
Abstract
We aimed to determine the prevalence of primary headache among schoolchildren in the city of Agri, located in eastern Turkey, where geographical, climatic and socio-economic conditions differ greatly from those of other regions of Turkey. A cross-sectional school-based (ages ranging from 11 to 18) study was conducted from January to April 2006. Diagnosis was based on the second edition of the International Classification of Headache Disorders. This population was evaluated by a two-stage clustered sampling procedure. In the first phase, 1385 children were asked whether they had had a headache within the past year. For the second-step interview, 540 children (38.9%) with a complaint of headache were selected. Five children who had complained of headaches in the first interview did not agree to participate in the second stage. Of the remaining 535, 473 were identified as having primary headache and 62 as having secondary headache. Overall, one-year prevalence of headache subtypes was 14.3% for migraine, 3.5% for probable migraine, 8.6% for pure tension-type headache, 4.6% for migraine plus tension-type headache, and 3.0% for probable migraine plus tension-type headache. The prevalence of migraine was higher in our study than in previous studies.
Introduction
Headache is a common symptom and complaint in pediatrics and pediatric neurology and is increasingly prevalent (1). In epidemiological studies conducted in children and adolescent populations worldwide, a variety of prevalence rates have been reported for migraine and tension-type headache (TTH) (2–15). Results varied widely due to social, genetic, cultural and geographical differences. Differences in reported prevalence rates may also be related to the different classifications used in this field (16–18). In Finland, 52% of seven-year-old children reported headaches in 1992, compared with 14% in 1974 (19). Among adolescents, more than 25% of 12–13-year-olds experienced headaches at least once a week, and there was an increase in prevalence over two years in Canada (20). Other published studies report the prevalence of headache in the seven-year-old group as 37%–51%, and state that it gradually increases to 57%–82% in the 15-year-old group (2,21). Other studies have shown that recurrent and frequent headaches are seen in approximately 2.5% of seven-year-old children, with prevalence increasing to 15% at 15 years of age (7,21).
Many previous studies, based on the 1988 International Headache Society (IHS) criteria, proved to be less sensitive and less specific for the diagnosis of migraine in children (17). Modification of the International Classification of Headache Disorders (ICHD) criteria in various domains has been suggested in order to improve the diagnostic sensitivity for migraine (22–25). ICHD-II has proposed important changes in the diagnosis of migraine for children and adolescents despite the preservation of some debatable criteria such as duration and number of attacks. By increasing sensitivity and specificity in the diagnosis of migraine, ICHD-II represents an improvement over the previous ICHD criteria (18,26). Understanding the changes in prevalence, and devising optimal management strategies, will depend on further research, which should provide a greater understanding of the pathogenesis, roles of genetic and environmental factors, and classification and validity of headache syndromes (19,20,27).
A limited numbers of epidemiological studies have been performed in Turkey. Among them, few up-to-date studies of headache exist, performed in limited areas (5,28–31): socio-economically developed centers and cities sharing similar geographical and climatic conditions, located in western part of Turkey. Prior to our study, no prevalence study had been conducted in eastern Turkey, which is quite distinct in terms of climate, geographical and socio-economical conditions.
In this study, ICHD-II, having greater sensitivity and specificity, particularly for migraine, was used instead of the ICHD-I or ICHD revised criteria (ICHD-R) used in previous epidemiological studies. In addition to determining the prevalence of primary headache subtypes in children according to ICHD-II in Agri, we also aimed to present the characteristics and relevant factors for primary headache subtypes using a neurologist’s diagnosis.
Patients and methods
Study design
This cross-sectional descriptive study was conducted in the city of Agri (Figure 1) in eastern Turkey from January to April 2006. Agri had a population of 73,800 as reported in the 2000 census, and has an altitude of 1800 meters. Climate greatly varies with the season, and winters are extremely cold. Annual temperature varies from −43°C to 34°C. Agri has a low per capita income, ranking 80th in annual gross income among the 81 cities of Turkey. The people of Agri consume mainly animal products, especially meat. In the Turkish national education system, it is obligatory to have a primary school education and earn a diploma. High school education is on voluntary basis.
Agri is located in eastern Turkey.
