
Abstract
The aim of the present study was to assess the distribution and characteristics of headache in children aged 7-14 years in Lower Saxony (Germany). For the survey, 8800 households with children were randomly drawn from community registers. Parents received comprehensive questionnaires regarding various aspects of their child's headache history and general health by mail. The response rate was 63.5%. The 6-month prevalence of paediatric headache was 53.2% and increased with age (39% at 7 years to 63% at age 14). Overall, recurrent headache (≥/week) was experienced by 6.5% of the total sample and was significantly more common among older girls (≥11 years) than their male counterparts. Boys and girls did not differ markedly from one another regarding headache occurrence and frequency until the age of 11. Mean age of headache onset was 7.5 years, with onset occurring at a significantly younger age among boys than among girls. In accordance with International Classification of Headache Disorders-II criteria, migraine was diagnosed in 7.5% and tension-type headache in 18.5% of the cases, hence a large proportion of the children had unclassifiable headache. Of the headache disorders, migraine was rated the most disabling, with the highest average intensity, highest frequency, duration of headache often exceeding 2 h and more frequent use of medication. In general, aura symptoms were rare except for visual disturbances (17%). Paediatric headache was strongly associated with other health problems, including other pain symptoms. Paediatric headache was also associated with a history of parental headache.
Introduction
In adults headache is one of the most debilitating pain syndromes if it occurs frequently or becomes a chronic condition (1). High-intensity and disabling concomitants such as nausea, vomiting or sensory hypersensitivity contribute to headache's negative impact on the individual. High healthcare costs are the result of recurrent or chronic headache (2, 3).
An early study by Bille (4) first directed attention to paediatric headache, especially migraine. It showed that headache onset can occur even in early childhood and that headache is common among children and adolescents. Longitudinal data from the same sample (5) revealed that over 50% of individuals with a history of childhood migraine continued to experience it 30 years later. Fearon and Hotopf (6) found children with recurrent headache to be not only more likely to experience headache in adulthood, but also to develop multiple physical symptoms and psychosomatic morbidity. Sillanpää (7) and Sillanpää and Anttila (8) conducted two of the most comprehensive epidemiological surveys on paediatric headache in Finnish children from the age of 7–14 years. The two studies, which utilized identical methodology, indicate that the prevalence of headache among 7-year-olds had doubled within a time span of two decades. More recent studies have documented that headache can be a serious health problem in children, resulting in a reduction of quality of life (9–12).
The main aim of the current study was to provide detailed information about the distribution and characteristics of headache in a German population-based sample and to compare these data with findings of recent epidemiological studies from other countries.
Methods
Procedure
Eight thousand eight hundred families were randomly drawn from community registries of four districts in southern Lower Saxony and the city of Hannover (Lower Saxony, Germany), thus including both urban and rural communities. The postal survey was conducted in winter 2003/2004.
The survey procedure was conducted in accordance with the recommendations of Dillmann (13). Following a prenotice letter, informing the household of the upcoming survey, parental questionnaires were mailed out to the randomly selected households. A child questionnaire was included for those households with a child aged ≥9 years. The child questionnaires, however, are not part of the current analysis. A postcard thanking responders for their participation and requesting the remaining subjects to complete and return the questionnaire(s) was mailed a week later. Two weeks following this postcard, all non-responders were sent replacement questionnaires. A lottery, in which responders had a chance to win prizes (e.g. gift certificates for books), was implemented as an incentive for participation.
Questionnaire development
Prior to the survey, the questionnaire was rigorously pretested. As a first step, experts in empirical psycho-social research reviewed the first draft of the questionnaire with regard to comprehensibility and adequacy of response categories. On the basis of this feedback, a number of questions and items were modified. As a second step, 10 families with children in the targeted age range completed the questionnaire in the presence of one of the authors. Retrospective interviews were then conducted in order to identify potential questionnaire-related difficulties and to assess acceptance of survey material (comprehensibility, layout, etc.). This procedure led to a second modification of the questionnaire. In the third step, a sample of 100 households (randomly selected from the community registry of the city of Göttingen) received the questionnaire by mail. In this pretest sample a response rate of 82% was achieved. Questionnaire items were analysed with regard to missing values and response consistency. A number of items were modified or eliminated as a result. The final version of the parents' questionnaire consisted of 28 pages with 111 questions.
