
Abstract
Objective:
To investigate behavioral and emotional symptoms in a community-based sample of children as a function of headache status and of headache frequency.
Methods:
Our sample consisted of 1,856 children (5–11 years). Primary headaches were assessed using a validated headache questionnaire. Emotional symptoms were assessed by the Child Behavior Checklist (CBCL). CBCL scores were modeled as a function of headache status after adjustments for demographics and headache frequency.
Results:
Relative to controls, children with migraine were significantly more likely to have abnormalities in the following CBCL domains: somatic, anxiety-depressive, social, attention, internalizing and total score. Children with tension-type headache (TTH) were significantly different from controls in the same domains but at a lower rate than migraine. In children with migraine, impairments significantly varied as a function of headache frequency, race, and income. In children with TTH, gender, age, and headache frequency were significantly associated with abnormal scores.
Conclusions:
Migraine and TTH are significantly associated with behavioral symptoms in several domains, and headache frequency affects the association. Internalizing symptoms are common in children with headaches, while externalizing symptoms (e.g. rule-breaking and aggressivity) are not significantly more common than in controls.
Introduction
Primary headaches are common in the pediatric population (1). When the International Headache Society criteria are strictly followed, prevalence of migraine in children ranges from 3.3% to 21.4%, increasing from early childhood to adolescence (1). The burden of pediatric headaches is best characterized for migraine, which impacts the child's quality of life and (2) school attendance (3), and sometimes disrupt the family (4). The impact associated with migraine seems to be influenced by several factors, including severity of pain and of associated symptoms, frequency of pain, anticipatory anxiety and adequacy of treatment (5,6).
Several conditions are comorbid with migraine (7,8). Comorbidities can alter the clinical course of diseases by affecting time to detection, prognosis, therapeutic selection and post-therapeutic outcomes (9). Nonetheless, the influence of established comorbidities or of psychological symptoms on the burden of primary headaches remains poorly studied in children. Clinical (10–13) and populational studies (14,15) suggest that, relative to children without headaches, those with migraine are more likely to have somatic, anxiety and depressive symptoms. Limited findings also suggest that pediatric migraine is associated with impaired attention span (15) and hyperactivity-impulsivity (16), but not with fully developed attention deficit and hyperactivity disorder (ADHD) (16). The subject is less studied for the other primary headaches.
Although the association between primary headaches and behavioral symptoms is well studied, significant gaps exist. First, most studies focused on migraine or tension-type headache (TTH) in isolation, and contrasts between migraine and TTH are less common. Second, most studies either excluded probable diagnosis (probable migraine or probable TTH) or pooled probable diagnoses together with full diagnoses. Third, studies assessed symptoms as a function of presence or absence of specific headache diagnoses without accounting for headache frequency, and this is a major data gap, since chronic pain is per se associated with psychological symptoms (17). Accordingly, herein we investigated behavior and emotional symptoms as a function of headache status and of headache frequency in children.
Methods
Overview
This study was conducted as part of a large ongoing population study aiming to investigate mental health and headaches in children and adolescents (Attention-Brazil Project) (18). We targeted all children from 5 to 12 years of age registered in the public school system of a city (Santa Cruz das Palmeiras, São Paulo) in the year 2009. Mothers/caregivers and teachers were directly interviewed. Children from both urban and rural areas were assessed, as long as they were enrolled in the school system (which is mandatory). Consent forms and analyzable data (complete demographic, mental health and headache information) were obtained from 1856 children (92.5%). The very high participation rate is explained by the active engagement of the city authorities in raising awareness about the study (see below).
Study flow
During the planning period for the 2009 school year (month of February), all teachers in the public school system were trained by one of us (MAA). They were given information about the study and educated about how to teach the parents to complete the headache questionnaire (see below). This was seen as a mandatory step, since many mothers had little or no formal education. The teachers received information on how to explain specific questions in lay terms and received a glossary of lay definitions. They were trained about being neutral and non-judgmental. Parents were then invited to attend a meeting at school (during the first week of the school year) and, under the supervision of the teachers, completed the questionnaire. Meanwhile, children remained with monitors, practicing physical activities.
Questionnaires
Mothers were requested to complete the questionnaire on demographic, mental health and headache information about the children, as well as headache information about themselves.
Headache diagnosis
The headache module of the questionnaire consisted of 14 questions assessing the distinguishing features required for headache diagnosis in the children according to the classification criteria of the second edition of the International Classification of Headache Disorders (ICHD-II) (19). The headache module is the validated Portuguese version (19) of the questionnaire used in the American Migraine Prevalence and Prevention Studies (20), which has been extensively used in the adult and pediatric population (16,21,22), although not for children younger than 10 years of age (see discussion regarding limitations). The logic used to assign a diagnosis followed two basic rules: (1) a full diagnosis (migraine and TTH) trumped a probable diagnosis (probable migraine and probable TTH) and (2) only one diagnosis was assigned (since questions were asked about the most severe headache type only). Accordingly, TTH refers to children endorsing TTH but not migraine criteria. “No headaches” refers to children without primary headaches (23).