There are 36 schools (25 primary schools, 11 high schools) in Agri. The total number of students attending high schools (male : female [M : F], 3981 : 1602) and primary schools (M : F, 11141 : 8836) was 25,560. Among these schools, only the students of one primary school and one high school were of moderate-to-high socio-economic status. The schools were classified into two groups: those having low and moderate-to-high socio-economic levels according to the District Education Directorate. A total of seven schools (two high schools, five primary schools) were randomly selected for the study. Among participating schools, classes were randomly identified by using a raffle and the students in those classes were evaluated. A computer program was used to estimate the number of subjects to be interviewed based on the prevalence figure of 20% with a 95% confidence interval (CI) and desired accuracy of 3%. The study recruited 1346 children of 11 to 18 years of age attending primary school or high school. The study sample was stratified according to sex, type of school (primary or high school) and socio-economical status (moderate-to-high or low).
First interviews of all the students were conducted in the exam room provided by the school administration. This interview was carried out by a single neurologist (RA). In the first-phase interview, 1385 children were asked whether they had had a headache within the past year.
For the second-stage interview, a total of 540 children (38.9%) with a complaint of headache were selected. One senior pediatric neurologist and two senior neurologists applied a questionnaire inquiring about socio-demographic features and all characteristic features of primary headache syndromes mandatory for classification. In the first part of the questionnaire, socio-demographic features were covered (name, last name, phone number, age, sex, number of siblings, child’s birth order in the family, maternal and paternal age and occupations, whether there was a divorce in the family, whether any of the parents smoked, whether there was any prior physician visit due to a headache, the specialty of the physician visited and her/his diagnosis, whether there was any motion sickness and whether the family environment was a happy one from the perspective of the child). In the second part of the questionnaire, the age of onset for the attacks, the characteristics of the headache (how many attacks had been experienced so far, the frequency of the headache, duration, localization, quality, severity, relationship to physical activity), symptoms accompanying the attacks (nausea, vomiting, photophobia, phonophobia, stomachache, dizziness, asthenia), factors precipitating and alleviating the headache, individuals with a history of headache in the family and their degree of relatedness were covered. Those with headache complaint were then asked additional questions to evaluate the temporal relationship of the headache to upper respiratory tract infections, head or neck trauma or other diseases accepted as exclusion criteria, indicating secondary headache.
Although aura is a less reliable phenomenon in children than in adults, we tried to ascertain visual symptomatology to the extent possible. Aura identified in this study was classified as visual, sensorial, visual-sensorial or verbal. Aura was accepted as visual if it was consistent with zigzag lines, colored lines, blind spots, micropsia, macropsia, visual field defects, blurred vision or colored circles. Blurred vision was accepted as a non-specific visual symptom, especially if it persisted during the headache period. Tingling and pricking sensations of the tongue, face and extremities as well as numbness were evaluated as sensorial symptoms.
Primary headache patients filled out the Pediatric Migraine Disability Assessment Questionnaire (PedMIDAS) (32) and visual analog scale (VAS). The classification of headache was based on ICHD-II (18). The Research Local Ethics Committee approved this study.
Statistical analysis
Data were entered and analyzed in a database that was prepared with the SPSS 11.5 (SPSS Inc. USA-Product ID: 19268001-740935192691, serial number: 3889132) for Windows program. Children were divided into two groups based on age: (1) age 14 and younger and (2) older than 14 years of age. Associations between categorical variables were analyzed using the Chi-square test. The level of significance was set to 5%.
