
Abstract
Complementary and alternative medicine (CAM) is increasingly common in the treatment of primary headache disorders despite lack of evidence for efficacy in most modalities. A systematic questionnaire-based survey of CAM therapy was conducted in 432 patients who attended seven tertiary headache out-patient clinics in Germany and Austria. Use of CAM was reported by the majority (81.7%) of patients. Most frequently used CAM treatments were acupuncture (58.3%), massage (46.1%) and relaxation techniques (42.4%). Use was motivated by ‘to leave nothing undone’ (63.7%) and ‘to be active against the disease’ (55.6%). Compared with non-users, CAM users were of higher age, showed a longer duration of disease, a higher percentage of chronification, less intensity of headache, were more satisfied with conventional prophylaxis and showed greater willingness to gather information about headaches. There were no differences with respect to gender, headache diagnoses, headache-specific disability, education, income, religious attitudes or satisfaction with conventional attack therapy. A higher number of headache days, longer duration of headache treatment, higher personal costs, and use of CAM for other diseases predicted a higher number of used CAM treatments. This study confirms that CAM is widely used among primary headache patients, mostly in combination with standard care.
Introduction
Standard prophylactic medical treatments such as β-blockers, anticonvulsants or antidepressants are well established in primary headache disorders. There is also evidence for the effectiveness of some non-pharmacological therapies such as cognitive behavioural therapy, progressive muscle relaxation and biofeedback. However, the use of other often-recommended pharmacological and non-medical treatments is either not investigated or has failed to prove efficacy. Successful drug-based prophylactic treatment is achievable in about two-thirds of patients suffering from migraine, but side-effects of pharmacological treatment often limit the use of these drugs. Furthermore, patients often avoid regular intake of drugs for prophylactic treatment of headaches. Therefore, patients are very attentive to complementary and alternative medicine (CAM) strategies in the prophylaxis and treatment of headache attacks. CAM practitioners emphasize the holistic, individualistic, empowering and educational nature of CAM (1). In US population-based studies from 1990 to 1997, the general use of CAM therapies increased from 33.8 to 42.1% (2) and in Germany there was an increase of CAM use from 52% in 1970 to 65% in 1997 in the population (3). However, the use of CAM is increasing not only in the general population but also in neurological patients (4). There is no generally accepted definition of CAM, which contrasts with the growing number of publications about CAM (5). Therefore, definitions to differentiate those therapies that are considered to be CAM, especially in headache therapy, do not exist. In general, it may depend on the kind of disease and the medical concepts of patients and therapists which different therapeutic strategies are subsumed under the term CAM. The (US) National Center for Complementary and Alternative Medicine defines CAM as ‘a group of diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine’ (6). Lundberg and Fontarnarosa stated ‘there is no alternative medicine. There is only scientifically proven, evidence-based medicine supported by solid data or unproven medicine, for which scientific evidence is lacking’ (7). This means that patients' and therapists' views on the efficacy of CAM are the most crucial question. However, which methods belong to CAM is still under discussion, depending from the kind of disease, cultural background, and health system conditions. Some of these in the field of headache therapies have been proven in clinical trials (e.g. Petasites hybridus) (8), others are only based on traditional theories and clinical experience (e.g. acupuncture) but have not shown consistent efficacy in randomized controlled clinical trials (9, 10). However, the majority of CAM therapies still remain to be evaluated in controlled prospective clinical trials.
In general, CAM therapies are not provided by regular physicians but can be prescribed, recommended or performed by a CAM practitioner, a physiotherapist, or sold over the counter (OTC) without a prescription (e.g. mineral or vitamin substitution). Patients' beliefs about the effectiveness of any therapy are important in the field of CAM, more so even than randomized controlled trials. Data about motivation of CAM use and incidence of CAM use among headache patients in Germany are scant, hence the reason for this study.
