
Abstract
The aim of this study was to estimate prevalence rates of different types of primary headache in 9- to 14-year-old children in a population-based sample. Case definition was based on International Classification of Headache Disorders (ICHD) criteria. The possibility of implementing these criteria within a questionnaire format, which has been regarded as problematic by some authors, was the main focus of the study. A questionnaire was sent to children and adolescents in 6400 randomly drawn families in southern Lower Saxony. Valid questionnaires were returned by 61.1% of the sample. The overall prevalence rate for tension-type headache (TTH) (criteria C and D) was 17.6% and for migraine (criteria B, C and D) 13.1%. Despite the use of abridged criteria for headache classification, 35.5% of all children reported headache that could not be classified using the ICHD criteria. The response behaviour of these children indicated that they had difficulties reporting symptoms that were defining for migraine or TTH. The classifiability of headache does not seem to be dependent on age or frequency of headache, but rather on the number of ‘I don't know’ answers given regarding headache characteristics. It is likely that studies reporting prevalence rates that are limited to migraine and or TTH diagnoses underestimate the true prevalence of headache in children and adolescents.
Introduction
Headache is common among children and adolescents. Epidemiological studies point to a 1-year prevalence of up to 68% (1). The International Classification of Headache Disorders (ICHD), published by the International Headache Society, delineates operationalized criteria for case definition, thus making prevalence rates of different types of headache comparable across different studies (2). These criteria were primarily developed for clinical use in adult populations. Implementation of these criteria in epidemiological research on paediatric headache involves two major problems: the applicability of these criteria to children and, due to economic reasons, the assessibility of the criteria in a questionnaire format.
The debate in regard to the applicability to children has focused on criteria regarding the number of previous headache episodes (3) and the duration of headache (4). As a result, the required duration for children was shortened from ≥ 4 h to ≥ 2 h in the second revised edition of the ICHD (ICHD-II, 2004) (5). Attacks < 2 h require corroboration by prospective diary studies. In relation to the criteria generally proposed for children, especially younger children may be unable to report migraine-defining features, resulting in underdiagnosis of migraine or tension-type headache (TTH) (6). In the discussion about the applicability of the ICHD criteria to children, several authors have noted that typical headache features for migraine are age dependent (7, 8). The limited ability of children to report specific headache symptoms becomes especially evident in epidemiological research via questionnaires. Recent epidemiological studies of headache in children and adolescents have used ICHD criteria for headache classification or focused on occurrence of headache. Questionnaires were often used as the sole source of information (9–15). However, a limited number of studies combined questionnaire and interview methods (7, 16, 17), and two studies have assessed the type of headache via interview alone (18, 19). Very few studies have implemented all ICHD criteria for migraine and/or TTH in epidemiological studies via questionnaires (12, 16, 17, 20). The studies differ not only as regards assessment method but also as regards operationalization. Zwart and colleagues, for example, summarized symptoms of migraine and TTH and then asked subjects to decide which description best fit their headache. In most studies, however, each ICHD criterion was assessed via an individual question (11, 13).
Studies have shown reduced concordance in the response behaviour of children concerning symptoms that did not occur regularly compared with more frequent symptoms (21, 22). This incongruence points to difficulties in responding to and/or understanding headache-related questions that are relevant for diagnosis according to the criteria of the ICHD. Assessing type of headache via self-report questionnaires without the opportunity to clarify comprehension problems may lead to a proportion of children being unable to answer some of the diagnosis-relevant questions. If there is an increasing ability to remember and verbalize relevant symptoms with age, it could be assumed that the response behaviour found in a questionnaire survey would reflect this. An increase of valid answers with age would be expected. Furthermore, age-dependency whether headache is classifiable according the primary headaches of the ICHD in an epidemiological study could be supposed, but remains unclear. Not only response behaviour and age, but also the number of headache episodes may be associated with the classifiability of headache to one of the main categories of primary headache.
In sum, the objectives of the present study were
To analyse response behaviour regarding headache-related questions relevant to ICHD diagnosis across gender and age.
To determine the association between age, gender, response behaviour and frequency of headache and non-classifiable headache.