The conduct of the study was approved by the Ethics Committee of the German Association of Psychology. Data safety procedures were approved by the University of Göttingen data protection officer.
Statistical procedures and data analysis
Sample size calculation took prevalence rates reported in prior studies and an expected non-response rate of 40% into account in order to ensure a sufficient number of responders, especially in specific categories of interest (e.g. different age groups, or children with recurrent headache). For the younger children (7–10-year-olds) 1200 households per age group were determined necessary, for the older children (11–14-year-olds) 1000 households per age group, since headache prevalence was expected to increase with age. Before conducting statistical analyses (SPSS version 12; SPSS Inc., Chicago, IL, USA) the data were checked for correct entry. A further procedure assured that the questionnaire referred to the intended child and that >50% of the items were answered, otherwise the respective case was eliminated.
A random set of non-responders (n = 199) were contacted via telephone in order to determine whether a non-response bias was present in the study sample. The data revealed significant differences in response rates depending on children's headache status: among non-responders the proportion of children without headache was substantially larger than among responders (64.3% vs. 46.8%).
Distributions were statistically examined using χ2 tests, tests for differences between groups (t-tests, analysis of variance) and rank correlation. The level of significance was set at P ≤ 0.05.
Results
Study sample
A total of 5586 households returned the parental questionnaire, thus yielding a response rate of 63.5% (Fig. 1). Valid data were received from 62.2% of the sample. Almost exactly half (50.6%) of the responding households reported data on a male child.
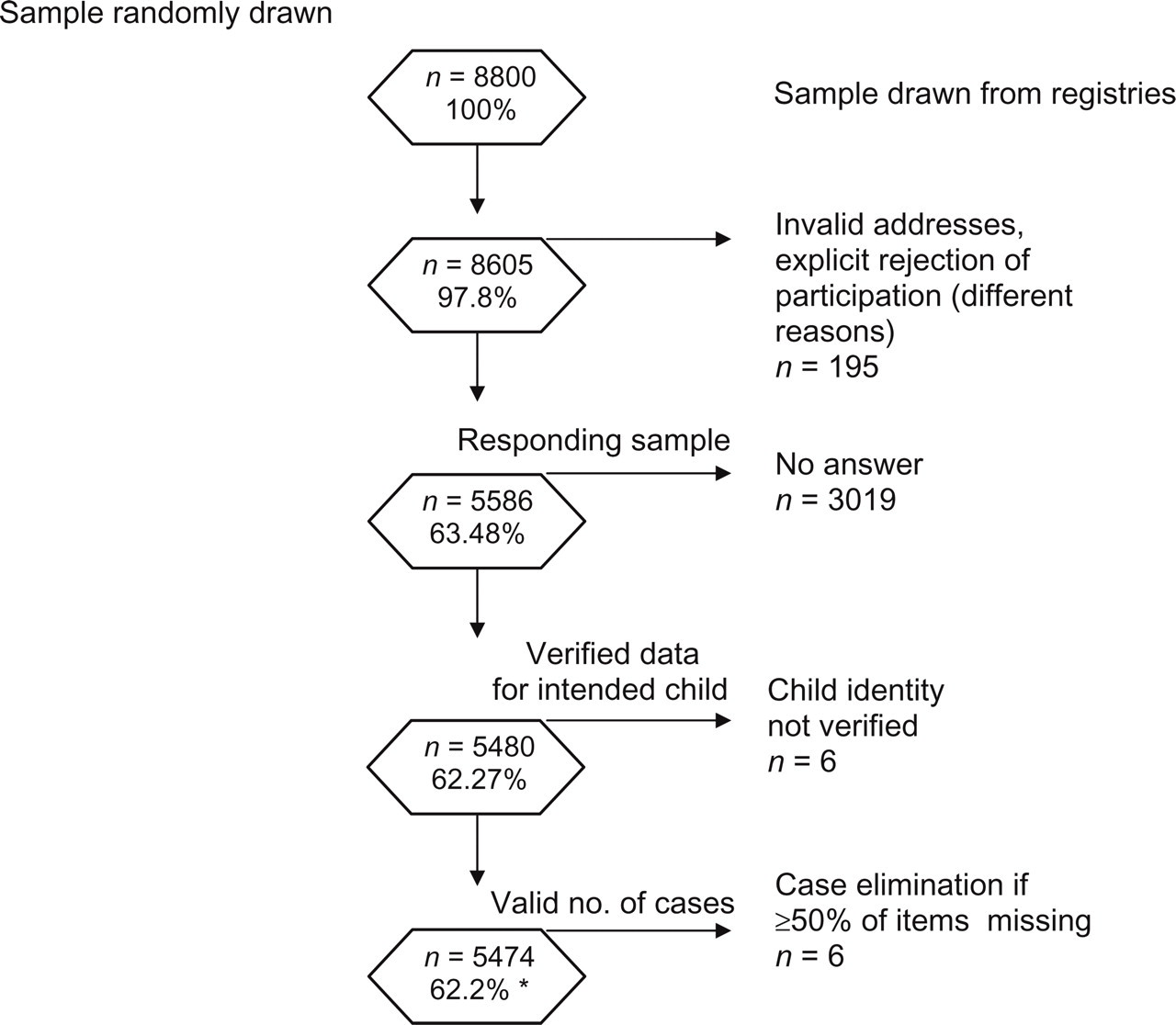
Study sample.
Socioeconomic status (14) was uneven among the study responders, with 7.5% of the households belonging to the lower class, 47.3% to the middle and 45.2% to the upper class.
The parental questionnaires were completed in most cases by the child's mother (74.4%).
Headache occurrence, frequency and age at onset
The frequency of headache was retrospectively assessed for the period of the last 6 months. Over half of the children, 52% of boys and 55% of girls, experienced headache at least once during this time. The gender difference is significant (χ2(1) = 4.03, P = 0.045; Fig. 2a,b).