Methods
Study population
Between July 2005 and December 2006, 470 patients with primary headache disorders were consecutively invited to participate; 448 were recruited in seven tertiary headache centres in university hospitals in Germany and Austria. Inclusion criteria were: diagnosis of a primary headache [e.g. migraine, tension-type headache (TTH), trigemino-autonomic headaches] according to the criteria of the International Headache Society (IHS) [International Classification of Headache Disorders, 2nd edn (ICHD-II)] (11). ICHD-II diagnosis was ascertained by experienced neurologists in all participants. Finally, 432 of the 448 (96.4%) patients were included in the analysis [Halle (n = 100), Hamburg (n = 100), Regensburg (n = 69), Ulm (n = 28), Münster (n = 53), Wien (n = 56) and Innsbruck (n = 26)]. Sixteen patients were excluded because of insufficient language knowledge, refusing participation at a later time, failure to send back the questionnaire, or a high amount of missing data. Patients suffering from medication overuse headache (MOH) were not included due to the classification of MOH as a secondary headache in ICHD-II and the difficulties in identifying the underlying primary headache in a cross-sectional study. The study was approved by the local ethics committee. Written informed consent was obtained of all patients. There was no financial funding of this study.
Research instruments
The questionnaire consisted of 42 items, including sociodemographic information, headache-specific data (e.g. onset and history of disease, frequency of attacks, conventional therapies, actual medication and prophylaxis, comorbid diseases, regular treatment). The seven-paged survey was developed by the Department of Neurology, University of Halle. The time for completing the questionnaire should not take > 30 min. Socioeconomic data were obtained following Jöckel et al. (12). Additionally, a standardized questionnaire about headache-specific disability in daily life [Migraine Disability Assessment Score (MIDAS)] was implemented (13). We included a list of possible CAM treatments in headaches. Patients could add additional therapies at the end of the list. Patients were asked for their lifetime experience with CAM use for headache therapy and duration of CAM use.
Statistics
Comparisons were primarily carried out between patients who had used CAM treatments and those who had not. Frequency distributions (e.g. gender, headache diagnoses, religious attitudes and willingness to gather information about the disease) between CAM users and non-users were analysed by χ2 test. Quantitative data were compared by Student's t-test or Mann–Whitney U-test. Alpha level of significance was set at 5%, two-tailed. Further explorative computations used a linear regression model to evaluate predictors for the number of used CAM treatments. Therefore, in the CAM user subgroup variables significantly correlating (Spearman rank order correlation) with the number of used CAM treatments were included in the regression analysis. All computations were made using
Results
Headache diagnosis and characteristics of the study population
The majority of participants were female (75.5%). The age range of the whole sample was 13–83 years (median 40.13;
Mean duration of disease was 16.28 years (
In the major diagnosis groups with statistically and clinically relevant sample sizes (migraine and TTH, but not a combination of both), chronic forms were identified according to the ICHD-II criteria. For statistical reasons we pooled the diagnosis ‘infrequent episodic tension type headache’ (ICHD-II 2.1) and ‘frequent episodic tension type headache’ (ICHD-II 2.2) into one group and separated this from the chronic variant (ICHD-II 2.3). Thirty-five (11.5%) patients with solitary migraine suffered from chronic migraine. According to the criteria of ICHD-II, 25 (50%) solitary TTH patients showed chronic courses of the disease.
There were no significant differences between the study centres with respect to frequency of headache diagnoses. Two hundred and fifty-four (58.8%) of the participants had a positive family history of headache, and 189 (43.8%) suffered from at least one additional disease.
Three hundred and ninety-seven (91.9%) of the participants were under regular attack treatment using analgesics or triptans, and 160 (37%) used a regular pharmacological prophylactic therapy. Satisfaction with the attack treatment was 25.9% ‘very pleased’, 39.0% ‘moderately pleased’ and 23.9% ‘dissatisfied’; 11.1% gave no information. As regards prophylactic therapy, 28.8% were ‘very pleased’, 35.6% ‘moderately pleased’ and 28.1% ‘dissatisfied’, whereas 7.5% of the patients gave no information.
Headache-specific disability according to MIDAS was moderate to severe in 321 (74.3%) participants, whereas only 54 (12.5%) were low to not affected in daily life; 57 (13.2%) patients gave no information.
CAM use in the study population
Three hundred and fifty-three (81.7%) participants used at least one of the therapies classified as CAM. Forty-one of them were not aware of having used alternative therapies, but affirmed using CAM treatments in the given list. Most (71.1%) patients used CAM in addition to their conventional treatments. The mean duration of CAM use was 7.2 years (median 4;
Frequencies of used CAM treatments

∗In Germany ‘Manual therapy’ usually means treatment by specialized physiotherapists with soft treatment methods and not adjustments. CAM, complementary and alternative medicine.