Materials and methods
Subjects
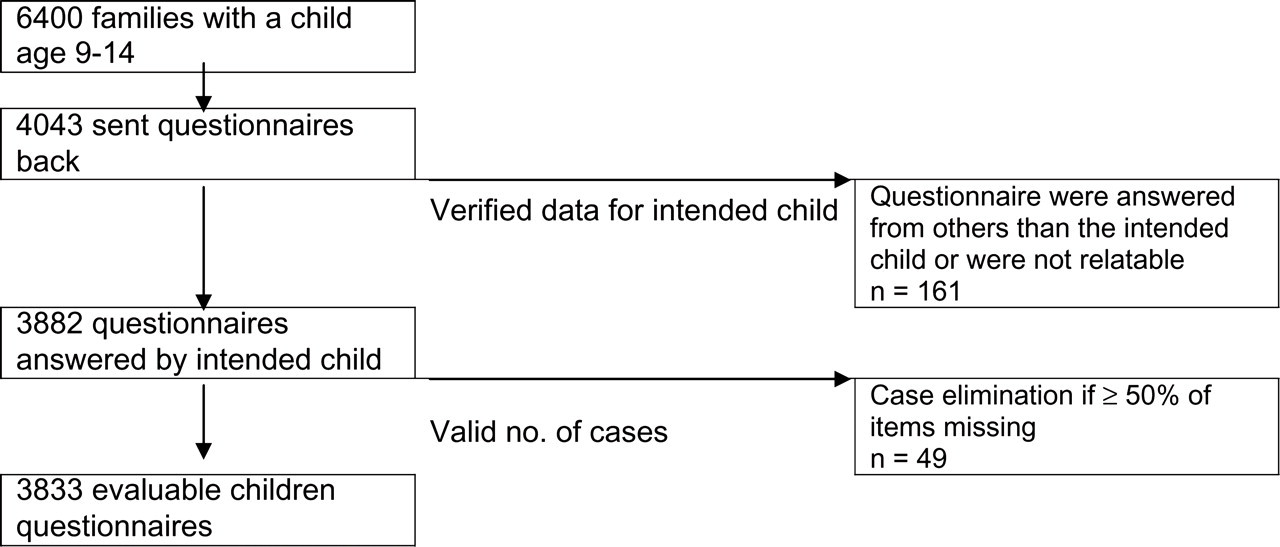
The sample of the study ‘Children, Adolescents & Headache’ consisted of an unselected population-based cohort of families with children and adolescents aged 9–14 years residing in four districts of southern Lower Saxony and the city of Hannover. A total of 6400 households with at least one child between 9 and 14 years old were randomly drawn from the community registries for the sample, constituting approximately 12.4% of the population of 9–14-year-olds. Data were collected via postal survey in the winter of 2003/2004. Survey implementation was conducted in accordance with Dillmann's recommendations for response optimization (23). Non-responding households were contacted twice following survey mail-out with reminders to complete and return the questionnaires. A lottery was implemented as an incentive to participation. Of the contacted families, 4043 returned the child questionnaire and 3833 of the questionnaires were determined valid (Fig. 1). Almost exactly half of the responding children were male (49.9%; female 50.1%). The average age was about 11 years (11.37;
Sample failures.
Questionnaire
Questionnaire items were based on measures used in prior studies on paediatric headache (8, 14, 15, 17, 24) and the criteria of the ICHD. As a gate question, children were asked if they had experienced headache in the last 6 months. If they answered ‘yes’, they were directed to questions regarding frequency, duration, intensity, location and quality of head pain and symptoms that may accompany headache. To assess headache intensity a numerical rating scale ranging from 0 (no pain) to 10 (worst imaginable pain) was used, which was transformed for headache classification into a categorical variable by grouping scores of 0–4 together as ‘mild to moderate’ headache and scores of 5–10 as ‘moderate to strong’ headache. Localization was assessed by asking the children to mark pain-affected areas on left- and right-hand-side images of the head. If the marked areas on the left- and right-hand side corresponded, localization was categorized as bilateral, otherwise as unilateral. Criterion A, amount of earlier headache episodes, was not assessed as it was considered too difficult for child response, especially for the younger children. Prior to implementation of the survey with the child questionnaire, all survey material underwent rigorous pretesting following the stages delineated by Dillmann (23).
