
Abstract
The objective was to determine headache patients' knowledge, prevalence of use and perceived effectiveness of complementary and alternative medicine. Seventy-three patients with headache syndromes attending a head and neck pain clinic were interviewed using a standardized questionnaire. Alternative medical therapies were used by 85% of surveyed patients for the relief of their head pain. In 60%, the therapies were perceived to have a benefit. Almost 100% of the patients were familiar with one or more of the presented alternative treatments. Eighty-eight per cent perceived at least one of the complementary treatments to be an effective remedy for headache pain. Exposure to and interest in alternative treatments are common among patients with headache syndromes, despite the lack of scientific evidence of benefit and assessments of risks for many of the treatments. Neurologists and general physicians should be aware of the increasing role of alternative medicine in the healthcare system. There is still an urgent need for objective, integrative and critical research with regard to complementary and alternative medicine.
Introduction
Headache is a common pain problem and one of the most frequent reasons for visits to general practitioners and neurologists. It is a major public health problem, which places a great strain on the quality of life of people of all ages and countries (1). Moreover, the management of headache disorders represents a drain on national health systems and results in significant socioeconomic costs (reduced or lost productivity, long-term disabilities) (1–3). Despite a wide range of current treatments for headache, many patients fail to achieve optimal control, or do so only at the expense of unacceptable side-effects. Recognizing the increasing interest in complementary and alternative medicine (CAM) among the public, this survey aims to assess headache patients' knowledge, prevalence of use and perceived effectiveness of CAM, as well as their expectations in relation to the use of CAM.
Materials and methods
The study population consisted of 73 patients attending the outpatient headache clinic at the Columbia campus of New York Presbyterian Hospital. Criteria for selection included a diagnosis of ‘headache’ as determined by the patient's primary physician or neurologist. Subjects were English-speaking patients over 18 years old, with no evidence of any cognitive or physical impairment that might prevent completion of the interview. Fifty-five patients had a face-to-face interview of approximately 5 to 10 min duration conducted by one of the authors. A trained research assistant interviewed 18 patients over the telephone.
Demographic data, including age, sex, marital status, education and ethnic background were recorded. A questionnaire was administered asking patients to describe their headache characteristics (frequency, intensity and duration), any associated symptoms (vomiting, bed rest required, dizziness, time spent out of work, disturbed sleep) and the number of years they had been suffering from headaches. A visual analogue scale (VAS) was used to describe the severity of headache. The patients' regular physicians were asked to classify the type of headache (migraine, tension, etc.) according to the current International Headache Society Classification scheme.
Complementary and alternative medicine was defined in this survey as ‘medical interventions, not taught widely at US medical schools or generally available at US hospitals’, a definition described by Eisenberg and associates (4). A list of 49 different CAM treatments and modalities with potential effects on pain was compiled (Table 1). The patients were given a list of different CAM treatments and were asked the following questions: (a) which methods were familiar to them as potential therapeutic interventions; (b) which methods they had tried; (c) what the results were; and (d) which of the listed treatments they thought might be beneficial for their disorder, and if so, why they had not tried this treatment so far.
Various techniques of CAM presented to the patients


∗Percentage of patients who had tried the treatment (
∗∗number of patients having perceived the treatment to be beneficial/
∗∗∗number of patients who did not have any benefit from the treatment).
†None of the patients had tried this treatment.
‡None of the patients was familiar with this therapy.
§Not used under this subgroup in the questionnaire.
For the statistical analysis, a chi-square test was used to compare the sociodemographic and clinical data with the pattern of responses. A P-value of less than 0.05 was used as the criterion for significance.