Motivations for using CAM treatments were ‘to leave nothing undone’ (63.7%), ‘to be active against the disease’ (55.6%), ‘not to take a permanent medication’ (40.2%), ‘advice of another person’ (39.1%), ‘dissatisfaction with conventional treatment’ (34.0%), ‘request for a therapy without side effects’ (31.2%), ‘anxiety of side effects’ (20.1%), ‘bad experience with regular treatments’ (8.8%) and other (7.6%).
Reasons for not having used CAM were ‘not heard about it’ (27.8%), ‘too expensive’ (12.7%), ‘I do not believe in this’ (8.9%), ‘no interest’ (3.8%), ‘other reasons’ (25.3%); 21.5% of non-users gave no information.
Characteristics of CAM users vs. CAM non-users
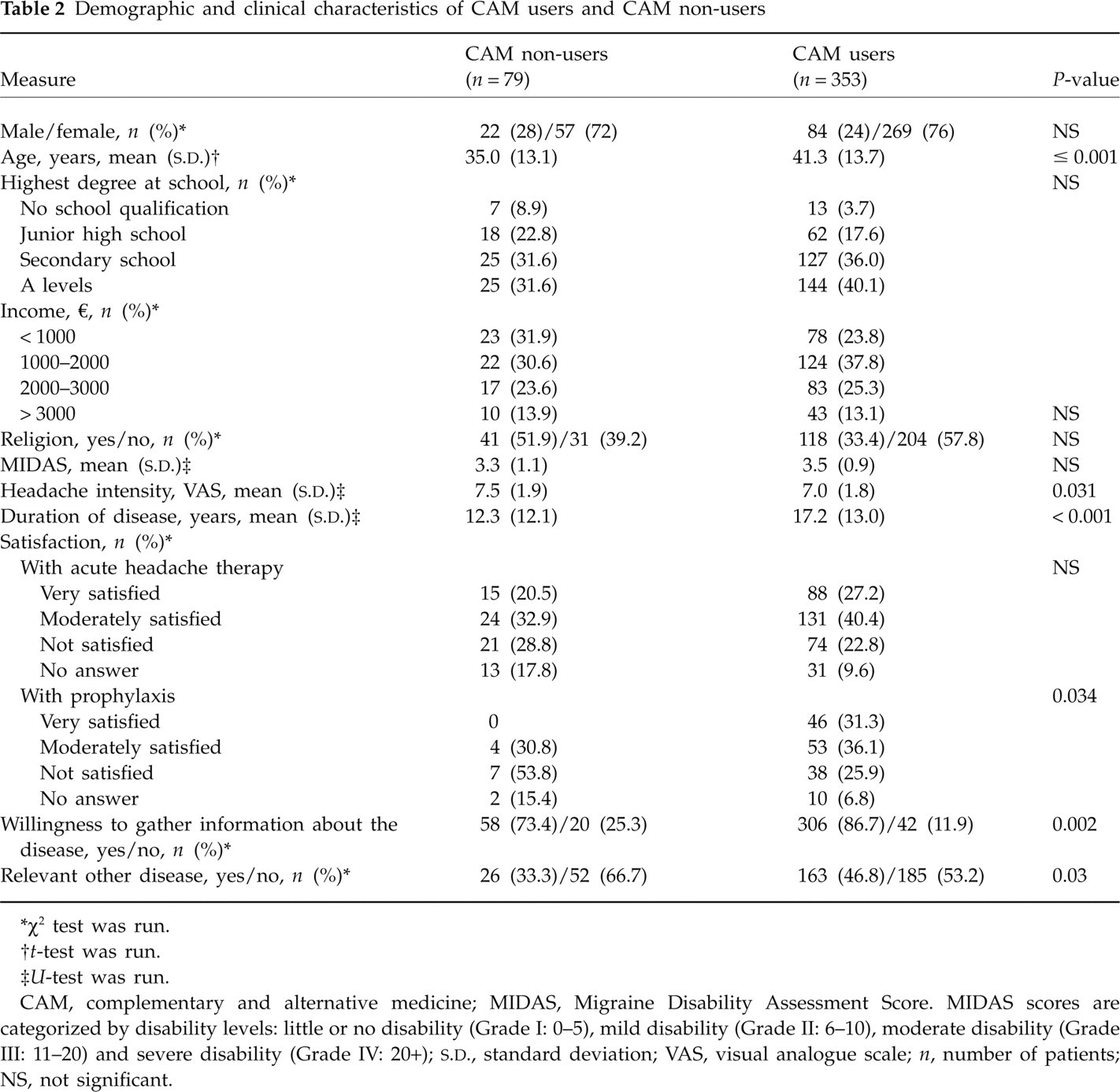
Compared with non-users, CAM users showed greater age, longer duration of disease (independent of greater age as controlled by analysis of covariance), less headache intensity, more satisfaction with conventional pharmacological prophylaxis, and more willingness to gather information about their disease. The two groups did not differ significantly in their patterns of gender, headache diagnoses, headache specific disability, education, income, religious attitudes or satisfaction with conventional attack therapy (Table 2). Furthermore, comorbidity in CAM users was higher than among non-users (unfortunately, comorbidities were not further specified by most of the patients).