The same reason led to the exclusion of criterion E, which requires the absence of an underlying (organic) cause and is difficult to fulfil without a clinical examination. The response categories in the questionnaire for the duration of headache did not differentiate further between headache lengths of < 1 h, thus operationalizing criterion B for TTH with some imprecision, as it stipulates a duration of 30 min to 7 days. In constructing the questionnaire, care was taken to ensure age-appropriate wording of instructions, items and response categories. To minimize missing items for headache-specific questions, a response category ‘I don't know’ was implemented.
Statistical procedures
The Statistical Package for Social Sciences (
Results
A total of 2553 of the school children (66.3%) who returned valid questionnaires reported having experienced headache in the last 6 months. The prevalence of head pain increased significantly with age: whereas headache was experienced by about half of the 9-year-olds (56.6%), it occurred in 75.1% of the 14-year-olds. Headache prevalence was also higher among girls than boys (χ2 = 18.926, d.f. = 1, P < 0.001). Older girls, in particular, reported higher headache prevalence and headache frequency (χ2 = 71.197, d.f. = 6, P < 0.01). One-sixth of all children (16.7%) experienced headache on a weekly basis, whereas 20.9% experienced headache one to three times a month, and 28.6% experienced headache less frequently.
Response behaviour
The frequency of ‘I don't know’ answers in contrast to the other response categories revealed that pain quality (criterion C) was most often answered with ‘I don't know’ (26.8%), followed by 23.4% of the children concerning duration of headache. Regarding localization of headache, the category ‘I don't know’ was used by 17.5% of children with headache, whereas 1% marked the chin and/or jaw region of the face. Ten per cent of the children were not able to report the intensity of headache (answer category ‘I don't know’). Regarding accompanying symptoms, the largest proportion of ‘I don't know’ answers was given for aggravation by routine physical activity (13.4%), followed by photophobia (7.4%) and phonophobia (6.5%), with the smallest proportion given for nausea and vomiting (3.7%) (Table 1).
Headache symptoms across gender and age

∗Nausea and vomiting.
†Aggravation by physical routine.