(a) Distribution of headache frequency × age (female). (b) Distribution of headache frequency × age (male).
The prevalence of any headache increased from 38.6% in 7–8-year-olds to 63.4% in 13–14-year-olds (χ2(3) = 37.51, P ≤ 0.0001). The prevalence of recurrent headache (≥1/week) increased almost threefold with age, from 2.6% in the youngest to 9.8% in the oldest age group (Fig. 2a,b) (χ2(3) = 72.16, P ≤ 0.0001). It became evident that when children were older (≥11 years) girls were distinctly more often afflicted with headache, especially with monthly or weekly episodes (frequency × gender total sample: χ2(3) = 28.82, P ≤ 0.0001; 7- and 8-year-olds, χ2(3) = 1.66, NS; 13- and 14-year-olds, χ2(3) = 22.62, P ≤ 0.0001).
The distribution of socioeconomic status (SES) categories showed no systematic relationship to headache prevalence (χ2(2) = 4.88, P = 0.09). Headache was more common in children living in single-parent households (59.7% vs. 51.9%; χ2(2) = 17.7, P ≤ 0.0001).
The mean age of headache onset was 7.5 years (SD = 2.53). Regarding type of headache, migraine had the earliest (7.1 years) and tension-type headache (TTH) the latest onset (7.9 years; F 2,1704 = 11.68, P ≤ 0.0001). Boys were significantly younger at onset of headache (7.3 years) than girls (7.8 years; F 1,1705 = 19.93, P ≤ 0.0001). In 5.3% of the children the age reported for onset of headache was in the range of 1–3 years.
Type of headache
Of the total sample, 5.4% to 7.5% of children experienced migraine according to the criteria of the International Classification of Headache Disorders (ICHD) I (15) or II (38), respectively, when all criteria except A (number attacks ≥5) and E (headache not attributed to another disorder) are considered; 18.5% suffered from TTH and about 27% were unclassifiable. There were no significant differences between girls and boys regarding type of headache (all tests: χ2(2) = 1.23, NS). The prevalence of migraine increased with age (Fig. 3a,b) (3.5–10.8%; χ2(3) = 21.70, P ≤ 0.0001). There were also differences in the occurrence of TTH between age groups (χ2(3) = 18.26, P ≤ 0.0001). In migraine, the percentage of children with recurrent headache (≥1/week: 18.5%) was the largest compared with TTH (8.5%) and unclassifiable headache (UCH) (13%) (diagnosis × frequency: χ2(4) = 101.8, P ≤ 0.0001).