Demographic and clinical characteristics of CAM users and CAM non-users
∗χ2 test was run.
† t-test was run.
‡ U-test was run.
CAM, complementary and alternative medicine; MIDAS, Migraine Disability Assessment Score. MIDAS scores are categorized by disability levels: little or no disability (Grade I: 0–5), mild disability (Grade II: 6–10), moderate disability (Grade III: 11–20) and severe disability (Grade IV: 20+);
A linear regression model was carried out to reveal predictor variables of the number of used CAM treatments with high significance (F = 5.58, d.f. = 14, P ≤ 0.001), but it explained only 37.7% of the variance of the criterion, suggesting more complex conditions than detectable with the available variables. Given significant Spearman rank order correlations with the criterion included, potential predictive parameters were age, variables according duration and pattern of disease and treatment, the presence of a comorbid disease, MIDAS score, expense of costs of CAM and prior experience with CAM. Regression analysis revealed a higher number of headache days, longer duration of headache treatment, higher personal costs and prior use of CAM for other diseases as predictors for a higher number of used CAM treatments (Table 3).
Predictors for the number of used CAM treatments (significant correlation with the criterion) in a linear regression model

CAM, complementary and alternative medicine; MIDAS, Migraine Disability Assessment Score; NS, not significant.
Characteristics of patients with chronic vs. episodic headache
Comparisons between chronic and non-chronic courses of headache were performed only for patients with solitary migraine or TTH due to sufficient sample sizes. For clear presentation and statistical reasons, patients with chronic TTH and chronic migraine were summarized in one group and compared with the group of patients with episodic TTH and episodic migraine. To reveal diagnosis-specific and chronification-specific effects, accordant explorative subgroup analyses were carried out (chronic migraine vs. chronic TTH; episodic migraine vs. episodic TTH; chronic vs. episodic migraine; chronic vs. episodic TTH). In both groups the majority of patients were female, but the chronic group included proportionally more male patients than the episodic headache group. Unexpectedly, in our sample patients with chronic headache had shorter durations of disease compared with patients with episodic headache (Table 4). Whereas a longer duration of disease was associated with using of CAM in the whole sample (Table 2), the chronic group was more likely to use CAM even though having fewer headache years. Therefore, we suggest chronification as an additional predictor for CAM use. Furthermore, the chronic group reported greater headache-specific disability and less satisfaction with conventional attack therapy and prophylaxis. No differences where found in age, headache intensity or the willingness to gather information about the disease (Table 4). The patterns of motives for using CAM treatments did not differentiate between CAM users in the two groups, either. Exploratively comparing diagnosis-specific and chronification-specific subgroups where statistically appropriate, use of CAM and dissatisfaction with conventional treatment were associated with chronification, too. Diagnosis-specific differences were a higher proportion of women and a longer duration of disease in migraine patients compared with TTH patients in general.
Characteristics of patients with chronic and episodic headache

∗χ2 test was run.
† t-test was run.
‡ U-test was run.