Results
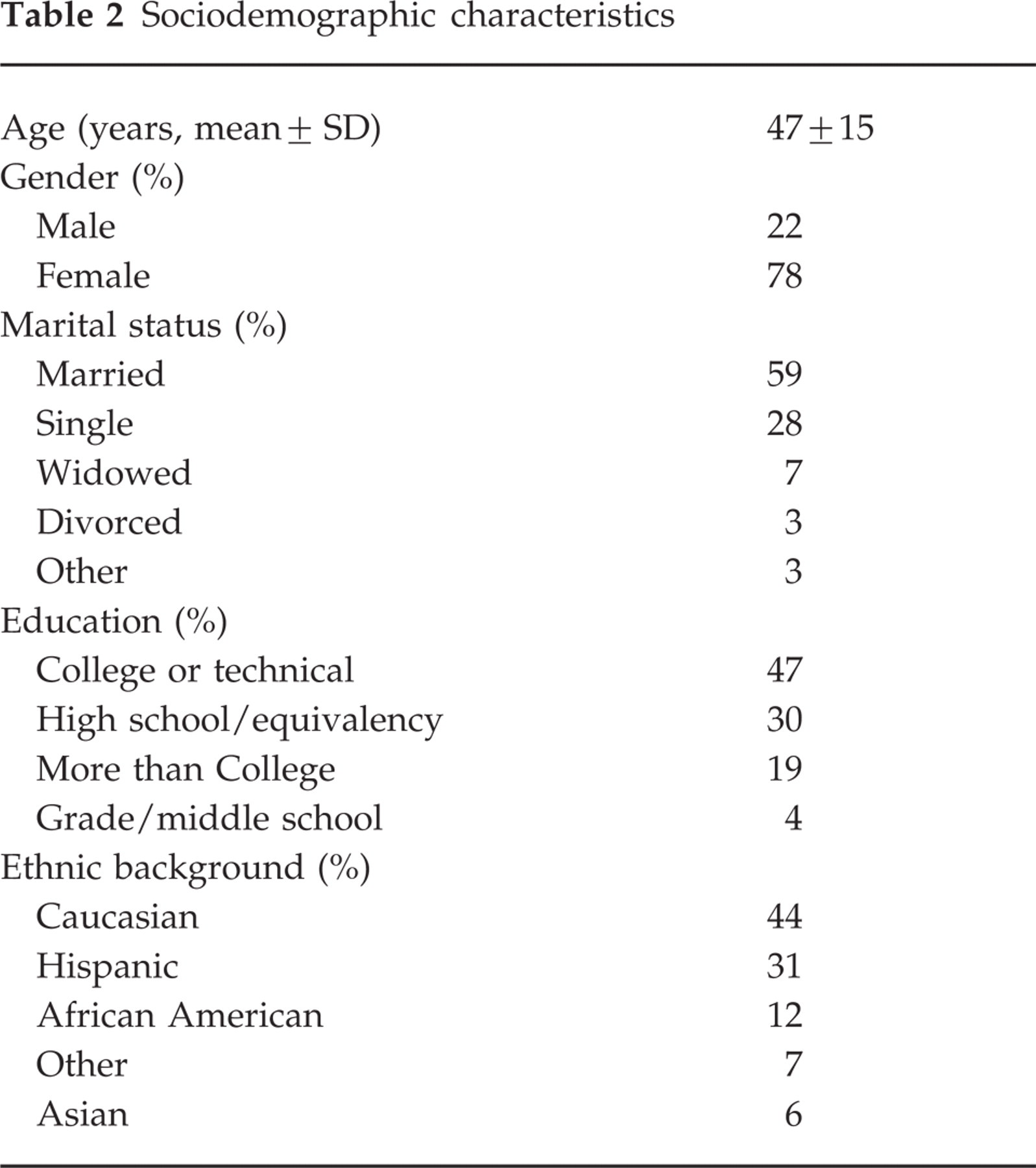
Tables 2 and 3 show sociodemographic and clinical characteristics of the patients. The majority of patients were female and most were married. Of the surveyed patients, 66% had completed schooling beyond high school; 44% of those interviewed were Caucasian, while 31% were Hispanic, 12% African-American and 13% described themselves as ‘other’ (6% were Asian and the remaining 7% were Native Americans, Pacific Islanders or not further specified). Migraine, myofascial pain and tension headache were the most frequently diagnosed types of headache. The mean intensity rating was 8 on a scale from 1 to 10 and in 37% of the patients the headache was specified as being constant or daily, indicating that the patients surveyed were considered to have severe headache disorders. Moreover, 79% of the patients took medication for their headaches, 38% had associated sleep disturbances and 23% were unable to work because of their head pain. A wide individual variation is shown with regard to mean duration of pain incidents and past years of suffering.