Results
Socio-demographical features of 535 students identified as having headaches
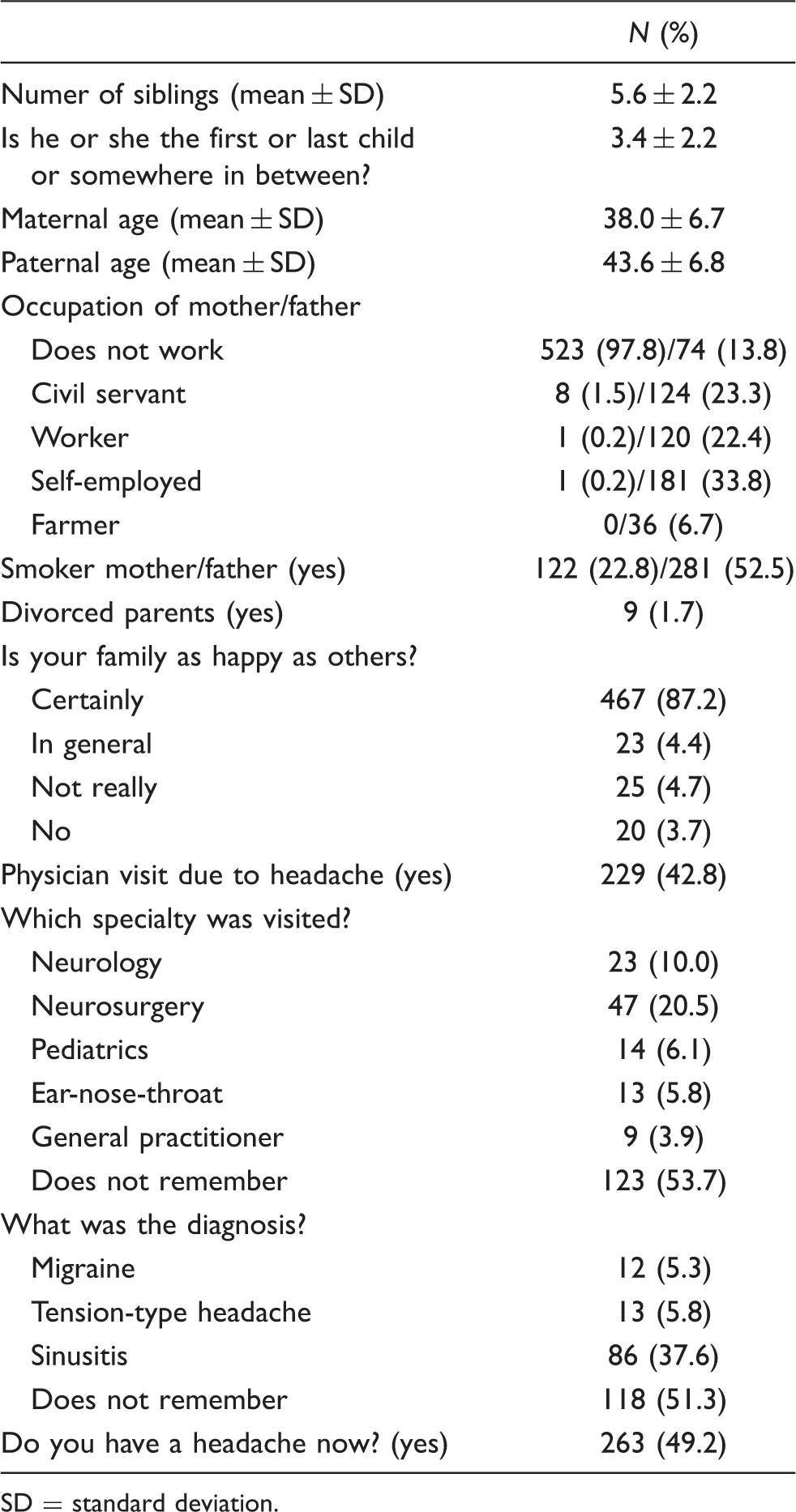
SD = standard deviation.
The distribution of children with primary headaches according to ICHD-II criteria was as follows: 198 children (overall one year prevalence: 14.3%) were diagnosed with migraine, and 49 children (overall one year prevalence: 3.5%) had a diagnosis of probable migraine (PM). Additionally, 65 children (4.6%) were diagnosed as migraine plus TTH, and 42 children (3.0%) were diagnosed as PM plus TTH. Thus, a total of 354 children (25.5%) were diagnosed with migrainous headache. Of the 354 children with migraine, 160 were girls and 194 were boys. The prevalence of migraine was found to be 29.5% in girls and 23% in boys. Migraine was 1.45-fold more frequent among girls than among boys (odds ratio [OR]: 1.45; [95% CI: 1.02–2.06].
Classification of headache disorders and their prevalence in school-age children in Agri

TTH = tension-type headache. ETTH = episodic tension-type headache.
Primary headaches can be listed as migraine, pure TTH, PM or probable TTH; however, in certain patients there may be overlapping between these categories (Figure 2).