The following primary headaches of interest were considered: migraine overall (migraine with and without aura plus probable migraine plus chronic migraine), episodic migraine (episodic migraine with and without aura), TTH overall (frequent and infrequent episodic TTH plus probable TTH plus chronic TTH) and episodic TTH (frequent and infrequent episodic TTH).
Behavior and emotional symptoms
The Child Behavior Checklist (CBCL) was developed for the assessment of competencies and psychopathological symptoms in children (20). The CBCL has been translated into more than 60 languages and has been validated in numerous cross-cultural studies (21).
The validated Brazilian version of the CCCL (CBCL/4–18) (22) was applied. The competency score of the CBCL consists of 20 questions concerning school achievement, social and activity scores. From these three scales, a total competency score is obtained. The behavior and emotional symptoms score consists of 112 questions focusing on the previous six months, which determine eight symptom scales: “Withdrawn,” “Somatic complaints,” “Anxious/Depressed,” “Social problems,” “Thought problems,” “Attention problems,” “Rule-breaking behavior” and “Aggressive behavior.” A ninth scale focusing on “Sexual problems” was not included. Two composite scales, Internalizing and Externalizing, were determined. The Internalizing scale comprises the “Withdrawn,” “Somatic complaints” and “Anxious/Depressed” scales. The Externalizing scale is composed by the “Rule-breaking” and “Aggressive” behaviors scales. The sum of scores of all scales defines the Total Problem Score. For each scale, cut-scores establish “clinically relevant” symptoms. The cut-scores were determined in the validation process of the CBCL by age and gender, and were adopted by us as recommended in the CBCL manual. For the Total Problem Score, the cut-score is 70 (20).
Analyses
Race and income were categorized according to the definitions proposed by the Brazilian Institute of Geography and Statistics (IBGE), which are adopted by the National Census. Race was dichotomized into white and non-white, which included black and brown. The five income classes were defined based on total family income, and do not reflect quintiles. They are determined based on the buying power for a basket of products and services that is defined by the institute and that correlates with socioeconomic characteristics. Classes A and B represent the upper economic classes, D and E describe different levels of poverty, and C is the middle class.
The sample was stratified by age, gender, race, income class and headache status, and 95% confidence intervals (CIs) compared specific categories (e.g. age categories or race) with the reference category. Relative risks (RR) was used to contrast children with migraine and TTH relative to controls on the different CBCL scales. The overall CBCL score and the scores for the individual scales were dichotomized (normal or abnormal, based on the pre-defined CBCL cut-off). They were independently modeled in binary logistic regression as a function of headache status, adjusted by age, gender, race and income. A second model also included headache frequency, categorized as low frequency (1–4 headache days per month), intermediate frequency (5–9) and high frequency (10 or more), as per previous studies (23). The headache questionnaire asked about headache frequency using the same categories (not as a continuous variable).
The level of significance adopted was p < 0.05. Statistical analysis was performed with the aid of SPSS 15.0 for Windows (SPSS Inc, Chicago IL, USA).
Investigation review board approval
This study and surveys received full approval from the Human Research Committee (São José do Rio Preto Medical School, São Paulo, Brazil). Written informed consent was obtained from the mothers.
Results
Overview
Demographic of the sample and response rates.

Prevalence of headaches
Prevalence of headache, migraine and tension-type headache by age, gender, race and income.