(a) Distribution of headache diagnosis × age (female). (b) Distribution of headache diagnosis × age (male).
Intensity and duration of headache and further symptoms
Average headache intensity was reported to be 4.0 (SD = 1.78) on an 11-point rating scale ranging from 0 to 10. Intensity correlated positively with frequency of headache (Spearman's ρ = 0.27, P ≤ 0.0001; F 2,2611 = 97.63, P ≤ 0.0001; t-tests: significant differences between each frequency category, P = 0.0001).
Headache intensity was greatest in migraine (5.9 ± 1.61) and lowest in TTH (2.91 ± 1.17) (F 2,2611 = 640.11, P ≤ 0.0001; all t-tests: P ≤ 0.0001). Mean intensity was slightly higher in boys than in girls (mean = 4.04/3.89; SD = 1.83/1.74; F 1,2612 = 4.68, P = 0.031) and increased with age (F 3,2610 = 11.72, P ≤ 0.0001).
A third of the children with headache (30.8%) experienced headache episodes of 1–2 h duration, 28% had even shorter attacks. A higher percentage of migraineurs (72.6%) experienced longer episodes of headache (≥2 h) compared with children with TTH (25.7%).
Aura symptoms were rare even in headache diagnosed as migraine (Table 1). The most frequently reported features of migraine were aggravation by physical activities, phonophobia and photophobia. Unilaterality of pain was uncommon even in migraine (21%). In general, UCH showed more correlating symptoms than TTH.
Headache correlates and aura symptoms in different diagnoses
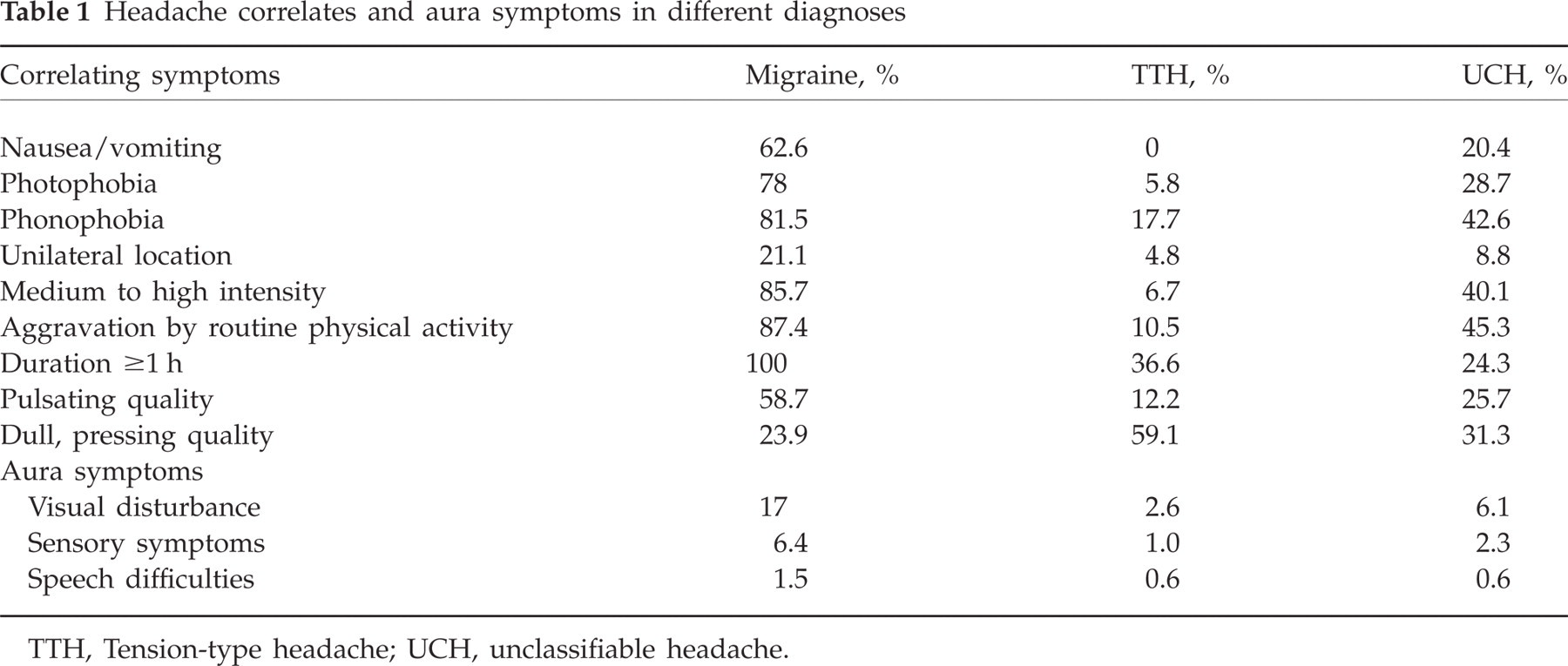
TTH, Tension-type headache; UCH, unclassifiable headache.
