
Abstract
To estimate the prevalence of tension-type headache, migraine and other headaches, 1850 schoolchildren, age 7-15 years, from the city of Uppsala, were invited to complete a questionnaire. The response rate was 74.1%. To validate the information from the questionnaires, 131 children and their parents were interviewed. Using the criteria of the International Headache Society, the 1-year prevalence of tension-type headache and migraine was 9.8 and 11.0%, respectively. However, these prevalence rates increased considerably, to 23.0 and 17.0%, respectively, when excluding the criteria defining the number of earlier episodes and duration of headache. The prevalence of headache increased with age, similarly in girls and boys up to 11 years, and thereafter only in girls. The preponderance in teenage girls was even more pronounced for tension-type headache than for migraine. Our results indicate an increase over time in headache prevalence when compared with findings in a study conducted in the same city in 1955.
Introduction
Headache is a common health problem, often with an onset in childhood. An increasing prevalence of headache in children has been reported (1, 2). In a Finnish study, the prevalence of migraine in 7-year-old children showed a threefold increase when the same age group was studied 18 years later (1.9 to 5.7%), and the total prevalence of headache increased nearly fourfold (14 to 52%) (1). In a cross-national study by the World Health Organization (WHO) including 12 000 children aged 11, 13 and 15 years, the prevalence of headache had increased by 5% in 4 years (2).
There is a paucity of population-based studies investigating the prevalence of tension-type headache (TTH) as defined by the International Headache Society (IHS) criteria (3), especially for studies including both pre-pubescent and pubescent age groups. The prevalence rates from the existing studies vary considerably (12.1 to 72.8%) (4–8). The prevalence of chronic tension-type headache (CTTH), defined as TTH with a frequency of at least 15 days per month for 6 months or more, was reported to be 0.9% in Scottish schoolchildren (9). However, in a Finnish study of 12-year-old children, no child fulfilled the criteria for such headache (6).
The majority of previous prevalence studies on headache in children and adolescents have mainly focused on migraine. In 1955, Bille conducted his pioneering, epidemiological study of headache in schoolchildren from the city of Uppsala, Sweden (10). The prevalence rate of migraine as defined by the criteria of Vahlquist (11) was 3.9%. After the introduction of the IHS criteria in 1988, population-based studies in school-aged children have shown 1-year-prevalence rates of migraine varying from 2.7 to 13.7% (4, 5, 7, 9, 12–14).
Prevalence studies on headache in children and adolescents mainly discussed here are summarized in Table 1.
The prevalence of tension-type headache, migraine and total headache in population-based studies in children and adolescents

Q, questionnaires; I, interviews.
One-year prevalence;
headache during the last 6 months, disturbing daily activities;
lifetime prevalence or time period not defined.
Modified IHS criteria;
modified IHS criteria for migraine.
Sample comprising girls only.
The IHS classification has improved the reliability of headache diagnosis in adults, but the applicability in children has been debated. The IHS criteria for migraine have been modified for children under the age of 15 years by reducing the duration criterion (criterion B), from 4–72 h for adults to 2–48 h for children. No modification has been made for the number of earlier episodes (criterion A). Several authors have suggested a further shortening (12, 13, 15–21) or even exclusion (22, 23) of the duration criterion for migraine in children. In addition, the requirement of five earlier episodes of migraine in a childhood population has been questioned (15). The IHS criteria are currently under revision by the Headache Classification Committee of the International Headache Society.
As there are a limited number of population-based studies on headache in children including both pre-pubescent and pubescent age groups, especially on the prevalence of TTH, the objectives of this study, in a sample of schoolchildren 7–15 years old, were as follows:
To estimate the prevalence of TTH, migraine and other headaches by age and gender, using strict and modified IHS criteria.
To compare the current prevalence of headache with the one reported from the same city by Bille in 1955 for schoolchildren in the same age group (10).
