria’ (IHS 1.7) if only 2 of the 3 criteria (headache duration, migrainous pain characteristics, and accompanying symptoms) were fulfilled (3, 6). Based on the hierarchy system proposed by the IHS classification, episodic tension-type headache (IHS 2.1) had to be excluded before the diagnosis of IHS 1.7 was made (3). In this study, we did not attempt to diagnose migraine with aura (IHS 1.2) because the validity for this diagnosis was not satisfied (12).
Statistical analysis
The 1-year prevalence of IHS 1.1 or IHS 1.7 was calculated as the number of cases per 100 students. Chi-square test was used to compare categorical variables. Hazard ratio (HR) and 95% confidence intervals (CIs) for the persistence of IHS 1.1 or IHS 1.7 during the 2nd and 3rd surveys were estimated by Cox proportional hazard models. All calculated P-values were 2-tailed and statistical significance was defined as P < 0.05. All statistical analyses were performed using the SAS software version 8.2 (SAS Institute Inc, Cary, NC, USA).
Results
Participants
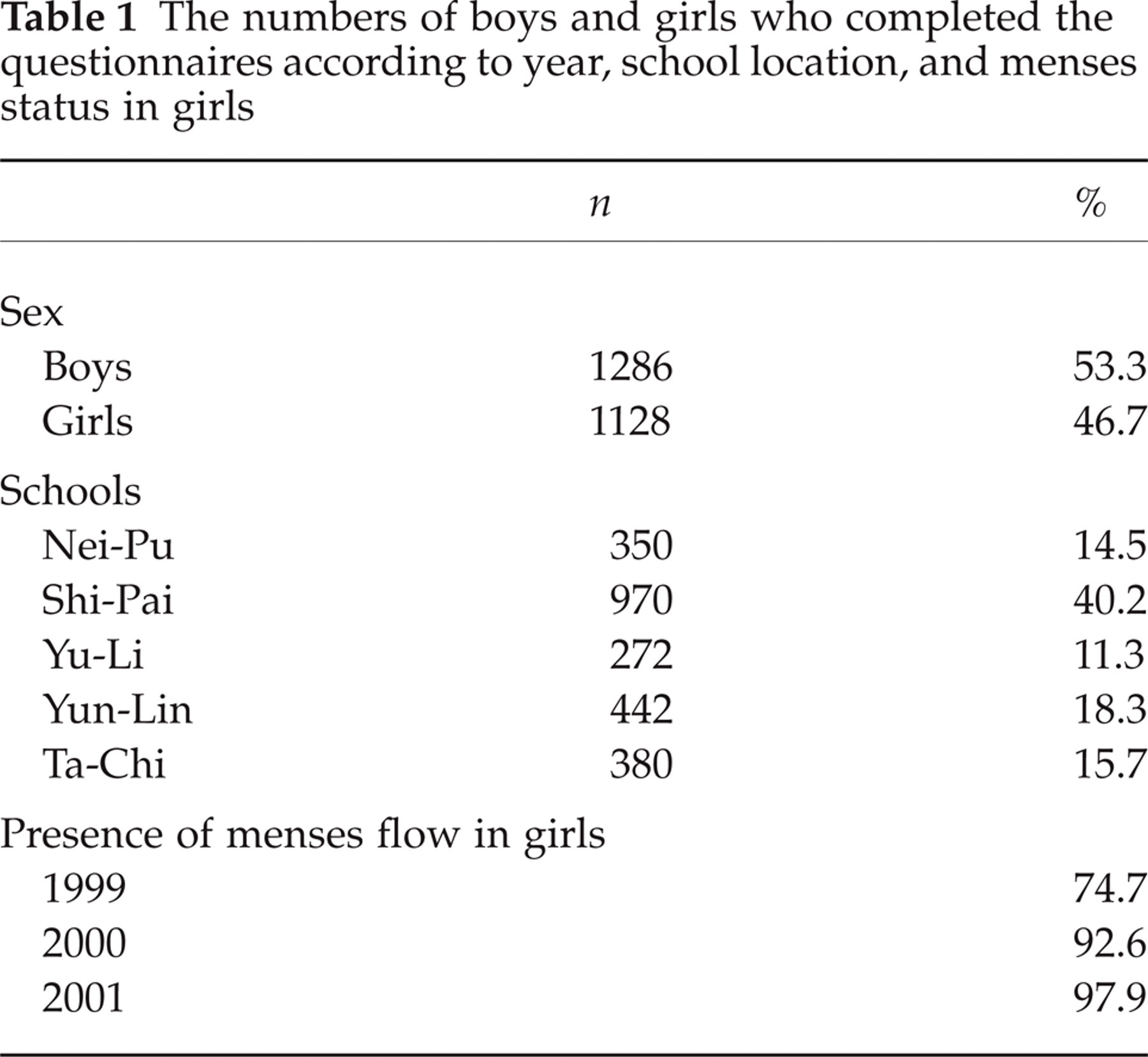
The 2414 adolescents who completed the 3 annual surveys during the study period of 1999–2001 constituted the final sample of this study (Table 1). The overall participation rate for the 3 consecutive years was 91%.