CAM, complementary and alternative medicine; MIDAS, Migraine Disability Assessment Score. MIDAS scores are categorized by disability levels: little or no disability (Grade I: 0–5), mild disability (Grade II: 6–10), moderate disability (Grade III: 11–20) and severe disability (Grade IV: 20+);
Discussion
The increasing trend of CAM use has been noted in clinical practice as well as in surveys in the USA (2) and Germany (3). This study has provided information about the use of CAM among headache patients. As well as in other diseases, many patients suffering from primary headache disorders are interested in CAM instead of or in addition to conventional drug treatment in acute headaches and in prophylaxis also. It has to be considered that our survey was performed among patients treated in tertiary out-patient headache centres. This population is representative neither of all headache patients nor of the general population. Patients affected only mildly are more likely to treat themselves with OTC medication or they are under the care of general practitioners. In the present study, most patients suffered from migraine (78.5%). This may not represent headache prevalence in the population (most research shows a predominance of TTH), but reflects in our experience diagnosis frequencies in a tertiary out-patient clinic. The majority of patients with TTH utilize self-medication or are treated by the family physician, and often only chronic or therapy-resistant courses frequent a neurologist or an out-patient headache clinic. Patients in tertiary care might be more affected by their disease than the general headache population. However, the study has a number of strengths including a large country-wide sample size with a high participation rate, so the data may be representative of a higher affected headache population that is treated in special centres. The study of von Peter et al. included primary and secondary headache disorders in the USA, but the sample consisted of only 73 patients (14). A retrospective single-centre study performed some years previously showed a response rate only in 29% and complete data in 16% of participants (15). The majority of our participants (74.3%) showed moderate to severe headache-specific disability in daily life, which corresponds to prior Italian headache studies about CAM and patients from tertiary out-patient clinics (16, 17). Therefore, our results confirm that most patients who are considerably impaired in their quality of life are treated in tertiary centres. It is suggested that data of primary and secondary treated headache patients can be used for comparison with the presented results.
Patients focusing on primary or exclusive CAM treatment of their headaches may be underrepresented in this university hospital-based collective. In general, patients look for therapies with the potential to improve their quality of life or showing fewer side-effects. As regards the prevalence of CAM use, it has to be considered that in contrast to this, CAM was more often used in order to prevent illness or to strengthen the immune system, rather than treatment of illness (18–20). Often patients are not aware of the potential risks of CAM treatment. CAM or herbal remedies are considered as ‘natural’ and safe, but some have potentially harmful side-effects. The use of CAM is frequently not communicated to the doctor (25.5% in our survey), which is consistent with the literature. Likewise, the doctors often do not ask for additional CAM therapies, neglecting the treatment preferences of the patients (21, 22). Patients often do not know that CAM therapies are not strictly regulated by the administrations (Food and Drug Administration for the USA, Bundesinstitut für Arzneimittel und Medizinprodukte for Germany), and many of the offered substances are classified as dietary supplements and not as drugs (23). This does not imply per se safety of the products.
Comparison of available data about CAM use among headache patients in different countries is shown in Table 5. This revealed higher use of CAM in the US and German population and preference for acupuncture in Germany compared with the others. Data interpretation is limited for several reasons: it has to be considered that different definitions of which therapies belong to CAM are used in the studies, resulting in different rates of CAM use. For example, the US survey includes biofeedback, which was excluded in other studies, because is not unconventional and efficacy is proven in trials. Furthermore, the designs of the trials are different: data of the US survey were taken by personal or telephone interview, whereas our study was based on a standardized questionnaire (14).

CAM, complementary and alternative medicine; TTH, tension-type headache.
With regard to socioeconomic and epidemiological data, the findings are different in several studies. Some showed female preponderance in CAM use (2, 25), others, like ours, failed to show such a gender effect (26). Data about age-related use of CAM are conflicting: positive correlation was detected in some studies, whereas others did not find such an effect (27, 28). A non-headache-specific survey in the USA found those reporting practitioner-assisted CAM therapy were more likely to be female, single or divorced, White, with some college education, reporting four or more health problems and with good general health (29). We found a correlation between higher age and longer course of disease, which may reflect the higher burden of disease in long-term course of illness. Obviously patients of higher age, longer duration of disease and those showing a greater willingness to gather information about headache and treatment methods are more likely to come into contact with CAM. Users of CAM therapies in the presented study furthermore had less headache intensity, were, in contrast, more satisfied with conventional prophylaxis and willing to report about their disease compared with non-users. Regarding less headache intensity of CAM users, it remains unclear if headache had a prior lower level or improved with CAM.