Sociodemographic characteristics
Clinical characteristics

Knowledge
Ninety-eight per cent of the interviewed patients were familiar with at least one presented CAM treatment as a therapeutic intervention, 44% of the patients were familiar with between one and 13 treatments, 41% were aware of 14–25 treatments, and 15% knew of more than 26 treatments. This and the mean knowledge of 7±9 treatments per patient indicate a wide individual difference and in total a broad knowledge of the listed CAM remedies and their therapeutic uses (Table 1). No statistical correlation was found when comparing individual education levels with knowledge of CAM modalities. CAM treatments familiar to the majority (86%) of patients included massage, acupuncture/acupressure, meditation, herbs, vitamins and nutritional supplements. About half of the patients were familiar with chiropractic, yoga, biofeedback, relaxation therapy, psychotherapy, homeopathy and aromatherapy. Less than 10% of the patients were familiar with Feldenkrais, craniosacral therapy, anthroposophic medicine and neural and reconstructive therapy.
Use
Eighty-four per cent of the patients had used one or more CAM treatments for the alleviation of headache, with a mean amount of 3±2 modalities used per patient. Of the 50 CAM therapies listed, 26 (52%) had been used by the patients in this sample. The percentage of use and the number of patients who perceived the treatments to be effective are shown in Table 1. The most frequently used CAM therapies were massage (42%), exercise (30%), acupuncture (19%), biofeedback (15%), chiropractic (15%), herbs (15%) and vitamins/nutritional supplements (14%). In about 60% of the patient population, the therapies used were perceived to have a benefit, as indicated in parentheses in Table 1. The perceived usefulness differed widely from treatment to treatment. The most useful therapies for alleviating head pain were acupuncture/acupressure, exercise, chiropractic manipulation, relaxation therapy, massage, biofeedback and herbs (Table 1).
Expectations
Eighty-eight per cent of the patients believed in at least one treatment as a potentially beneficial headache remedy. The highest percentage of patients believed in massage, acupuncture and meditation for the relief of headache pain (Table 1). Reasons listed for not having used these therapies were lack of referral/recommendation by personal physicians, lack of time, cost of the therapy and lack of insurance coverage for CAM therapies. In addition, patients reported lacking information about where to obtain these treatments or whether treatments would be useful. Some patients reported concerns about the possibility of treatments having adverse effects or potentially aggravating their conditions.
Analysis
No statistically significant differences were found among the surveyed patients in knowledge, use or expectations regarding the listed CAM treatments when compared with sociodemographic and clinical characteristics. However, given the small sample size, this outcome should be of minor value.
Discussion
This study demonstrates that a high proportion of headache patients use and frequently perceive a benefit from CAM therapies. Almost 85% of those interviewed had used at least one of the listed CAM treatments, and in 60% the therapies used were perceived to be beneficial. Moreover, a high percentage of patients were well informed about the existence of the treatments mentioned and wished to try some of them. Almost all of the patients were familiar with at least one of the remedies and 40% knew of up to 25 treatments as possible therapeutic interventions. Eighty-eight per cent of the patients thought that at least one of the modalities might be beneficial for their headache disorder.