The numbers of boys and girls who completed the questionnaires according to year, school location, and menses status in girls
Prevalence of migraine diagnoses
Among the 2414 participants, the 1-year prevalence of IHS 1.1 was 3.7% (boys 3.3%, girls 4.1%) for the 1st year survey when they were 7th graders, 5.7% (boys 3.9%, girls 7.8%) for the 2nd year, and 8.4% (boys 6.1%, girls 10.9%) for the 3rd year. For the IHS 1.1 diagnosis, 13 students(4 boys and 9 girls) were diagnosed for all 3 years (0.5%), 69 students (30 boys and 39 girls) for 2 of the 3 years, and 252 students (100 boys and 152 girls) for only 1 of the 3 years. The prevalence of IHS 1.1 for at least 1 of the 3 years was 13.8% (boys 10.4%, girls 17.7%).
Diagnosis of IHS 1.7
The prevalence of IHS 1.7 among our participants was 14.9% for the 1st survey, 12.3% for the 2nd survey, and 14.3% for the 3rd survey. The duration of headache (especially < 2 h) was the major reason that one criterion was unfulfilled in the diagnosis of IHS 1.7 in at least 70% of the patients (Table 2). Of those with duration < 2 h, around 50% reported headache duration less than 30 min.
The duration of headache in patients diagnosed with migrainous disorder (IHS 1.7) in 3 annual surveys

Prevalence of the diagnoses of IHS 1.1 or IHS 1.7
Among the 2414 participants, the 1-year prevalence of either IHS 1.1 or IHS 1.7 was 18.6% (boys 14.9%, girls 22.8%) for the 1st year survey, 18.1% (boys 14.1%, girls 22.6%) for the 2nd year, and 22.2% (boys 15.9%, girls 29.3%) for the 3rd year. Those diagnosed with either IHS 1.1 or IHS 1.7 included 134 students(48 boys and 86 girls) for all 3 years, 261 students (110 boys and 151 girls) for 2 of the 3 years, and 497 students (214 boys and 283 girls) for only 1 of the 3 years. The prevalence of IHS 1.1 or IHS 1.7 for at least 1 of the 3 years was 37.0% (boys 28.9%, girls 46.1%).
The trend of the diagnoses of IHS 1.1 or IHS 1.7
Of the 89 adolescents with IHS 1.1 in the 1st year survey, 25 (28%) had the same diagnosis in the 2nd year and 21 (24%) in the 3rd year (Fig. 1a). Overall, only 0.5% (boys 0.3%, girls 0.8%) of the students were diagnosed as IHS 1.1 for 3 consecutive years, comprising 4% (0.5/13.8) of all migraine sufferers diagnosed in any of the 3 annual surveys.