Overlapping of primary headache subtypes. M = migraine. PM = probable migraine. TTH = tension-type headache.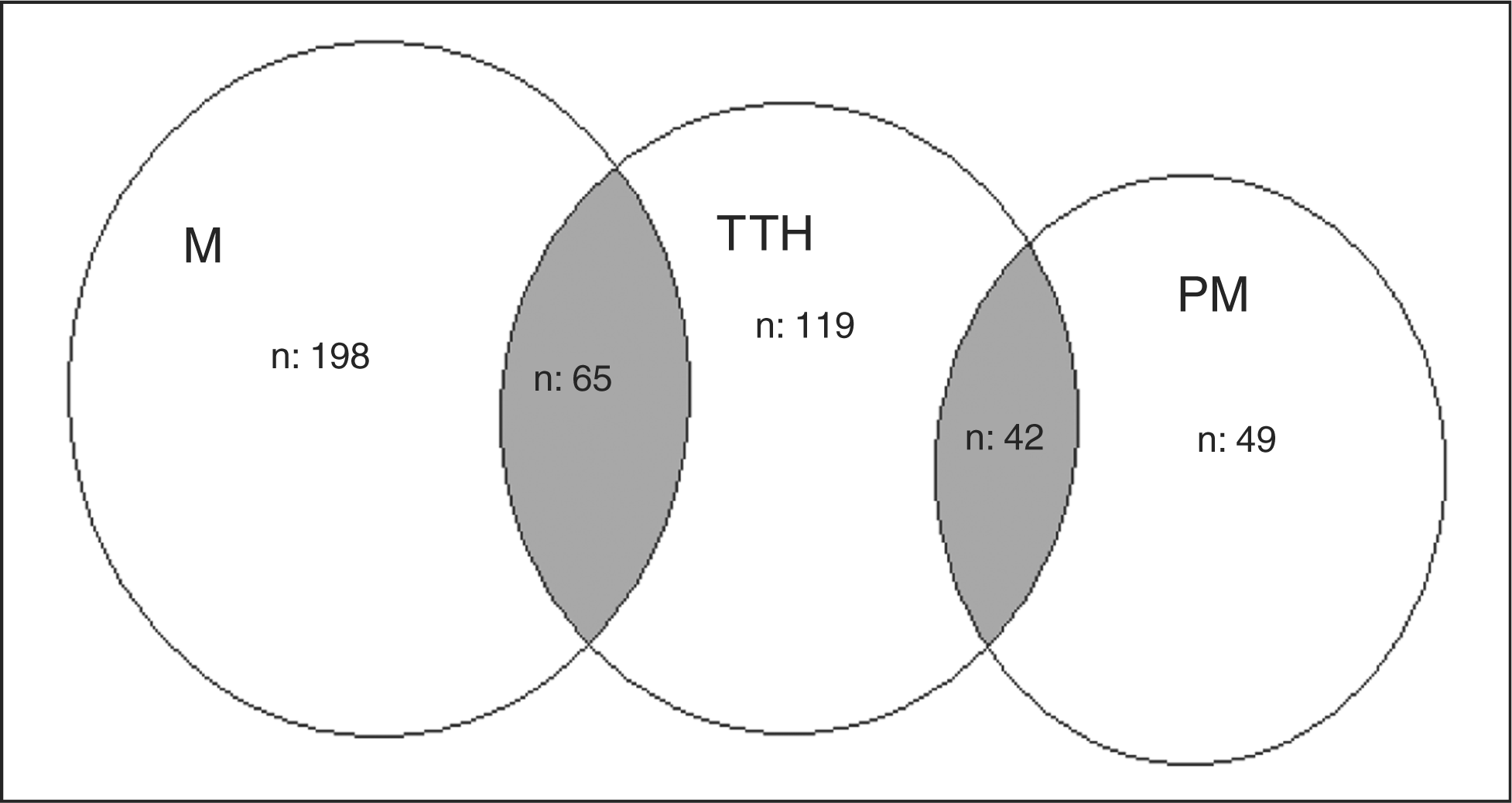
For girls below the age 14, the prevalence of migraine was 5.6%; for boys below the age of 14 it was 3.6%. For girls above the age of 14, the prevalence of migraine was 2.6%; for boys above the age of 14 it was 2.4%. In girls below the age of 14, the prevalence of pure TTH was 3.0%; for boys below the age of 14 it was 2.3%. In girls above the age of 14, the prevalence of pure TTH was 1.2%; for boys above the age of 14 it was 2.1%. In adolescents of low socio-economic status, the prevalence of migraine was 10.3% and that of pure TTH was 4.7%. In students of moderate-to-high socio-economic status, the prevalence of migraine was 4.0% and that of pure TTH was 3.8%. When socio-economic status is taken into consideration, total migraine was identified as being more prevalent among students of a low socio-economic status (79.9%, X2 = 14.41, p = .000). When we elaborate on the relationship between socio-economic status, sex and migraine, migraine was more common among girls of low socio-economic status, whereas TTH was more common among boys of low socio-economic status (42%, X2 = 2.13, p = .05; 35.7%, X2 = 2.27, p = .01, respectively).