The proportion of valid answers increased significantly with age regarding the following three headache symptoms: pain quality (χ2 = 85.802, d.f. = 2, P < 0.01), duration of headache (χ2 = 23.041, d.f. = 2, P < 0.01) and headache intensity (χ2 = 12.278, d.f. = 2, P < 0.01). A significant gender difference was found in four of the eight headache variables, i.e. duration (χ2 = 14.456, d.f. = 1, P < 0.01), aggravation by physical routine (χ2 = 5.995, d.f. = 1, P < 0.05), intensity (χ2 = 9.772, d.f. = 1, P < 0.01) and phonophobia (χ2 = 10.249, d.f. = 1, P < 0.01). For each of these variables girls responded significantly more often with ‘I don't know’ than boys.
Type of headache
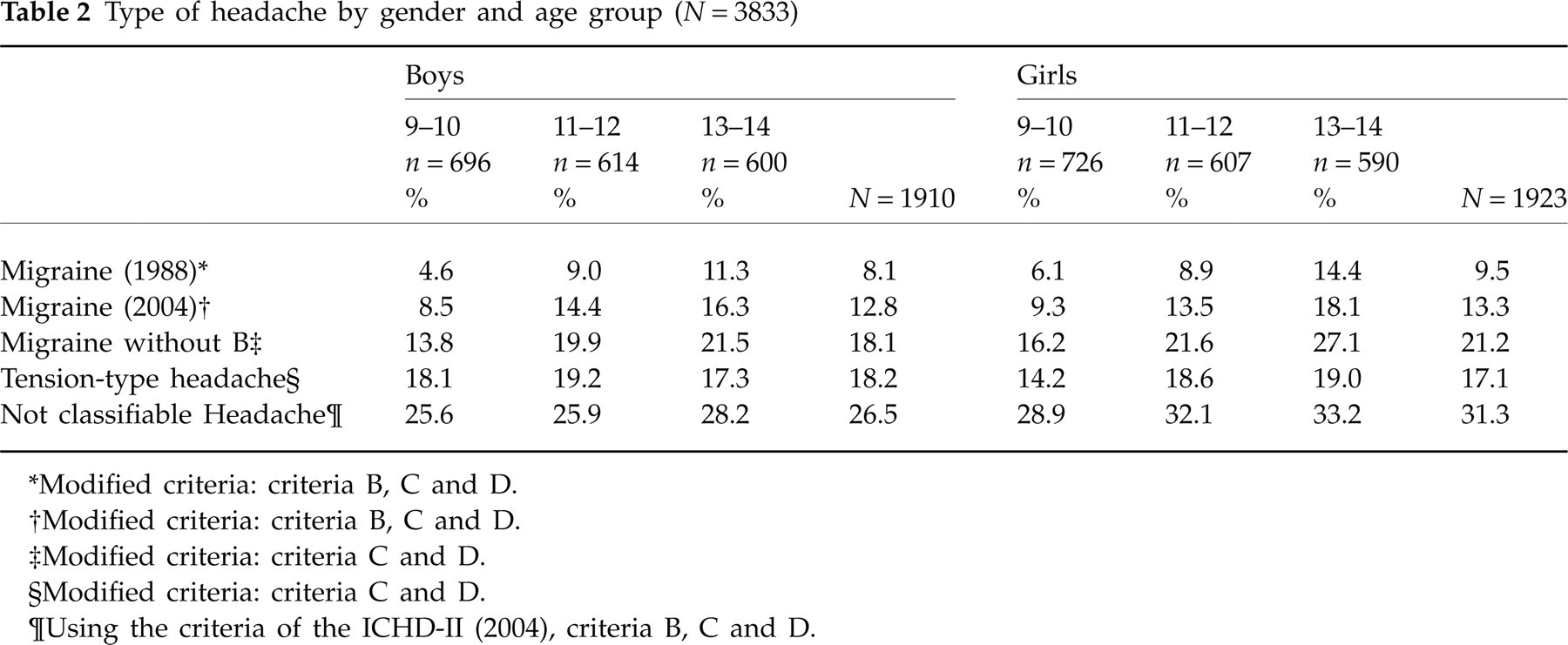
The prevalence of migraine-like headache (criteria A and E excluded) according to the ICHD-II (2004) (5) was 13.1%, according the ICHD (1988) (2) 8.9% in the present sample. The prevalence of TTH was 17.6% (criteria A, B and E excluded). The proportion of children with non-classifiable headache was 35.4% when using ICHD-II (2004) and 39.4% when using the earlier version of the ICHD (1988). Of all children with headache in the last 6 months, less than one-half (46.4%) could be diagnosed with migraine or TTH using the classification of 2004, leaving 53.6% with non-classifiable headache. The proportion of children with diagnosable headache was significantly higher when employing the 2004 classification than with the 1988 criteria (χ2 = 1065.468, d.f. = 1, P < 0.01). Table 2 shows the different types of headache across gender and age groups. There was an increase of migraine across the age groups (χ2 = 19.074, d.f. = 1, P < 0.001), but no difference between boys and girls. There was no difference across the age groups regarding TTH, but boys had TTH more often than girls (χ2 = 6.392, d.f. = 1, P < 0.05).
Type of headache by gender and age group (N = 3833)
∗Modified criteria: criteria B, C and D.
†Modified criteria: criteria B, C and D.
‡Modified criteria: criteria C and D.
§Modified criteria: criteria C and D.
¶Using the criteria of the ICHD-II (2004), criteria B, C and D.
Variables associated with non-classifiable headache
The proportion of children with headache that could be classified according to ICHD-II increased with age (χ2 = 6.492, d.f. = 2, P < 0.05), and was larger among boys than girls (χ2 = 8.253, d.f. = 1, P < 0.01). Closer examination of children with non-classifiable headache revealed that 48.2% of these children fulfilled at least two criteria of migraine. Criteria B and C were fulfilled by 22.3%, C and D by 18.7%, and B and D by 7.2%. Children with non-classifiable headache responded more often with ‘I don't know’ to headache-specific questions than those with migraine and TTH (Table 3). In 9.4% of cases the number of ‘don't know’ answers made classification impossible.
Headache symptoms across the types of headache (N = 2538)

∗Nausea and vomiting.
†Aggravation by physical routine.