Medical consultations and medication
Only about one-third of the children (31.1%) with a history of headache in the last 6 months had consulted a physician with regard to headache, a very small percentage (14.5%) had seen at least two different physicians. The more frequent the child's headache, the more common it was to consult a doctor (χ2(4) = 270.52, P ≤ 0.0001). Children with recurrent headache had consulted at least one physician in 57.7% of cases. Consultation was also dependent on type of headache, with migraine being the headache disorder most commonly associated with multiple consultations (33.4%), followed by UCH (14.0%) and TTH (7.6%; χ2(4) = 222.97, P ≤ 0.0001).
Analgesics or antimigraine medication were taken by 54.5% of the children with headache, with no significant difference between girls and boys (χ2(1) = 3.22, P = 0.073). The number of children taking these drugs increased markedly from 38.7% in 7–8-year-olds to 70.2% in 13–14-year-olds (χ2(3) = 158.98, P ≤ 0.0001). With increasing frequency of headache the percentage of children consuming these kinds of drugs increased (less than monthly headache, 47.6%; weekly headache, 65.3%; χ2(2) = 68.16, P ≤ 0.0001). Of children with migraine, 83.6% used analgesics or antimigraine drugs, whereas only 40.1% of those with TTH and 56.3% with UCH made use of it (χ2(2) = 220.2, P ≤ 0.0001).
Preventive medication was used in only 6.2% of cases. Again, the consumption of preventive medication became more common with increasing frequency of headache (4.4–11.7%, χ2(2) = 27.69, P ≤ 0.0001) and from the youngest to the oldest age group (3.57–9.34%, χ2(3) = 19.741, P ≤ 0.0001). There were also differences between diagnostic groups in the use of preventive medication (χ2(2) = 10.68, P ≤ 0.005) (migraine 9.4%, TTH 4.7%, UCH 6.4%).
Interference due to headache
Three items (complete school days lost, complete inability to do homework or chores at home, complete inability to engage in social activities) were used to calculate a global interference score. It did not differ between girls and boys (F1,2674 = 0.01, P = 0.91) or between age groups (F3,2672 = 12.24, P = 0.0001). Children with weekly headache showed the highest amount of interference (F2,2673 = 148.64, P = 0.0001). Migraine (4.79 ± 6.84) was characterized as the most interfering headache disorder (TTH 0.87 ± 2.38, UCH 1.91 ± 3.76) (F2,2673 = 132.29, P ≤ 0.0001). The difference between headache diagnoses remained significant even when controlling for headache frequency (F5,2670 = 118.8, P ≤ 0.0001). With regard to the three areas of functioning, the reported interference was higher regarding homework and chores (0.87 ± 2.09) than for school activities (0.30 ± 1.25) (F 2,2546 = 104.4, P ≤ 0.0001).
Headache and other health problems
The distribution analysis shows a close relationship between headache frequency and other pain problems, such as abdominal and back pain (Fig. 4) (χ2(9) = 699.82, P ≤ 0.0001). Additional pain problems were more common among children with migraine than children with other headache types (χ2 = 21.07, d.f. = 6, P = 0.002).