Pain characteristics of cases with primary headaches
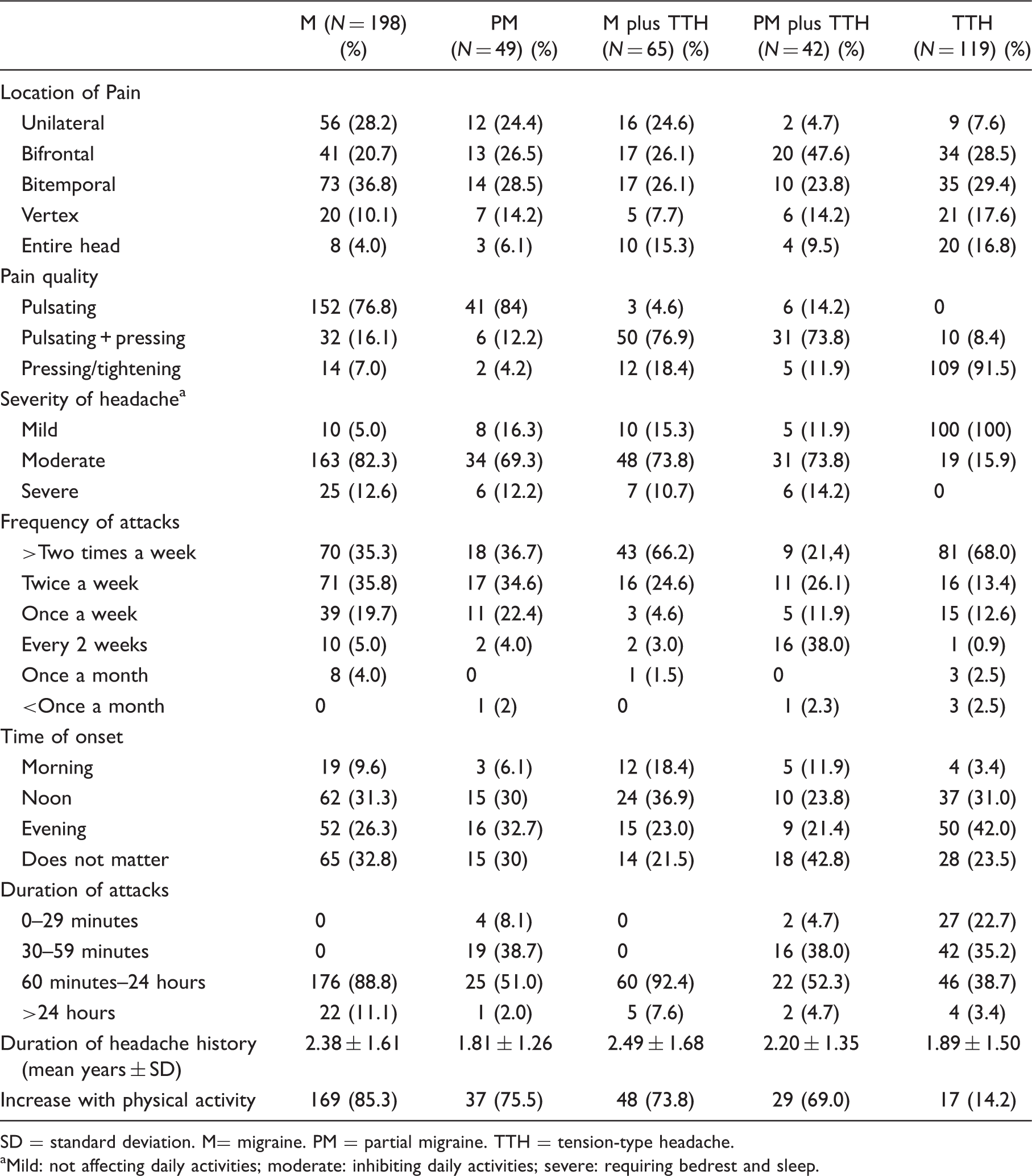
SD = standard deviation. M= migraine. PM = partial migraine. TTH = tension-type headache.