When we added IHS 1.7 to the migraine spectrum, 52% of the IHS 1.1 sufferers (n = 89) at the initial survey were diagnosed as IHS 1.1 or IHS 1.7 in the 2nd annual survey, and 57% were diagnosed as IHS 1.1 or IHS 1.7 in the 3rd survey (Fig. 1a). For those with the diagnosis of IHS 1.1 or IHS 1.7 (n = 449) in the initial survey (Figs 1a,b), 43% (n = 191) acquired the diagnosis of either IHS 1.1 or IHS 1.7 in the 2nd annual survey and 48% (n = 217) in the 3rd annual survey. Overall, 5.6% (boys 3.7%, girls 7.6%) of the students were diagnosed as IHS 1.1 or 1.7 for 3 consecutive years, comprising 15% (5.6/37) of all those diagnosed as IHS 1.1 or 1.7 in any of the 3 annual surveys. In the subjects with IHS 1.1 at the initial survey (n = 89), 44% (n = 39) acquired at least 1 diagnosis of IHS 1.7 in either of the 2 annual follow-up surveys. In contrast, in the subjects with IHS 1.7 (n = 360) at the initial survey, 28% (n = 101) acquired at least 1 diagnosis of IHS 1.1 at either of the 2 follow-up surveys (Fig. 1).
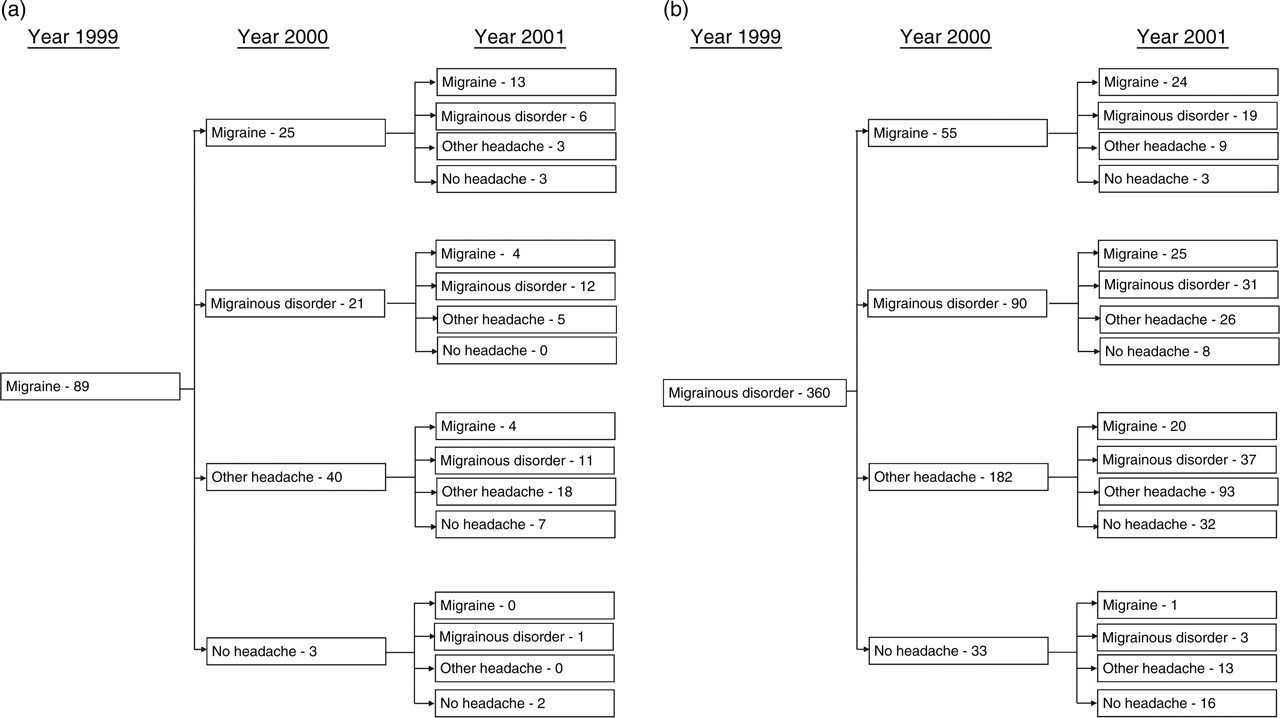
The changes in migraine/headache status in adolescents, taking migrainous disorder (IHS 1.7) into consideration. (a) Patients in this group completed 3 consecutive annual surveys and were diagnosed with migraine (IHS 1.1) at the initial survey (n = 89). (b) Patients in this group completed 3 consecutive annual surveys and were diagnosed with migrainous disorder at the initial survey (n = 360).