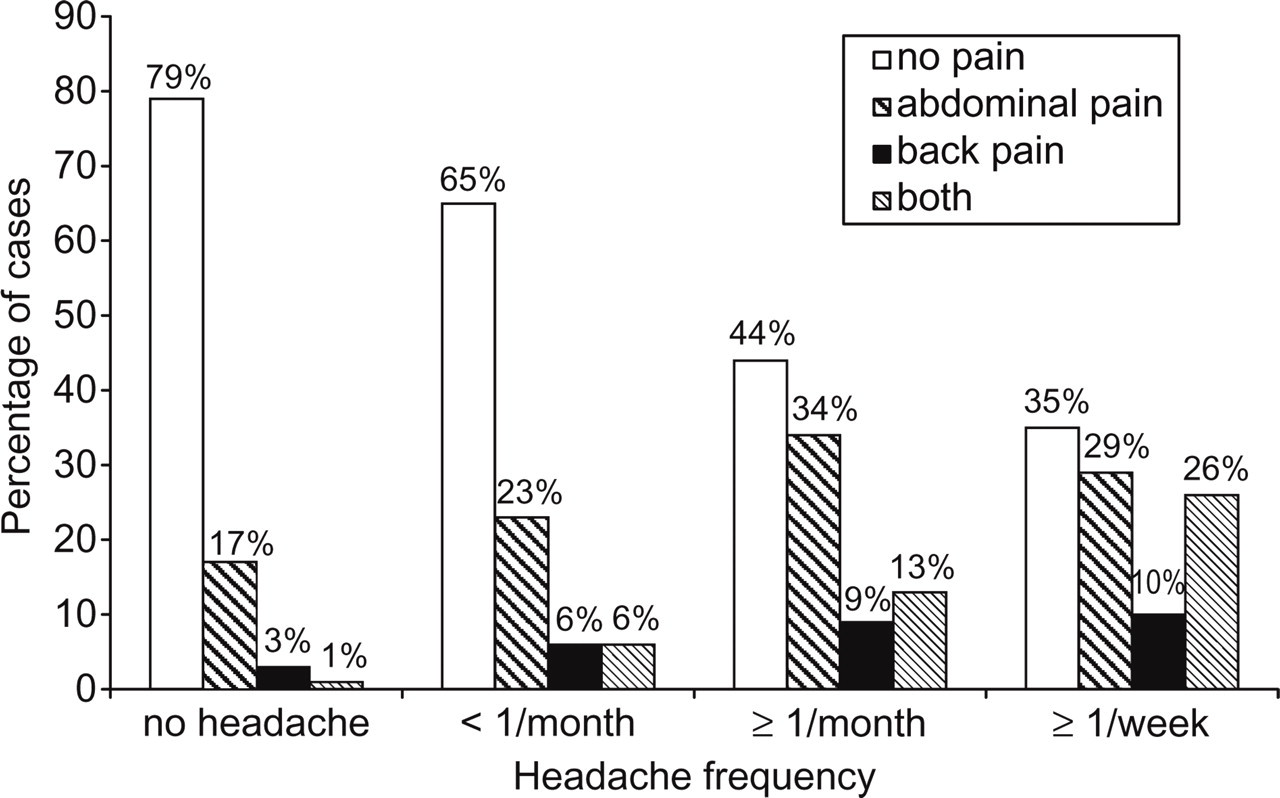
Association of headache with other pain complaints.
There was also a close association between headache frequency and the number of other physical complaints (excluding pain) (Spearman's ρ = 0.28, P ≤ 0.0001).
Also, children with headache were reported to have significantly more chronic diseases (no headache, 0.34 ± 0.64; headache, 0.48 ± 0.76; F 3,5393 = 49.99, P ≤ 0.0001).
Parents' and children's headache
There was a strong association between pain in parents and headache in children. If a biological parent (in most cases the mother) experienced headaches, 72.3% of the children did so also. If parents were not afflicted by headache, then only 27.7% of the children suffered from it (χ2(1) = 372.50, P ≤ 0.0001).