Logistic regression analysis was conducted with the dependent binary variable ‘classifiable headache’ vs. ‘non-classifiable headache’ plus age, sex, number of ‘don't know’ answers, and frequency of headache as independent variables. For the dependent variable, ‘classifiable headache’ was selected as the reference category, for the independent variable headache frequency the category ‘seldom headache’ was selected as reference category. The results showed that non-classifiable headache was strongly associated with the number of ‘don't know’ answers [odds ratio (OR) 2.33, confidence interval (CI) 2.12–2.56, P < 0.001], but unrelated to age, sex or frequency of headache. The model explained a moderate amount of the variance (Nagelkerke's R 2 = 0.215).
A second, analogue analysis was performed with headache classifiability as the dependent variable plus specific headache symptoms as independent variables. Accordingly, children with missing values on items regarding specific headache symptoms were excluded from analysis, which led to a reduction of sample size (n = 995). Non-classifiable headache was associated with headache duration of ‘less than an hour’ (OR 8.52, CI 5.26–13.81, P < 0.001), pulsating pain quality (OR 3.02, CI 2.20–4.16, P < 0.001), aggravation by routine physical activity (OR 2.77, CI 1.96–3.93, P < 0.001), moderate to severe intensity (OR 8.52, CI 5.26–13.81, P < 0.001) and vomiting and nausea (OR 2.52, CI 1.51–4.21, P < 0.001). Phono- and photophobia did not attain significance in the model. This model also explained a moderate amount of the variance of headache classifiablity (Nagelkerke's R 2 = 0.287).
Discussion
In this population-based study of 3833 children aged 9–14 years, 66.3% (2553) experienced headache in the last 6 months. The prevalence of headache increased with age, especially in girls. The female preponderance was most pronounced among the 13- to 14-year-olds. Not only was headache more widespread among girls, it also occurred more frequently: girls reported frequent headache (weekly headache) more often than boys, especially in the older age group. The prevalence rate in the present sample (66.3%) is somewhat higher than that reported by Laurell and colleagues (44.8%) and Bener and colleagues (39.5%) (10, 17), which were comparable with regard to the examined age group.
Response behaviour
Analysis of response behaviour indicates that the items regarding duration of headache, pain quality, and localization of headache were the most difficult to answer. This finding is in line with previous studies, which reported difficulties in the same areas (6, 8). Laurell and colleagues found much lower rates of invalid answers (‘don't know’ answers and missing), but showed a comparable ranking order, with pain quality and duration as the most difficult items to respond to and nausea as the most consistently answered item (10). Laurell and colleagues had the questionnaires filled out in class, in the presence of a teacher or another person who could answer questions. In the present study, parents received explicit instructions not to influence the child, and only to answer questions to enable their child to comprehend the questionnaire. The difference in the amount of invalid answers may be due to the setting, as admitting ‘I don't know’ in the classroom may be associated with negative consequences. In any case, our data demonstrate an age-dependent increase in valid answers to items regarding pain quality, duration and intensity of headache. Girls appear to have more difficulties than boys answering questions regarding headache duration and intensity, phonophobia and aggravation by physical activity.
In general, the allowance of the answer category ‘I don't know’ may limit the ability to classify headache, but as our main interest was the reduction of ‘missings’ we took this ability into account.
Type of headache
The ICHD classification system for primary headache was developed to enhance comparable case definition across studies. Nevertheless, difficulties regarding the applicability of these criteria in epidemiological research on paediatric headache have led researchers to employ modified criteria, in particular when assessment was conducted via questionnaire. For example, the migraine criteria A and/or E have been excluded in some studies (9, 15). We shared the concerns regarding the applicability of these criteria. We also refrained from assessing criterion E for migraine and TTH.
Based on the ICHD (1988) criteria, the 6-month prevalence of migraine in our sample of 8.9% is in line with other studies. Al Jumah et al. reported a lower 1-year prevalence rate of 6.2% for migraine (13), whereas other studies have reported slightly higher 1-year prevalence rates of 10.4% (16), 11% (10) and 13.7% (17). Studies with older children (11–18 years old) have yielded similar 1-year prevalence rates, ranging between 5.2% and 8.8% (11, 12, 25).
The 1-year prevalence rates of TTH in previous studies ranged from 9.8% reported by Laurell (10), when using strict ICHD criteria, to 24.7% reported by Özge et al. (16). The 6-month prevalence rate of TTH in our sample is in line with these data (17.6%). The data are best comparable concerning the operationalized criteria to the study by Laurell and colleagues (10), and their results are similar to the presented data. Using reduced criteria (excluding migraine criteria A and B), they obtained a prevalence rate of 17% for migraine (exclusion of criterion B leads to a prevalence rate of 19.7% in the present study). The prevalence rate of TTH with reduced criteria (exclusion of criteria A and B) reported by Laurell and colleagues (23%) is higher than that in the present study (17.6%).