Materials and methods
Study population
The study population consisted of a randomised, stratified, cluster sample of 1850 schoolchildren, aged 7 to 15 years, from public comprehensive schools in the city of Uppsala in 1997. At that time, the total number of schoolchildren aged 7–15 years was 20 531, of which 93.2% attended public schools, 6.0% private schools and 0.8% schools for handicapped children (data from Uppsala municipal administration, January 1997). In order to include a representative sample of schoolchildren, one class from every grade (1–9) was randomly selected from each of the eight districts of the city. Thus, altogether 72 classes distributed on 28 different schools participated in the study. The randomization was proceeded with help of lists of classes in each district and random numbers generated by a computer. The methods used were similar to those reported by Bille (10) in a study from the same city 42 years earlier (1955), and the study population was fairly comparable. Bille included all children aged 7 to 15 years attending public comprehensive schools (n = 9059), and excluded those attending schools for handicapped children, in addition to those aged 13–15 years, who had stopped school or attended vocational schools.
Questionnaires
The teachers distributed questionnaires to be filled out at home together with a parent. The non-responders were first reminded by the teacher and then by a letter sent home.
The questionnaire, which was developed and tested together with Bille, covered the Vahlquist (11), as well as the IHS, criteria (3). However, an important difference to the study by Bille (10) was that, for the current study, children with headache associated with infections or other diseases (i.e. secondary headache) were asked to stop filling out the questionnaire after the initial questions concerning whether they had experienced headache during or previous to last year. The others were asked additional questions about different headache symptoms mainly answered by ‘yes’ or ‘no’, except for questions on the number of earlier episodes, duration, intensity and frequency of headache that were rated into categories.
To validate the information obtained in the questionnaire, a random sample of 131 children, stratified for sex, age and preliminary headache diagnosis, was interviewed and physically examined (by KL). As reported in a previous study (24), the concordance of information from questionnaires and interviews was high. The agreement between headache diagnoses based on questionnaires and interviews increased, and the number of unclassified headaches decreased, when the duration of headache was excluded.
The questionnaire had previously been tested in a sample of 266 schoolchildren aged from 7 to 14 years, of which 35 children were interviewed (25). The agreement between questionnaires and interviews concerning diagnoses of TTH, migraine and unclassified headache was high (85.3%), as was the agreement between diagnoses based on the IHS criteria and diagnoses set by two experienced physicians (BL, OEO) after reviewing the interview responses (88.6%). In an initial version of the questionnaire, answers could be given separately for two types of headaches. However, as only 11% of the children who stated that they had more than one headache type actually received two different diagnoses, we did not use separate response alternatives for different headache types in the present study.
Diagnosis
The IHS criteria (3) were applied for establishing a diagnosis of TTH or migraine. According to the IHS classification, when the criteria for both TTH and migraine were fulfilled, the diagnosis should be migraine. The IHS 2.3 diagnosis was used for headache fulfilling all but one criteria for TTH, but not fulfilling the criteria of migraine with or without aura. Similarly, IHS 1.7 was used for headache fulfilling all but one criteria for migraine, but not fulfilling the criteria for TTH. Overlapping cases were diagnosed as IHS 1.7.
In this study, we modified the IHS criteria in that the number of earlier headache episodes (criterion A) and the headache duration (criterion B) were excluded. For comparison with the study by Bille, the Vahlquist criteria (paroxysmal headaches and at least two of the following: unilateral pain, nausea, visual aura and heredity) were used.
The Research Ethics Committee of Uppsala University approved this study.
Statistical analysis
Associations between categorical variables were analysed using the chi-square test or, when appropriate, the Fischer exact test. The level of significance was set to 5%.
Results
Acceptable questionnaires were returned from 1371 (74.1%) children, 686 girls and 685 boys aged 7–15 years (median 11 years). In children aged 7–9, 10–12 and 13–15 years, the response rates were 69.4, 79.9 and 72.9%, respectively. The response rate for the various districts of the city ranged from 68 to 84%.
The proportion of missing values (‘not replying’ or ‘do not know’) for each of the single items ranged from 1.8 to 7.3% (median 2.1%) in the headache sample. The item concerning ‘number of earlier headache episodes’ had the highest number of missing answers (7.3%, n = 57). For ‘duration of headache’, answers were missing from 24 children (3.9%), and for ‘nausea’ the number of missing values was the lowest (1.8%, n = 11).