Comparisons of follow-up diagnoses for IHS 1.1 and IHS 1.7
Students diagnosed with IHS 1.1 at the baseline survey (33/89; 37%) were significantly more likely to have a diagnosis of IHS 1.1 in either of the 2 following years compared to those diagnosed with IHS 1.7 (101/360; 28%) (P = 0.03). Whereas, the frequencies of acquiring at least 1 diagnosis of either IHS 1.1 or IHS 1.7 at the follow up did not differ significantly between those with IHS 1.1 and IHS 1.7 at the baseline survey (62/89(70%) vs. 206/360 (57%), p = 0.09).
Predictors for persistence of IHS 1.1 or IHS 1.7
According to univariate analyses with Cox proportional hazard models, subjects with either IHS 1.1 or IHS 1.7 who reported greater frequency of headache (>5 days/month vs. ≤5 days/month) (HR = 2.0, 95% CI = 1.2–3.3), pulsatile headache (HR = 1.6, 95% CI = 1.1–2.2), photophobia and phonophobia (HR = 1.7, 95% CI = 1.2–2.4), or exacerbation by routine physical activities (HR = 1.6, 95% CI = 1.1–2.5) were significantly more likely to retain diagnoses of either IHS 1.1 or IHS 1.7 in both of the follow-up surveys (Table 3). Two independent significant risk factors, including greater frequency of headache (HR = 1.8, CI = 1.1–3.0) and pulsatile headache (HR = 1.5, CI = 1.0–2.1), were identified using stepwise multivariate analysis.
Hazard ratio and 95% confidence intervals for persistence of migraine or migrainous disorder in 2 follow-up annual surveys

P < 0.05.
5 days/month was at the 75% percentile of headache frequency per month.
Discussion
This large-scale, nationwide, 3-year annual survey provides us with longitudinal data to observe the evolution of IHS migraine diagnoses in adolescents over time. Of the IHS 1.1 participants diagnosed as 7th graders (n = 89), 28% and 24% retained the diagnosis at the 2nd and 3rd annual surveys. Only 0.5% of the adolescents had IHS 1.1 for 3 consecutive years; 13.8% had IHS 1.1 for at least 1 of the 3 years. Therefore, IHS 1.1 migraine diagnosis among adolescents is quite unstable even for short-term follow-up. The instability of migraine diagnosis, which results from the strict IHS criteria, partly contributes to the favourable prognosis of the disease in this age group.
In line with previous studies (2, 7), we found that the most common reason for diagnosing IHS 1.7 was short headache duration. About 70% of our participants with migrainous disorder reported < 2 h headache duration. It is of note that about half of them reported headache duration less than 30 min (Table 2). Their other headache characteristics or accompanying symptoms were the same as those in patients with IHS 1.1. In our study, the conversion between IHS 1.1 and IHS 1.7 in adolescents occurred frequently. For the subjects with IHS 1.1 at the initial survey, 44% acquired at least 1 diagnosis of IHS 1.7 at follow-up. In the same context, 28% of the subjects with IHS 1.7 at the initial survey acquired the diagnosis of IHS 1.1 at follow-up. High conversion rates between IHS 1.1 and 1.7 have also been reported in previous studies (9, 10). In fact, we found that the frequency of acquiring the diagnosis of IHS 1.1 or IHS 1.7 at follow-up was only slightly higher in those with a diagnosis of IHS 1.1 at the initial survey than those with IHS 1.7. In contrast, two clinic-based studies also demonstrated high frequencies (around 25%) of conversion from migraine to tension-type headache at 8-year and 10-year follow ups; however, neither study took IHS 1.7 into consideration (13, 14). In another recent study, headache attacks in migraineurs, along a spectrum ranging from IHS 1.1 to IHS 1.7 to tension-type headache, were all responsive to sumatriptan (15). These findings support the continuum model of headache (14, 16, 17) which places tension-type headache, IHS 1.7, and IHS 1.1 along a spectrum of severity, based upon the existence of a common biological mechanism.