In our sample, 35.5% of all children reported headache, which due to the pattern of responses to headache questions was not classifiable as migraine or TTH, the two main primary headache diagnoses. The percentage of children with non-classifiable headache in Laurell and colleagues' study is not explicitly reported, but can be inferred from the given data and appears with 15.2% to be somewhat lower than in the present study. The lower proportions of children with non-classifiable headache in their study may be associated with the lower proportion of invalid answers. Özge et al. do not report the number of children with headache that cannot be classified according to ICHD criteria, but 14.17% of all children seem to have experienced headache, yet did not receive one of the diagnoses. The lower rate in their study may be due to the fact that they validated the questionnaire data in a clinical interview. In the study by Anttila et al., approximately 20% of all children had headache that only partially fulfilled the criteria for migraine or TTH, and 6% of the sample had non-classifiable headache (26). The German study conducted by Pothmann and colleagues found, comparable to our study, a rate of 29% with non-classifiable headache (15).
Contrary to Laurell and colleagues (10), we found no age-related increases in prevalence of migraine or TTH. An increase in TTH with age was reported by Pothmann and colleagues (15), but they found no increase in migraine with age.
Variables associated with non-classifiable headache
Despite differences across age groups as regards valid answers to some of the specific headache symptoms, there was no significant association between age and classifiability of headache in the logistic regression model. Some authors have postulated that typical symptoms defining the ICHD categories of migraine and TTH will increase with age, because of improved ability to describe headache in ICHD-relevant terms (8), a better recognition of headache symptoms, and more headache experiences (21, 22). The present data do not confirm a strict association between age and classifiability of headache. Instead, the amount of ‘I don't know’ answers seems to have the most influence on whether headache is classifiable or not, and is not only related to age or to sex.
A closer look at headache symptoms reveals that classification into either migraine or TTH depends on whether typical migraine features are present or not (pulsating pain, aggravation by routine physical activity, moderate to high pain intensity and nausea). Despite the exclusion of criterion B in TTH, the main predictor for non-classifiable headache was headache duration of < 1 h. Non-classifiable headache seems to represent a brief form of migraine or probable migraine. In a clinical sample, Rossi and colleagues reported that clinical features of both migraine and TTH were present in a single headache episode in about 20% of children. Furthermore, they described great intraindividual variability of headache symptoms in 15% of their sample (8). As a result, the authors question whether a distinction between migraine and TTH is appropriate for paediatric age groups. According to their research, it could be supposed that a certain amount of the non-classifiability found in the present research is due to children with intraindividual variations in headache symptoms and/or the presence of both types of headache.
Anttila et al. noted that unilateral pain and phonophobia may be more typical of childhood TTH than of TTH in adults (26). This description raises questions regarding the strictness with which the ICHD-II criteria were employed in the study. It may also point to the limited usefulness of the ICHD-II criteria in paediatric epidemiological research.
Conclusions
The main recommendation that can be derived from our findings in order to enhance comparability between epidemiological studies on headache is to analyse and report specific headache features in addition to ICHD diagnoses. In light of the high proportion of ‘don't know’ answers in our study, which reflect difficulties the children and adolescents had in responding to some of the headache items, it may be useful to supplement prevalence rates on the basis of ‘strict’ ICHD criteria with prevalence rates using ‘reduced’ criteria (limited to criteria C and D of TTH and migraine). Furthermore, the report of response behaviour in children, e.g. missing behaviour and amount of ‘don't know’ answers, may be helpful to decide which features and which question and/or answer formats are most suitable for children. Our data indicate that the applicability of the ICHD criteria in an epidemiological study via questionnaire without the opportunity to clarify misunderstandings and to assess different types of headache in the same child is reduced. Studies reporting only classifiable headache and associated complaints may underestimate the occurrence and burden of headache in children and adolescents.
Footnotes
Acknowledgements
This research project has been supported by a grant from the German Ministry of Education and Research within the German Headache Consortium.