Discussion
Headache prevalence related to gender and age
The 6-month prevalence of headache in our population-based sample of 53% is much lower than that of 89.8% reported by Pothmann et al. (17) in his early study of German schoolchildren, only slightly older than our sample. Assuming an actual decrease of headache from 1994 to 2004 would disregard the results of Sillanpäa and Anttila (8), who reported a remarkable increase within two decades. We rather attribute it to differences in methodology. The early German study relied on self-report data of the children, whereas our data are based on the parents' report. Some studies show parents tend to underestimate their children's pain (or children overestimate their pain) (e.g. (18, 19)). Whereas in the earlier study lifetime prevalence was asked for, we asked for the 6-month prevalence. However, there is not much difference between a 12-month and lifetime prevalence in children, as Barea et al. (20) were able to demonstrate (82.9% vs. 93.2%). Thus, the type of prevalence assessed alone does not explain the discrepancy of >30% between the two studies. Recent data from German surveys reported by Roth-Isigkeit (21) (prevalence 65.6%) and Ravens-Sieberer et al. (22) (prevalence 55.4%), however, support the validity of our results, as do prevalence figures lying in a comparable range reported from other countries (23).
The survey clearly demonstrates a marked increase of headache occurrence over the age range. An age effect was found in nearly every recent and older study (24–27).
Headache was relatively evenly distributed among boys and girls, when looking at the sample as a whole. We found, however, an interaction of gender and age, with the older girls experiencing headache more often than the boys, especially recurrent headaches. The majority of studies have found an overall higher prevalence of headache in girls (17, 25, 27–32), whereas others (33, 34) have not. Data from Sillanpää and Aro (31) and Laurell et al. (25) support our finding that with increasing age the gap between boys and girls in the occurrence of headache increases. The vulnerable period for girls begins at the age of 11, when a considerable percentage of them develop frequent or recurrent headache.
Especially in older girls, a high proportion (13%) of children were afflicted by frequent headache (≥1/week). This is a high percentage of children faced with a reduced quality of life, which is shown by higher disability scores. The group of children with recurrent headache is also predisposed to chronic headache in their adult life (35). Nevertheless, these prevalence rates are in contrast to much higher figures reported by older studies (36–38). Recent studies from Laurell et al. (25) (children aged 7–15), Zwart et al. (32) (adolescents aged 12–19) and Rhee (30) (11–22-year-olds) have also reported prevalence rates in excess of 20% for recurrent headache. While the differing age range (including adolescents >14 years old) and the source of data (children) might explain some of the differences in prevalence rates, the discrepancies cannot be explained satisfactorily. Our impression from clinical work with paediatric headache patients seeking treatment, however, does not support the assumption of a prevalence of weekly headache in the order of 20–25% of the total paediatric population.
Types of headache and headache features
The ICHD I and II differ with regard to the minimum duration of a headache episode ((15), >2 h; (38), ≥1 h). The criteria of both classifications were assessed by our questionnaire with the exception of quantifying the number of attacks with the specific pattern of symptoms. Also, differentiation between primary and secondary headache was not possible since questions regarding symptoms were aimed at the ‘typical’ headache and a medical diagnosis was not made independently. It was also impossible to assess the coexistence of two types of headache in a child. Thus, if the assessable criteria for migraine were fulfilled, a TTH diagnosis was excluded. If the symptoms did not correspond to the criteria of either migraine or TTH, headache was characterized as unclassifiable (about 50%), including single or very rare headaches, which might have been caused by illness. This high percentage may reflect both the deficit of a diagnosis based solely on questionnaire data and the less distinctive differentiation between primary headache types in children.
The overall prevalence of migraine was 5.4% according to the old and 7.5% according the new system. Thus the more liberal classification does not excessively inflate the number of children with migraine, but includes a considerable percentage of those who otherwise would have been categorized as non-classifiable on the basis of the shorter duration of the average attack.
The prevalence of migraine increases with age by about 7%, whereas the gradient of increase of TTH is not linear and not as steep. In our study the distribution of headache diagnoses did not differ with gender, a finding which is in contrast to a meta-analysis by Scher et al. (39), who found migraine to be more prevalent among girls. Less pronounced gender differences, lying in the range of our study, have recently been reported in other studies (24, 25, 33). Overall, reported prevalence rates for migraine are relatively heterogeneous, with estimates from 5.4% to 14% (27, 31, 34).