Prevalence of headache
The 1-year prevalence of headache not caused by infection or other illness, was 44.8% (n = 614) and the proportion of children who ever had experienced headache (lifetime prevalence) was only slightly higher at 45.4% (n = 622). A total of 16.0% (n = 219) had not experienced any kind of headache during the last year. Headache during the last year was significantly more common in girls (50.3%) than in boys (39.3%) (P < 0.001) (Table 2). However, no significant gender differences in prevalence rates were found under the age of 11 years, whereupon the prevalence increased further in girls (Fig. 1).

One-year prevalence of headache among 7–15 year-old Swedish schoolchildren, □, girls; ♦, boys.
One-year prevalence of different headache diagnoses in relation to gender

TTH – strict IHS, tension-type headache as defined by the IHS criteria.
TTH – modified IHS, tension-type headache as defined by the IHS criteria with criteria A and B excluded.
IHS 2.3, tension-type like headache not fulfilling the criteria.
CTTH, chronic tension-type headache.
Migraine – strict IHS, migraine as defined by the IHS criteria.
Migraine – modified IHS, migraine as defined by the IHS criteria with criteria A and B excluded.
IHS 1.7, migrainous disorders.
Migraine – Vahlquist, migraine as defined by the Vahlquist criteria.
∗P < 0.05
∗∗P < 0.001.
Prevalence of tension-type headache
With strict application of the IHS criteria, the 1-year prevalence of TTH was 9.8%. When excluding the headache duration (criterion B), the prevalence rate increased to 13.5%. Excluding both the criteria A and B (modified IHS criteria) resulted in a prevalence of 23.0% (Fig. 2). IHS 2.3 occurred in 9.5% of the children (Table 2).

Prevalence of tension-type headache and migraine with strict IHS criteria, with criterion B excluded or with both criteria A and B excluded. Note that criteron A defines number of earlier episodes and criterion B defines duration of headache. □, Strict IHS criteria; □, criterion B excluded; ▪, criteria A and B excluded.
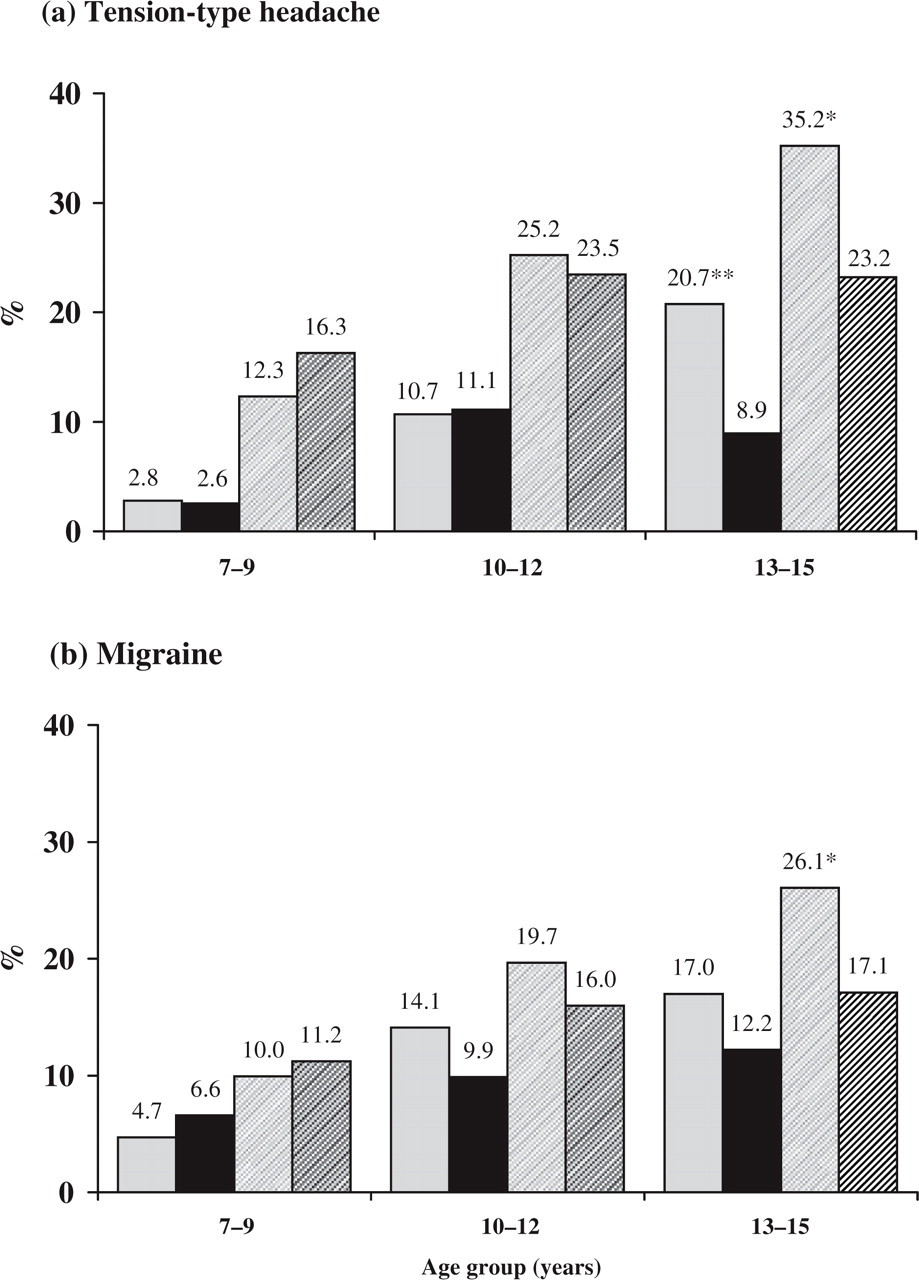
With strict IHS criteria, the prevalence rate of TTH was significantly higher in girls than in boys (Table 2). The prevalence rate increased with age, more so in girls than in boys (Fig. 3a). In children aged 7–9 and 10–12 years, the difference between girls and boys in prevalence of TTH was not significant. At the age of 12 the prevalence was 14.8% with strict IHS criteria, 15.7% in girls and 14.0% in boys – an insignificant difference. In children aged 13–15 years, significantly more girls than boys suffered from TTH. Similar age- and gender differences were seen for TTH with modified IHS criteria (Fig. 3a).