Additional comparisons of chronic and non-chronic headache patients suggest chronification as a predictor for increased CAM use. These may be explained by a higher headache-specific disability and less satisfaction with conventional attack therapy and prophylaxis, which leads to seeking alternatives in treatment.
Additional factors, such as the personal course of disease or individually different perception and understanding of pain, could also affect the subjective measure of headache intensity. Further investigation may reveal if a potential decrease in headache intensity is the effect of CAM use or if less affected patients are more likely to try CAM. Most patients of the study population are under regular treatment. This causes a selection bias in the study because none of the headache clinics provides exclusively CAM treatment. Theses are also approaches for prospective investigations. Higher income was reported in prior studies to be associated with increased CAM use, which was not a significant predictor in our study (2, 26, 28, 30, 31). These differences may in part be caused by different definitions of what CAM is and by regional differences in income and health system, especially the willingness of health insurance to reimburse the costs for such treatments.
A substantial proportion of our study population were dissatisfied with the usefulness of their former medical treatment (22% dissatisfied with attack medication and 10.4% with prophylaxis). This may reflect the situation of conventional pharmacological treatment; part of the headache population does not respond to the standard treatment options either in acute or in prophylactic treatment. However, patients used CAM not because of general dissatisfaction with conventional therapy. Furthermore, most of them exploratively showed an active oriented coping and utilized alternative treatments in addition to conventional care. In the German healthcare system, the time for consultation is short, caused by economic necessity. In contrast, the time for consultation, for example, by homoeopaths was found to be more than twofold longer than consulting a physician practising conventional medicine, so patients receive more attention than in the usual consultation with a physician (32).
Use of CAM was reported by the majority (81.7%) of the study population. The most frequently used CAM treatments included acupuncture (58.3%), followed by massage (46.1%) and relaxation techniques (42.4%). The most common pharmacological CAM among the study population was homoeopathy (23.1), followed by high-dose megavitamins (7.4%) and herbal medicine (5.6%). This does not reflect the scientific evidence for these therapies (33). Patients may not choose a specific method because of intellectual discourse or individual preference, but choose methods easily available to them. The testimony of family members and friends (anecdotal evidence) plays an important additional role (34). The mean number of used CAM treatments during the course of the disease was 3.9, which was comparable to the 3.5 finding in a retrospective study on this topic (15). This may be explained by ineffectiveness of some therapies, which leads to testing other therapeutic offers following a trial and error concept. In the patients' view, scientific data on a CAM therapy of their choice is not the most crucial aspect, as they do not pay attention to evidence-based medicine. Of patients in a recent survey, 65% reported that they would continue their CAM therapies despite negative scientific reports; positive personal experience overrides scientific data (35).
There is a strong need for future adequate randomized trials about the effects of CAM, physical therapy and exercises in primary chronic headache disorders (36). The design of these trials should follow the recommendations of the IHS for controlled trials (37). Difficulties in randomized trials on CAM arise from difficulties with blinding of non-pharmacological therapies, lack of adequate placebo control and the strong patient preference for their therapy of choice, which results in refusing of randomization in trials (38). Additional research is also needed to determine the cost effectiveness of CAM therapies, which is still unknown (39).
Conclusion
CAM is in widespread use among patients in tertiary headache care. Clinicians treating headache patients may consider use of these therapies as adjunctive or alternative treatment. Considering patients' wishes about treatment, the physicians should ask patients about their experiences with CAM. Ignoring this is neglecting a chance of sometimes successful treatment options. Information about scientific evidence of CAM could add to the patients' anecdotal evidence for belief in CAM therapies. An integration of CAM contents in medical education is useful to inform patients adequately about possible effects, side-effects, contraindications and potential interactions of CAM with standard care therapies. This is of particular importance in the treatment of chronic headache patients, who often have a long-lasting history of medical therapy. Therefore, it is appropriate to take advantage of all available resources. Since almost 25% of the study population is dissatisfied with standard care, a single therapy concept often seems insufficient in these complex cases. Integration of alternative and complementary treatments in conventional care according to a multimodal therapy may be useful. Most evidence is available for the additional or alternative treatment with Petasites, Coenzyme Q10 and stress management strategies using relaxation techniques and biofeedback in the prophylaxis of primary headaches. However, the combination of methods has to be investigated in controlled clinical trials.