Adolescent migraine was a much more stable diagnosis when we added IHS 1.7 to the spectrum. About 43% to 48% of those with IHS 1.1 or IHS 1.7 continued to suffer from migraine disorder at the follow-up visits. Also, 5.6% of the adolescents were diagnosed with either IHS 1.1 or IHS 1.7 for 3 consecutive years; this percentage is much greater than the 0.5% of participants diagnosed with IHS 1.1 for all 3 years. IHS 1.1 and IHS 1.7 together represent the realistic trend and disease burden of migraine in adolescents. In previous studies, 40% to 50% of adolescent migraineurs continued to suffer from migraine after a longer follow-up period (1, 10, 11). In a prospective study of 73 children with ‘more pronounced’ migraine, 38% suffered from migraine at the 6-year follow-up (during puberty) (1). At the ages of 30 years and 40 years, 60% and 53% had migraine(23- and 30-year follow-up). At the age of 50 years, more than half of the migraine group still had migraine attacks (11). In an epidemiologic sample of adolescents with migraine, Camarda et al. (10) reported that about half of the patients continued to have migraine attacks at the 5-year follow-up. Two clinic-based studies showed that adolescents with migraine without aura tended to persist in 45% of the study sample at 8- and 10-year follow ups. In addition, these two studies also showed that adolescents with migraine were less likely to become headache-free than those with other headache types (13, 14). Our results and these reports suggest that adolescent migraine is not benign; a significant number of adolescent patients with migraine disorder suffer from a chronic course in short- and long-term studies.
In this study, high frequency of headache and the presence of pulsatile headache were 2 independent predictors for the persistence of migraine disorder at follow-up. Bille (1) also characterized high frequency of headache as a poor outcome predictor. However, in our study, other reported prognostic factors, such as certain combinations of migrainous features or gender, were not identified as risk factors after multivariate analyses (18, 19). Notably, the duration of headache was not a predictor for the persistence of migraine disorder in our study.
Our study has several limitations. First, the diagnosis of IHS 1.1 in our study was accomplished by a questionnaire survey rather than a neurologist's interview. The questionnaire was validated in diagnosing migraine without aura but not migraine with aura. Thus, comparisons to other studies should be made with caution. Second, we did not use the new ICHD-II criterion of headache duration ‘1–72 hours’ for IHS 1.1 migraine diagnosis because of our original questionnaire design. The choice items in our questionnaire for headache duration included only ‘<30 minutes’ and ‘>30 min and <2 hours’ (Table 2) (12). Nevertheless, the prevalence of migraine (IHS 1.1) would be much higher if shorter headache duration were used as a criterion. Third, ethnic and cultural factors affect the prevalence of migraine in different populations(e.g. Asian and Western); therefore, these factors should be considered when extrapolating our data to other populations (20).
In conclusion, the diagnosis of IHS 1.1 in adolescents was relatively unstable; conversion between IHS 1.1 and IHS 1.7 occurred frequently. Independent predictors for the persistence of IHS 1.1 or IHS 1.7 included high frequency of headache and pulsatile headache. Factoring IHS 1.7 into the spectrum of migraine diagnoses during epidemiological surveys provides a more realistic impression of the disease burden in this age group.
Footnotes
Acknowledgements
This study was supported by grants from the National Science Council (NSC 90–2314-B-010–026).