The prevalence of tension-type headache (a) and migraine (b) with strict or modified IHS criteria (criteria A and B excluded) by age group and gender. ∗P < 0.05; ∗∗P < 0.001. ▪, Girls strict; ▪, boys strict;, girls modified; boys modified.
Prevalence of migraine
The 1-year prevalence of migraine with or without aura was found to be 11.0% with strict IHS criteria and increased to 15.6% when criterion B was excluded. Excluding both criteria A and B resulted in a prevalence of 17.0% (Fig. 2). The prevalence of IHS 1.7 was 6.6% (Table 2).
With strict IHS criteria, the prevalence of migraine was slightly, but not significantly, higher in girls than in boys (Table 2). As for TTH, the prevalence of migraine increased with age and this was more so in girls than in boys (Fig. 3b). In children aged 7–12 years, no significant difference in migraine prevalence between boys and girls was found. At the age of 12, the prevalence was 13.2% with strict IHS criteria, 16.9% in girls and 9.7% in boys (not significant). In the 13–15 years age group, the difference in prevalence rates between girls and boys was insignificant for migraine with strict IHS criteria, but the difference was significant for migraine with modified IHS criteria (Fig. 3b).
Migraine with aura, visual or sensory, occurred in 7.8% of the children, slightly more often in girls than in boys (Table 2). Reports of aura increased significantly with age and was reported by 11 children (2.7%) aged 7–9 years, 37 children (7.8%) aged 10–12 years, and 59 children (12.1%) aged 13–15 years (P < 0.001).
According to the criteria of Vahlquist (11) the overall prevalence of migraine was 6.6% and higher in girls than in boys (Table 2). This prevalence rate of migraine was significantly higher than the one reported by Bille (3.9%) (P < 0.001). The prevalence rates in children aged 7 and 15 years were 3.0 and 7.7%, respectively, as compared with 1.4 and 5.3% in the study by Bille.
Number of earlier headache episodes
In the headache sample, 30.4% reported less than 10 earlier headache episodes and 12.9% less than five. The number of earlier episodes was significantly associated with age group (P < 0.001). The highest proportion of children who had experienced less than 10 earlier episodes was reported among the youngest children (Table 3), however, no significant difference in the number of earlier headache episodes was found in relation to gender (Table 3).