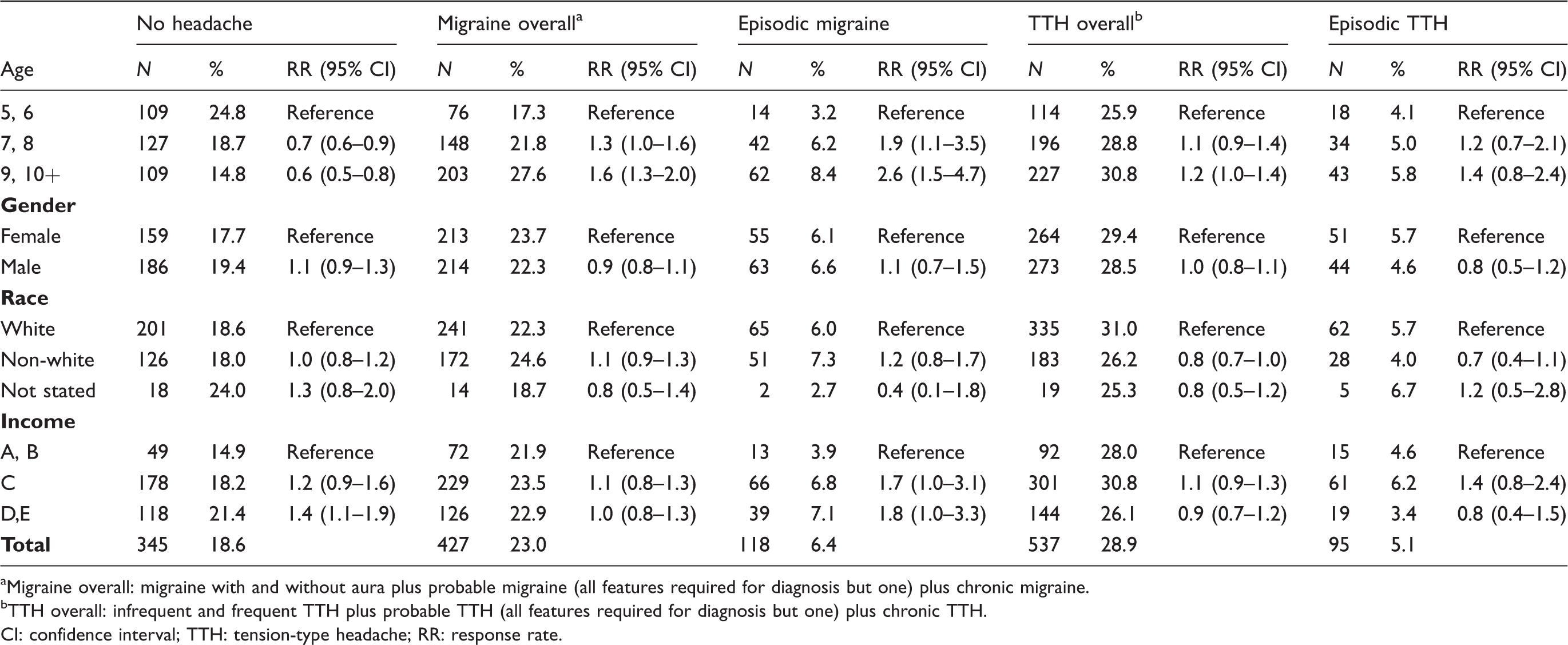
Migraine overall: migraine with and without aura plus probable migraine (all features required for diagnosis but one) plus chronic migraine.
TTH overall: infrequent and frequent TTH plus probable TTH (all features required for diagnosis but one) plus chronic TTH.
CI: confidence interval; TTH: tension-type headache; RR: response rate.
Behavior and emotional symptoms as a function of headache diagnosis
Prevalence of clinical impairment in different CBCL symptoms scales between children with migraine, TTH and controls.

Migraine overall: migraine with and without aura plus probable migraine (all features required for diagnosis but one) plus chronic migraine.
TTH overall: infrequent and frequent TTH plus probable TTH (all features required for diagnosis but one) plus chronic TTH.
CI: confidence interval; TTH: tension-type headache; RR: response rate.
Children with TTH overall were significantly more likely to have abnormal clinical scores in the following domains: somatic (8.8% vs. 2.9%, p < 0.05), anxious-depressed (7.4% vs. 3.5%, p < 0.05), attention (10.2% vs. 6.4%, p < 0.05), internalizing (37.2% vs. 19.1%, p < 0.05) and total score (23.5% vs. 14.5%, p < 0.05), and a similar pattern was seen for episodic TTH (Table 3).
Relative to children with episodic TTH, children with episodic migraine were significantly more likely to have abnormalities in the following domains: somatic (26.3% vs. 10.5%, p < 0.05), anxiety-depressive (20.3% vs. 10.5%, p < 0.05) and internalizing symptoms (56.8% vs. 40.0%, p < 0.05).
Multivariate analyses
Multivariate analyses of determinants of CBCL symptoms scales in children with migraine and in children with TTH.

Model 1: gender, race, age and, income class.
Model 2: gender, race, age, income class, and headache frequency.
NS: non-significant.
Frequency had a clear influence on CBCL scores of migraineurs (Table 4). After adjustments for headache frequency, children with migraine were more likely than controls to have a clinically relevant abnormal total CBCL score, as well as abnormalities in somatic, anxious-depressed, social, attention, aggressive, internalizing (p < 0.001 for all comparisons) and externalizing (p < 0.05) domains. Children with TTH, in turn, were more likely than controls to have clinically relevant abnormal scores in somatic (p < 0.01), anxious-depressed (p < 0.05) and internalizing symptoms (p < 0.05).
Discussion
Pediatric headaches impact quality of life (2) and school attendance (3,25), and seem to be associated with behavioral, emotional, and social problems and competencies (13,14). To the best of our knowledge, the present study is the first study to examine the behavior and emotional correlates of migraine and TTH in young children using the ICHD-II criteria and the CBCL questionnaire and accounting for headache frequency in a large community-based study. Our findings can be summarized as follows: (1) relative to controls, children with migraine are more likely to have symptoms in several domains and to have clinically abnormal total CBCL scores; (2) children with TTH have impairments in the same domains seen in those with migraine, but with lower magnitude; (3) in children with migraine and with TTH, impairments significantly vary as a function of headache frequency.