Mild: not affecting daily activities; moderate: inhibiting daily activities; severe: requiring bedrest and sleep.
The duration of the headache period was reported as 306 minutes on average in adolescents with migraine. In the PM group, headache was reported to last for less than an hour in 23 of 49 children (46.9%). Headaches in these patients had all the characteristics of migraine, except for duration. Fewer than five episodes were reported in 19 patients (27%).
Accompanying symptoms in primary headache

M = migraine. PM = probably migraine. TTH = tension-type headache.
Precipitating and alleviating factors in primary headache subtypes

M = migraine. PM = probably migraine. TTH = tension-type headache.
Aura types and distribution of symptoms

Mean VAS and PedMIDAS scores in primary headache subtypes are presented in Figures 3 and 4, respectively. Absentee days were highest among students with migraine: 2.1 days/3 months on average.
The relationship between Visual Analog Scale (VAS) score and headache subtype. M = migraine. PM = probably migraine. TTH = tension-type headache. Relationship between Pediatric Migraine Disability Assessement (PedMIDAS) score and primary headache subtype. M = migraine. PM = probable migraine. TTH = tension-type headache.

There was a family history of headache in 74% of all those with primary headaches: in 84.8% of all patients with migraine and in 69.7% of patients with pure TTH. For migraine patients, this family history was paternal in 16.4% of cases, maternal in 47.7% of cases, and from both parental sides in 35.9% of cases.
Discussion
This study has numerous methodological differences compared with previous reports. Epidemiological data for migraine and other recurrent headaches in children are usually based on studies compiling information by using self-administered questionnaires and classifying symptoms according to a variety of classification systems. Instead of using a self-administered survey, which is a less sensitive method for diagnosis than a clinical interview (3), the present data were collected via face-to-face interviews performed by individuals specially trained in the differential diagnosis of headache disorders. This study design has been used in few reports (5). The age range of the sampled populations in previous studies was also different. In this study, children younger than 10 years of age were excluded because history given by young children can be unreliable. Another advantage of this study is the high rate of coverage for the target population, indicating that the study group represents the population fairly well. Limited numbers of studies are performed in this manner.
Lack of standardized case identification has made epidemiological studies of headache difficult, leading to great variations in prevalence and incidence calculations of primary headache disorders in children (8–16). In a study carried out in Mersin, Ozge et al. found the prevalence of migraine to be 10.4%, relying on IHS criteria, and the prevalence of TTH to be 24.7% (5). In a study in the Aegean region, the prevalence of migraine was 8.8% (27). In an Istanbul-based study by Turkdogan et al., the prevalence of migraine was 9%, and the prevalence of TTH was 6.1% (29). The prevalence found in our study is higher than that found in other studies in Turkey. This discrepancy may relate to regional differences, differences in diagnostic criteria, or differences in age groups as well as the study design.
The prevalence of migraine varies according to age and gender. It is 3.7%–11% at 3 to 7 years of age, 4%–11% at ages 7 to 11, and 8%–23% during adolescence (21). The mean age of onset for migraine has been reported as 7.2 years for boys and 10.9 for girls (4,6,32). Migraine prevalence before adolescence is higher among boys; thereafter, prevalence increases more rapidly in girls than in boys (2,33). Prevalence increases up until age 40, approximately, and then begins to decrease (34); however, in the present study, the prevalence of migraine was higher among primary schoolchildren than in adolescents attending high school. Results similar to ours can be found in the prevalence study by Gupta et al. performed in India. In that study, migraine prevalence was 17.2% for early adolescents and TTH prevalence was 11% (35).