According to our findings, migraine is the headache disorder with the highest frequency, longest duration, highest intensity and most pronounced disability. It is also associated with more other pain or physical symptoms, a greater likelihood to consult a physician or use medication.
The most characteristic and differentiating symptoms of migraine are aggravation by physical activities, and photo- and phonophobia, which was also reported by Zencir et al. (27) and Bener et al. (33). In our study, aura symptoms were rare except for visual disturbances. The symptom cluster of UCH showed greater similarity to migraine than TTH.
On average, age at onset of headache lies between the ages of 7 and 8 years, with boys experiencing their first episode earlier than girls, and migraine starting earlier than other types of headache. Surprisingly, >5% of the parents reported their child's first headache to have occurred between the ages of 1 and 3 years, when it should be difficult for children to verbalize their pain.
Pain proneness and vulnerability
The high covariance of different ‘pains’ (head, abdomen, back) is noteworthy and concurs with recent data from Aromaa et al. (40) and Fichtel and Larsson (41). One-quarter of all children with recurrent headache experience pain in the abdomen and back, which is a higher proportion than that reported by Groholt et al. (28). Pain proneness seems to be an adequate term for the description of this finding. Headache is also significantly related to other physical symptoms and chronic disease. Thus pain proneness is associated with general vulnerability.
This clustering of health-related complaints should be taken into consideration in future epidemiological studies, especially regarding risk factor analysis.
Findings indicating that children are more likely to experience headache if there is a history of parental headache (e.g. (27, 33)) are corroborated by our study.
Treating headache
The data on headache-related medical consultations suggest that paediatric headache is not considered by parents to be a serious illness. Hence, <60% of children with recurrent headache have consulted a physician. Although this could be interpreted as health behaviour (relying on the child's own ability to cope with the problem), it may, on the other hand, be interpreted as an impediment to enter a treatment which may effectively reduce the child's distress and suffering. Many parents are concerned about unwanted side-effects of medication-based treatment, at least in younger children. However, headache treatment in children need not necessarily be pharmacological. The meta-analyses by Eccleston et al. (42) and Trautmann et al. (43) underline the preventive efficacy of psychological treatment of children with headache. The substantial increase in using abortive medication from 7 to 14 years suggests that non-pharmacological means of preventing headache should be encouraged.
Assessing interference
Headache-related interference with activities manifests itself more often in inability to do homework or chores than in absence from school. Our data indicate that headache-related interference is more pronounced among children with frequent headache, migraine and of older age. Because of the covariance of these variables, only multivariate regression analysis can yield information on the relative weight of these factors.
Limitations
The achieved response rate of >62% valid questionnaires in a postal survey is not satisfying, but comparable to another recent study on children's pain (28) with a similar design (population-based study, postal survey, parent questionnaire). These and other findings reflect the trend for declining participation in epidemiological studies, at least in western countries (44).
There is no indication that the region selected for recruiting (Lower Saxony) deviates markedly from other German areas in relation to headache-relevant factors. Considering the large number of families recruited (randomly selected from community registries), the procedure should result in a representative selection of families with children between 7 and 14 years of age of German nationality. Neither assumption, however, can be substantiated since reference data for the population are not available.
However, two factors might have led to sample bias. The majority of the 199 non-responders who were contacted via telephone were parents of children without headache, indeed there were 18% more headache-free children than in the total responder sample. This could have resulted in an overestimation of headache prevalence. No covariation between headache occurrence and SES was found, hence bias because of the overrepresentation of upper and middle class households is unlikely.
The methodological limitations in estimating the prevalence of the different types of headache (migraine, TTH) have already been discussed and are common to all studies with postal surveys.
Acknowledgements
The research project has been supported by a grant from the German Ministry of Education and Research within the German Headache Consortium. We thank Mrs A. Feuersenger, Institute for Medical Informatics, Biometry and Epidemiology (Professor K.-H. Jöckel, University of Duisburg-Essen) for her support regarding case number calculation and the design of the study.