These findings are consistent with several studies assessing the prevalence and patterns of CAM use. Interest in CAM among the public and medical community in the United States of America (USA), Europe and Australia has increased significantly over the past decade. In 1993 Eisenberg et al. reported that approximately one in three Americans had used at least one form of alternative therapy in the preceding 12 months (4). They estimated that visits to CAM providers (425 million) exceeded the number of visits to all USA primary care physicians (388 million) at the time of publication. The results of this study estimated the annual USA expenditure for CAM to be $13.7 billion dollars. In another national study, Paramore (5) found that 10% of the USA population (25 million people) saw a CAM professional in 1994 for at least one of the following four therapies: chiropractic, relaxation techniques, therapeutic massage and acupuncture. A follow-up study by Eisenberg in 1997 showed an upward trend in both the reported use of CAM (from 33.8% of the USA population in 1990 to 42.1% in 1997) and annual CAM expenditures ($14 billion in 1990; $22 billion in 1997) (6). In Australia, McLennan et al. reported that approximately 50% of those surveyed had used CAM in the previous year (7). The reported prevalence and costs of CAM in Europe vary depending on the country and the type of survey, but in general exceed those of Australia and the United States (8–10).
This pattern of increasing interest was analysed in several studies by looking at patients' motivations for using CAM. Some attribute this to conventional medicine's high costs, impersonality, bureaucracy, and the perceived over-specialization of allopathic medicine (11). Moreover, the efficacy of conventional treatments, especially with regard to chronic illnesses and non-specific symptoms, is frequently questioned and found unsatisfactory by many CAM users (12–15). Additionally, the side-effects of conventional treatments, both as perceived by patients and as widely reported by the media, may contribute to the interest in CAM modalities (14). Lastly, patients are attracted to CAM by holistic treatment philosophies, encouragement of self-help measures and lesser side-effects (11, 16).
The high prevalence of CAM use requires even more serious consideration in light of several studies reporting that most physicians are unaware of their patients' use of these therapies (4, 18). Indeed, 72% of CAM users reported not discussing such treatments with their doctors. There is still a lack of scientific evidence and risk assessment for many CAM treatments, in part due to problems in designing studies of CAM. It is argued that the methods and results of CAM are hardly testable by controlled trials (11, 14). Among other problems, placebo treatments are difficult to establish, therapies cannot be masked and are highly individualized, outcome variables are not reliable, and the rather ‘soft’ expected outcomes require many patients and long treatment periods (18). These problems make it difficult to systematically evaluate and report the effects of CAM, its side-effects, and interactions with conventional medicine treatments.
A few limiting factors were present in this study. There was an uneven gender distribution, which could be explained by the predominance of females seeking medical care for headaches (19). The small sample size, the inclusion of only English-speaking patients and the fact that only patients attending a headache clinic were included could have decreased the generalizability of the results. This may be particularly true regarding the perceived benefits of alternative treatments used, as this may have been confounded by the fact that most of the patients in this sample had been unresponsive to prior conventional therapies. Finally, the internal and external validity of the questionnaire was not determined.
Nevertheless, these findings suggest that several modest recommendations should be made. Physicians should be made aware of the increasing interest in and use of CAM by headache patients. Moreover, physicians should be aware of the fact that most patients do not report the use of CAM to their doctors. Openness to potentially beneficial treatments should be an important aim in the physician–patient relationship and inquiries about the use of CAM should be part of the routine medical history. Moreover, incorporation of CAM remedies that are considered safe and effective into daily pain practice is a desirable future direction. The relationship between CAM and conventional therapies is often mischaracterized as an either-or relationship, implying CAM use instead of conventional treatments. In contrast, CAM may permit synergistic collaboration (20), as verbalized by Andrew Weil, who suggested the replacement of the term ‘alternative medicine’ with the term ‘integrative medicine’ (21). Lastly, to assess both the risks and benefits of CAM, high quality research is necessary. There is an urgent need to establish and promote new study designs, combining the specific demands of CAM with scientifically based, randomized controlled trials.