Number of earlier headache episodes, duration and frequency of headache by age group and gender

∗P < 0.05.
In order to study the number of earlier episodes and headache duration in relation to headache diagnosis, we used modified IHS criteria with the criteria A and B excluded. This was because the inclusion of criteria A and B defines the minimum number of headache episodes and the minimum duration for migraine and TTH, respectively. A significantly higher proportion of the children with TTH (36.5%) than those with migraine (22.2%) reported less than 10 earlier episodes (P < 0.001). However, in the 13–15 years age group, slightly more children with migraine (25.7%) than with TTH (20.8%) reported less than 10 earlier episodes, an insignificant difference.
Headache duration
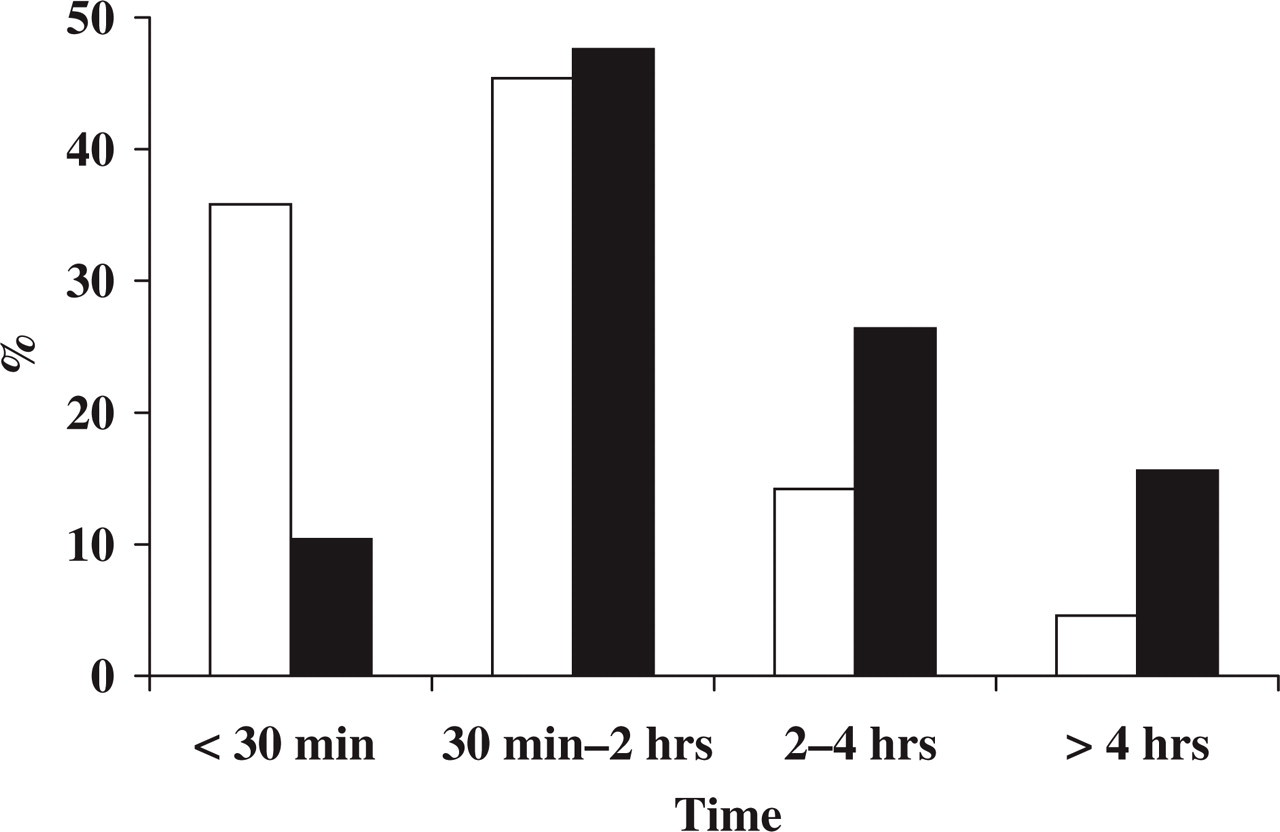
A total of 70.5% of the children with headache reported a duration shorter than 2 h and 25.1% reported a duration shorter than 30 min. There were no significant associations between headache duration, age and gender (Table 3). However, children with migraine reported longer headache duration than those with TTH (modified IHS criteria) (P < 0.001) (Fig. 4).