Our findings corroborate the higher prevalence of somatic and anxiety-depressive symptoms in children with migraine and TTH compared to those without headache. Previous populational studies have also showed the higher prevalence of somatic (14,26) and anxiety-depressive symptoms (15,27) in children and adolescents with migraine compared to children without chronic headaches, although controversial findings are reported concerning children with TTH (14,26).
As previously reported by others (14), we found that migraine was associated with social problems but not with “rule-breaking” and/or “aggressive’ symptoms (externalizing behavior problems). The “social” domain identifies difficulties in social engagement as well as infantilized behavior for the age and this may be associated with an important impact on personal and social life. Social isolation is, in turn, associated with anxiety and depression, with the potential for a self-perpetuating association. Providers should be aware of this possibility in children with migraine, in order to properly address the problem. We found no evidence of differences in withdrawn (shy behavior), thought (delusions and obsessive–compulsive behavior) and externalizing (“rule-breaking” and “aggressive” behaviors) scales.
Two previous population studies suggest that migraine (but not TTH) and chronic daily headaches are associated with inattention (15,28), hyperactivity (28) and other behavioral problems. Here we found abnormal scores in the CBCL attention domain. However, in a separate study using the Swanson, Nolan, and Pelham scale version IV (MTA SNAP-IV), which is DSM-IV-based and validated to identify specific symptoms of ADHD, we found that, in multivariate analyses, ADHD or inattention symptoms were not predicted by headache subtypes or headache frequency, but hyperactivity-impulsivity symptoms were significantly associated with any headache (p < 0.01), tension-type headache (p < 0.01) or migraine headaches (p < 0.001) (16).
To explain this discrepancy, we highlight that of the 11 questions that encompass the CBCL domain for attention, only three indeed capture this domain, and only one seems to truly focus on attention. The remaining questions focus on hyperactivity, impulsivity, executive dysfunctions and lack of coordination (20). The specificity of the scale to measure attention can therefore be questioned, since it seems to be a composite metric.
The influence of headache frequency on the behavior of children with migraine and other primary headaches is still poorly understood. In a recent study we explored the influence of maternal headache frequency on the CBCL scores of their children (29). In multivariate analyses, we found that, in children with migraine, maternal migraine status and maternal headache frequency did not predict CBCL scores in children with migraine but did predict them in children without migraine (p < 0.01). Our current results add to the picture by suggesting the relevance of probands headache frequency, and highlighting that the burden of migraine on the family is complex. Taken together it seems that children with migraine are more likely to have behavioral and emotional symptoms than children without migraine, and that this is influenced by their headache frequency but not by their mother's headache status or headache frequency. Children with TTH follow the same pattern of children with migraine, but are less severely impacted. Children without migraine may be affected, in turn, by frequent headaches experienced by their mothers (29).
The strengths and limitations of our study deserve comment. Among the strengths we list the relatively large sample size of young children, the use of validated questionnaires, the help of trained facilitators (teachers) and the strict following of standardized criteria for diagnosis, as well as the very high participation rate.
Among the limitations, we first highlight that headache diagnosis was determined by the information provided by the mother; and that no direct interviews were conducted with the children, raising the potential for unavoidable biases. Mothers could fail to report existent migraine symptoms from their children or could, alternatively, have a distorted perception (reporting them as more severe than they were) of the symptoms. However, it was necessary to obtain the information from the mothers, as the patient group was too young to properly understand the questions. Nonetheless, this is not different from what is often seen in medical practice for young children, and potential biases of our method need to be explored (30). Second, we underestimated the prevalence of TTH, as we classified only the most severe type of headache presented by patients. This is a standard method in the field (31), but because we did not assess more than one type of headache, we cannot adjust for whether one headache (TTH) influences the association of headache/CBCL in children with another (migraine).
Finally, our most important limitation involved the questionnaire used, which has been validated for children 10 years or older, not for younger children. This is a limitation not only of our study, but to virtually all studies in the field where medical diagnosis has been done. Nonetheless, a random sample of 100 children was seen by one of us (MAA) and sensitivity was above 90%, with specificity above 75% for the four diagnoses of interest. The process of validation is currently being written for publication. Nonetheless, because the questionnaire basically presents the ICHD diagnostic criteria, and because we interviewed the mothers, we are confident that major biases are excluded.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
This study was conducted without commercial financial support. Dr Bigal is a full-time employee of Merck Inc. He owns Merck stocks and stock options. Merck did not sponsor this study. Dr Arruda reports no disclosures.