In our study, 34.4% of all migraine patients experienced aura, with visual aura being the most common. These results are similar to those found in the literature (36–38).
In this study, patients with migraine and patients with PM demonstrated similar headache characteristics. Indeed, 46.9% of patients diagnosed as having PM were given this diagnosis only because the duration of their headache was shorter than 1 hour. Only four of these patients experienced headaches shorter than 30 minutes. According to ICHD-II criteria, minimum duration of headache is 1 hour; therefore, this patient group, bearing all the characteristic of migraine, could not be diagnosed as having migraine. Furthermore, in this group of patients the factors precipitating and alleviating the headache were similar to those found in the migraine group. A change in diagnostic criteria of migraine with reevaluation of the length of an attack might change the rates of diagnosis of migraine.
In addition, migraine and TTH, the most common episodic headache types, are often accompanied by features of each other, an occurrence that complicates differential diagnosis. Another striking finding of our study was the presence of a group of patients who could be located between migraine and pure TTH, but in terms of their clinical presentations were closer to migraine. In these patients the localization of pain, its severity and duration were similar to those of migraine, but the frequency of attacks correlated with that of TTH. The quality of the headache was both pulsatile and tightening. Symptoms accompanying the headache, and patients’ VAS and PedMIDAS values, were similar to those of the migraine group. TTH subjects with migrainous features and migraine subjects with TTH features might occupy a place between TTH and migraine on the spectrum. A similar situation applies to patients with PM and those with TTH (Figure 2; Tables 3 and 4). Kienbacher et al. followed up 227 patients for a long period of time and reported that 25.7% of patients with an initial diagnosis of migraine converted to TTH and 20.7% of patients with an initial diagnosis of TTH converted to migraine (39). The overlapping forms identified during the effort to determine overall one year prevalence in our study can accommodate those patients whose headache types can convert from one type to another.
Epidemiological data for the prevalence of TTH in children and adolescents are more limited than data for the prevalence of migraine in these age groups. Estimation of the prevalence of TTH in these groups varies on a large scale, from 0.9% to 72.8%, most likely because of the differences between the methods used (2–8). The prevalence of TTH was found to be 8.6% in our study. This figure increases to 16.3% when the group of patients having TTH coexisting with migraine is included. The effect of gender on TTH is less consistent than its effect on migraine. In a study by Laurell et al., increasing prevalence with age was shown particularly in girls with migraine (6). In our study, when all age groups are considered, as is the case in the Laurell study, TTH was found to have a higher prevalence rate among girls. However, in children above the age of 14, TTH prevalence was higher among boys. This observation differs from the literature.
A positive family history is more frequent among patients with migraine than among those with TTH. The role of genetic predisposition in headache is well known, particularly in migraine. Several studies performed on twins have shown that the genetic contribution to migraine is approximately 50% (40). In the present study, 74% of all primary headache sufferers, 84.8% of migraine cases and 69.7% of all patients with TTH had a positive family history for headache. For migraine, this family history was more common on the maternal side.
Patients with migraine and those with higher socio-economic status are reported to be more likely to seek care from a specialist or from a headache clinic. Thus, from the perspective of clinic attendance it would seem as if the prevalence of migraine and socio-economic status are directly related; however, an exactly inverse relationship has been observed in population screening studies (41). Studies of the effect of social status on the prevalence of headache commonly report a significant negative correlation between socio-economic status and prevalence of headache (2,19). The relevance of psychosocial factors (low socio-economic status, poor housing conditions, school problems, poor relationships with peer groups) was investigated in depth in several studies (5,19). In the present study, we observed migraine as being prevalent among children with low socio-economic status; however, there was no relationship between TTH and socio-economic status.
In the present study, which was performed in a region with socio-economic, climatic, and geographic characteristics different from those in previous studies in Turkey, the prevalence of migraine was higher than that of TTH. This may be related to the geographic and climatic characteristics of the region, as well as the nutritional habits or lower socio-economic status of the patient population. The use of ICHD-II criteria may also be a reason for this finding. Further studies are required to explain this observation.
Footnotes
Acknowledgements
This study was presented at the 2008 International Congress of Childhood Headaches in Istanbul. The authors thank Professor Dr Mustafa Ertaş for editing the manuscript.