Duration of tension-type headache (TTH) (□) and migraine (▪) (modified IHS criteria).
Headache frequency
Among the children with headache, 24.4% reported headache occurring at least once a week. The proportions of children who reported frequent headache (at least once a week) increased with age (Table 3). Significantly more girls (27.6%) than boys (20.3%) with headache reported weekly occurrence (P < 0.05). The gender difference was most pronounced in children aged 13–15 years (Table 3). More children with migraine (39.4%) than TTH (20.8%) reported weekly headache (P < 0.05). However, when controlling for age and gender, the differences between these two diagnoses were only significant in the 13–15 years age group for both genders, and in the 10–12 years age group for girls. The proportion of children who reported suffering from more than one headache type was higher in migraine (49.0%) than in TTH (27.7%). When only those children who reported one headache type were included in the analysis, weekly headache was still more common in migraine (35.3%) than in TTH (17.2%) (P < 0.05).
Of the total sample, 39 children (2.8%) reported a headache frequency of more than 15 days per month, and out of them 20 children (1.5% of the total sample), 10 boys and 10 girls, during more than 6 months. However, only two children fulfilled the criteria for CTTH, corresponding to a prevalence rate of 0.1% (Table 2).
Discussion
In this population-based study of 1371 schoolchildren aged 7–15 years, the prevalence of headache was found to increase with age, especially in girls. In TTH as well as in migraine, the female preponderance was most pronounced in the 13–15 year age group. In addition, girls reported more frequent headache than boys, especially in the oldest age group.
Few reports exist on the prevalence of TTH during childhood and adolescence and the results from these earlier reports vary considerably (4–8). These variations in prevalence rates may partly be due to differences in study populations and assessment methods employed, but probably also because the IHS criteria were applied differently. In the study by Anttila et al. (6) on 12-year-old children, the prevalence of TTH was 12.2% according to the IHS criteria. At that age, the prevalence rates were similar among boys and girls. Similarly, in our study the prevalence rate of TTH was 14.8% and only slightly higher in girls than in boys at the age of 12.
In contrast, using the IHS criteria except for criteria A and B, Pothmann et al. (4), reported a higher prevalence rate of TTH (48.5%) than in our study (23.0%) and, unlike our results, a preponderance for boys. It should be noted that in both the studies by Anttila et al. and Pothmann et al. the estimates of TTH prevalence were based only on questionnaires.
Using interviews, Barea et al. (5) found a higher prevalence of TTH in girls than in boys and an increase with age, which is in accordance with our results. However, in their study, the total prevalence of TTH was strikingly higher (72.8%). It is noteworthy that almost all of the children with headache were classified as either having migraine or TTH and only one child (0.2%) was unclassifiable. When interviewing girls only, Ayatollahi et al. (7) reported a TTH prevalence of 12.1% and an increase with age. In a study of 5562 schoolchildren, who were all interviewed by the same neurologist, Özge et al. (8) found a TTH prevalence of 24.7%, however, relationships to age and gender were not studied.
In adults, TTH is more prevalent among women than men (26), which concurs with the finding of increasing prevalence in girls in the present study. The influence of sex hormones in TTH has been discussed but, so far, insufficiently investigated (27).
Although headache for at least 15 days per month during at least 6 months was reported by 1.5% of the children in the present study, only two children (0.1%) fulfilled the criteria for CTTH. A similar figure (0.9%) was reported by Abu-Arafeh et al. (9). In their study of 12-year-old children, Anttila et al. (6) found no child with CTTH, though, in accordance to our results, 1.6% reported headache for at least 15 days per month during at least 6 months.
In our study, the general frequency of headache was higher in girls than in boys and increased with age, findings consistent with outcomes from the cross-national WHO study (2). Unexpectedly, in both the study by Anttila et al. (6) and the present study, the reported frequency of headache was higher in children with migraine than among those with TTH. In our sample, the difference was most pronounced in the oldest age group. A higher frequency of headache in children with migraine might depend on co-existing tension-type headache. However, when only including those who reported one headache type, the frequency of headache was still higher in children with migraine.
For migraine, we found a 1-year prevalence of 11.0% with strict IHS criteria, a figure in accordance with estimates reported in earlier population-based studies in schoolchildren, varying between 2.7 and 13.7% (5, 7, 9, 12–14).
In this sample of schoolchildren, the use of strict or modified IHS criteria had great influence on the prevalence figures, especially for TTH, which increased from 9.8 to 23.0% when excluding criteria A and B, defining number of earlier episodes and duration of headache. In an earlier report, we showed that excluding criterion B resulted in an increased agreement between questionnaires and interviews for headache diagnoses, and a decreased number of unclassified headaches (24).
In the questionnaire, a considerable proportion of the children with headache (30.4%) reported less than 10 earlier headache episodes, especially in the younger age group. This may be due to the incidence of migraine (studies on TTH are lacking) being highest during childhood and adolescence (28,29). Consequently a number of children in the general population will only have had few previous headache episodes.
Further, a high proportion of the children with headache (70.5%) reported a duration of less than 2 h. Also, in previous clinical and population-based studies, a considerable proportion of children reported a headache duration shorter than 2 h (10, 12, 17–20). Only in one study, including children with severe, recurrent headache referred to a headache clinic, did all children with migraine or probable migraine fulfil the minimum duration criterion of 2 hours (30). Children were also asked to report the longest headache duration, including the time of sleep after an attack.
In clinical samples, due to inclusion of children with more severe headache, you would expect the criteria for duration of headache as well as the minimum number of earlier episodes to be more easily fulfilled than among children from the general population.
Another important aspect is that children under the age of 12 have difficulties with time estimation (31), and the parents’ observations may be restricted to the worst part of the headache attack. Thus, children and their parents may be unable to recall the real headache duration. The number of earlier headache episodes may also be difficult to estimate. The findings in our study of higher number of missing answers for the questions on number of earlier episodes and duration of headache suggest that these issues are problematic to assess for children and their parents.
To diminish classification problems that may contribute to a high number of unclassified headache, we suggest that the IHS criteria A and B should be modified or excluded, in particular in epidemiological research. For example, the minimum number of earlier episodes in criterion A should be reduced and, instead of using precise time limits in criterion B, a distinction should be made between very short headache (seconds to minutes) and headache with longer duration. However, further studies are needed to evaluate the specificity and sensitivity of such modified IHS criteria.
One of the aims of this study was to compare the results with the large study by Bille performed in the same Swedish city more than 40 years ago (10). Using the same criteria as proposed by Vahlquist (11), we found a higher migraine prevalence (6.6%) than in the study by Bille (3.9%). As we excluded all headaches associated with infection, fever or other disease, it is not possible to compare directly the prevalence rate of overall headache in our study (45.4%) with the one reported by Bille (58.7%). However, the number of children who reported no headache at all during the last year was higher in 1955 (41.4%) than in 1997 (16.0%), indicating an overall increase in headache prevalence among today's schoolchildren. This finding is in accordance with results from other studies in children and adolescents (1, 2). In contrast, no increasing trend was found in a large American population-based study on individuals older than 12 years of age, compared with a similar study conducted 10 years earlier (32).
In conclusion, in this sample of schoolchildren, the prevalence of TTH as well as migraine increased with age, especially in girls. The increase in prevalence in girls from the age of 12 was even more pronounced for TTH than for migraine. More studies of the prevalence of TTH and its relationship to puberty, menstruation and levels of sex hormones are needed.
The exclusion of the IHS criteria A and B led to considerably higher prevalence rates, especially for TTH. In epidemiological studies of TTH and migraine in children, the IHS criteria A and B seem less suitable. Further studies are needed to evaluate the specificity and sensitivity of modified criteria.
The proportion of schoolchildren in the city of Uppsala who never suffered from headache was lower in 1997 than in 1955, indicating an increase in the general prevalence of headache. The reason for this increase is unclear. Changes in society, increased stress and reduced physical activity have been suggested as causal factors, though evidence is still lacking. Future research should therefore address these important issues.
Footnotes
Acknowledgements
The authors would like to express their deep gratitude to the late Bo Bille, who initiated this work. The study was supported by grants from Uppsala County Council, Uppsala University and Swedish Migraine Society.